
Abstract
Rationale:
Most of the preterm infants are born between 32 and 36 weeks of gestation (moderate to late preterm infants [MLPIs]). This comes with significant short- and long-term risks. Breastfeeding reduces many of these risks, but breastfeeding rates in MLPIs are lower than those in full-term infants. We performed a systematic review of studies identifying factors associated with successful breastfeeding in MLPIs and interventions to improve breastfeeding.
Methods:
Systematic search performed using PubMed April 24, 2020. In total, 11 articles describing barriers to breastfeeding in MLPIs and 6 articles about interventions to improve breastfeeding were included. Interventions were categorized according to different outcomes: breastfeeding initiation, continuation for 5 days to 6 weeks, and continuation ≥3 months. Because of heterogeneity in study characteristics, no meta-analysis was performed.
Results:
Breastfeeding rates were lower in those with lower socioeconomic status and single-parent households. Providing parents with more information and direct health care support significantly improved breastfeeding initiation. Cup feeding instead of bottle feeding had inconsistent effects on breastfeeding initiation and continuation. Continuous skin-to-skin contact did not affect breastfeeding initiation or continuation.
Discussion:
Risk groups for lower breastfeeding rates of MLPIs include mothers with lower socioeconomic status and single mothers. Interventions that may improve breastfeeding include cup feeding and providing parents with more information and health care support. Key limitations of included studies are lack of adequate adjustment for confounders and lack of blinding. However, this is the first systematic review identifying both risk groups and interventions to improve breastfeeding in MLPIs.
Introduction
Worldwide, 11.1%
Nevertheless, moderate and late prematurity carry their own risks: the relative risk of dying as a moderate preterm infant (MPI) or late preterm infant (LPI) is three to nine times higher than infants born at full term.5,6 Karnati et al. 6 described several short-term complications for LPIs including respiratory problems, hyperbilirubinemia, feeding difficulties, hypoglycemia, temperature instability and cold stress, poor immunological response, and sepsis. Long-term complications consist mainly of neurodevelopmental problems. 6 Finally, MPIs and LPIs are associated with significant medical care costs: McLaurin et al. 7 concluded that preterm infants of 33–37 weeks have three times higher 1- and 5-year costs than term infants. 7
The incidence of these complications can be reduced by feeding breast milk to moderate to late preterm infants (MLPIs) instead of artificial milk formula. Breast milk is a complex, living fluid containing lipids, proteins, antibodies, carbohydrates, cytokines, bacteria, and enzymes,8,9 the composition of which can never be replicated artificially. Compositional ratios differ for each mother-infant dyad: preterm milk, for example, contains significantly more macronutrients than full-term milk. 10 Breast milk is especially important for preterm infants because it contains multiple specific nutrients that impact on brain growth. 11 Hallowell et al. 12 noted that one third of the final brain volume at term corrected age is accrued in the last 5–6 weeks of pregnancy meaning that most MLPIs are born with only 65% of the brain volume of full-term infants. 12 Therefore, it is especially important to support human milk feeding in MLPIs.
Studies show that feeding breast milk instead of formula results in fewer gastrointestinal infections and lower respiratory tract diseases; less acute otitis media; lower blood pressure; lower total cholesterol; less obesity and type 1 and 2 diabetes; lower risk of necrotizing enterocolitis and late-onset sepsis; decreased incidence of childhood leukemia; less pain during procedures; less atopic dermatitis and childhood asthma; better cognitive development in infants; a lower risk of sudden infant death syndrome and a shorter hospital stay.9,13 Breastfeeding can also improve the mother's health: there is a reduced risk of breast cancer, ovarian cancer, type 2 diabetes, and possibly postnatal depression. 9 However, it is unclear whether associations in individuals who are breastfed are solely owing to breast milk or breastfeeding, or whether some of the effect may be owing to residual confounding that influences the mothers' decision to breastfeed, or owing to reverse causation. Nevertheless, there are widespread data that strongly support a biological role of breast milk components in improving a range of longer term health outcomes.
Although studies show that breast milk is especially important for all preterm infants, MLPIs are less likely to be fed breast milk than full-term infants.14–16 Some studies even show that very preterm infants (<32 weeks) are fed human milk more often than LPIs. 15 Therefore, our review specifically investigates the barriers to and interventions for supporting breastfeeding in MLPIs.
There are several maternal and infant factors and characteristics that can form barriers to successful breastfeeding. First of all, although MLPIs may appear relatively mature at birth, they frequently have a weaker suck and poorer suck–swallow–breathe coordination, making breastfeeding more difficult. Furthermore, preterm infants cannot communicate as effectively as term infants, and feeding cues may not be conveyed as clearly to, or acted upon, by their parents. 17 Another challenge is that preterm infants and their mothers are often separated after birth, which negatively affects breast milk production.12,17
Several previous studies on this subject17–19 have tended to focus on extremely preterm infants, 20 although many do not integrate both risk factors for decreased breastfeeding and solutions. The aims of this review are first to investigate which specific barriers interfere with breastfeeding in MLPIs (32–36 weeks) compared with full-term infants (37–42 weeks), and second, what interventions can be implemented to improve breastfeeding success. The population included preterm infants of 32 + 0–36 + 6 weeks and their mothers/parents. A range of interventions that attempt to improve breastfeeding in this gestational age group were anticipated, as was variation in the outcome measures chosen.
Materials and Methods
Information sources and literature search
For this systematic review, articles were retrieved from PubMed. The following search strategy was used: (“moderate preterm”[tiab] OR “moderately preterm”[tiab] OR “late preterm*”[tiab] OR “near term*”[tiab] OR “marginally preterm*”[tiab] OR “marginal preterm*”[tiab] OR “minimally preterm*”[tiab] OR “minimal preterm*”[tiab] OR “mildly preterm*”[tiab] OR “mild preterm*”[tiab] OR “larger preterm*”[tiab] OR “large preterm*”[tiab] OR “moderate premature”[tiab] OR “moderately premature”[tiab] OR “late premature*”[tiab] OR “marginally premature*”[tiab] OR “marginal premature*”[tiab] OR “minimally premature*”[tiab] OR “minimal premature*”[tiab] OR “mildly premature*”[tiab] OR “mild premature*”[tiab] OR “larger premature*”[tiab] OR “large premature*”[tiab]) AND (breast feeding[mesh] OR “breast milk”[tiab] OR breastmilk[tiab] OR “human milk”[tiab] OR “breast fed”[tiab] OR “breast feeding”[tiab] OR breastfed[tiab] OR breastfeeding[tiab] OR mothermilk[tiab] OR “mother milk*”[tiab]).
This search string was chosen because it includes all synonyms found for infants of gestational ages 32–36 weeks and breastfeeding. The medical subject heading (MeSH) “Infant, premature” was not included because this would generate results showing all articles about preterm infants combined with breastfeeding, including all those about severely and extremely preterm infants.
This systematic review was written according to the PRISMA statement. 21
Eligibility criteria
For full-text screening, the following inclusion criteria were used: (1) Investigations on quantitative effects of factors or interventions on breastfeeding outcomes in preterm infants between 32 + 0 and 36 + 6 weeks of gestation. (2) Absolute effects of factors/interventions or a comparison with full-term (≥37 weeks) infants were reported. (3) Interventions applied to the parents and/or infants. (4) Study population of at least 15 MLPIs. (5) Dutch or English language. (6) Full text paper available.
The exclusion criteria were the following: (1) Articles that also included infants with gestational age <32 weeks or >37 weeks with no subgroup analysis. (2) Studies conducted in “low resource settings” (or alike) because there may be multiple different resource and contextual factors that impact on breastfeeding in those settings. 22 (3) Animal studies. (4) Articles exclusively focusing on multiple pregnancies (twins, etc.). (5) Case studies and systematic reviews.
Study selection and data collection
The search stated previously was used to find articles for both aims of this investigation: the barriers to breastfeeding and interventions. Full-text screening was used to distinguish between barrier and intervention articles. Any data relating mother and infant characteristics of MLPIs to breastfeeding and data on interventions that attempted to improve breastfeeding in MLPIs were extracted.
Critical appraisal
For the critical appraisal, edited checklists from the Joanna Briggs Institute were used for each of the study designs, which are included in the Supplementary Data. Two independent investigators carried out the critical appraisal (N.C.C. and A.K.). Only the articles investigating interventions were critically appraised. Some items were taken out of the checklist because they were not relevant for the studies. For the checklist about quasi-experimental studies, point 5 was removed: were there multiple measurements of the outcome both pre and post the intervention/exposure? This criterium was deemed irrelevant because it can be assumed that the outcome (breastfeeding) was not present before the intervention/exposure.
Checkpoints 4 and 5 were eliminated from the checklist for randomized controlled trials: were participants blind to treatment assignment? And: were those delivering treatment blind to treatment assignment? These were presumed to be impossible because, owing to the nature of the investigated interventions, participants and those who delivered the treatment could not be blinded for the assignment to care for the infants.
Post hoc analysis
After selecting the articles and analyzing the results, it was decided to only discuss the barriers to breastfeeding that were identified in at least three articles to have sufficient evidence to draw conclusions about the effect of that specific factor on breastfeeding rates. The factors that were discussed in at least two articles are reported in Supplementary Table S1.
Results
Article selection
On April 24, 2020, the search was executed, and 266 articles were retrieved. Two duplicates were removed, leaving 264 articles for screening. The result is given in Figure 1. Fifteen articles were selected using the search strategy and inclusion and exclusion criteria: 11 about factors affecting breastfeeding in MLPIs, and 4 about interventions that may have an effect on these breastfeeding rates. The references of the four intervention articles were screened for any articles that the search string may have missed, and two additional intervention articles were subsequently identified and included.
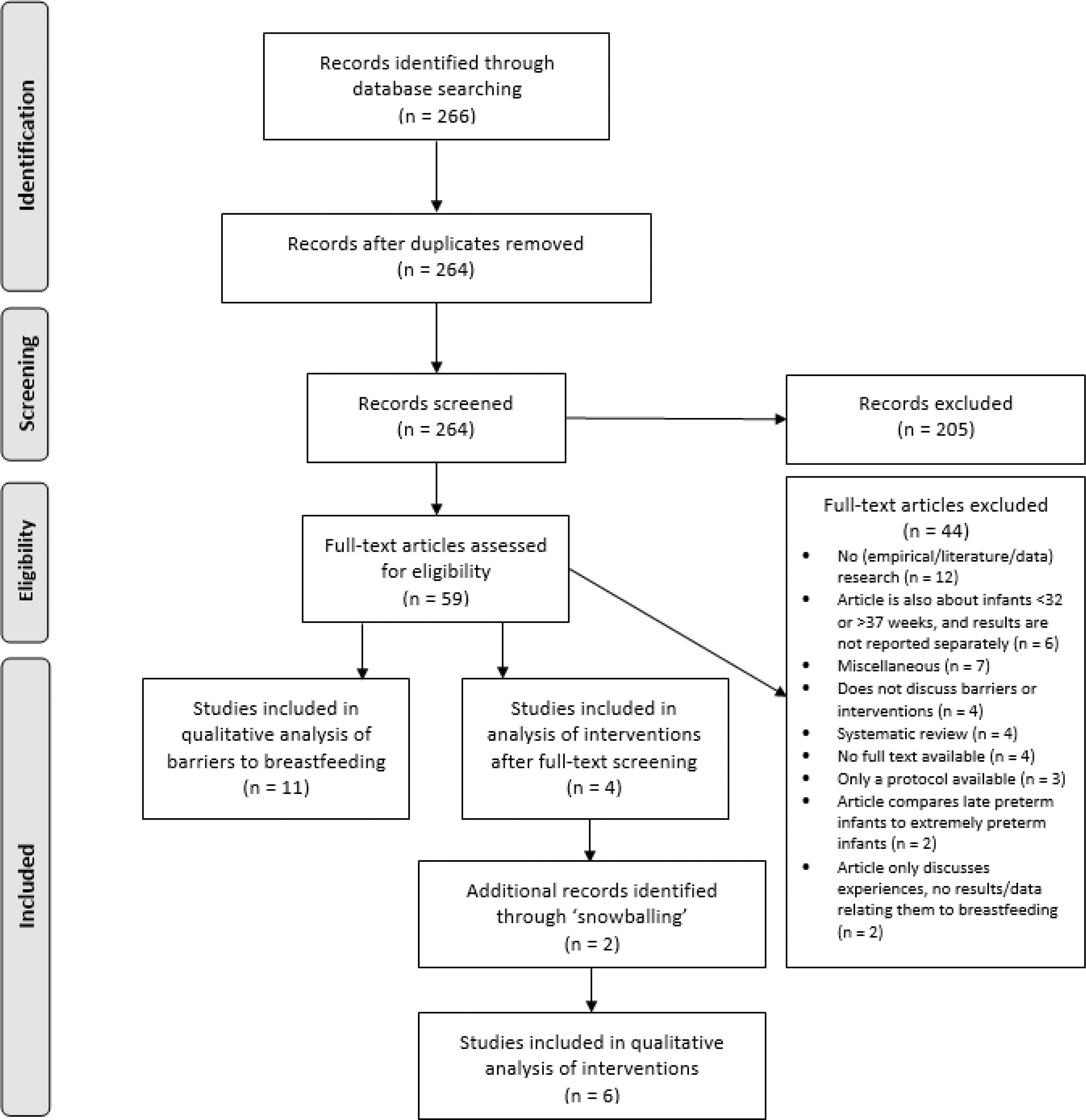
Flowchart showing article selection. Adapted from the PRISMA 2009 flow diagram. 21
Critical appraisal
The quality assessments of the articles investigating an intervention to improve breastfeeding are given in Tables 1 and 2. The full, edited checklists from the Joanna Briggs Institute 23 are provided in Supplementary Data.
Critical Appraisal of the Quasi-Experimental Studies
Critical Appraisal of the Randomized Controlled Trials
Tables 1 and 2 show that the quasi-experimental studies24,25 are generally of lower quality than the randomized controlled trials.26–29 Neither Abouelfettoh et al. 24 nor Estalella et al. 25 met the criteria of item 5: “Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analyzed?” 23 ; they gave a questionable and no explanation on loss to follow-up, respectively. More importantly, the treatment of the patients in the intervention and control groups in the study of Abouelfettoh et al. 24 differed in more ways besides the intervention (item 3 on the checklist). Another important item is item 2, which is about whether the patients in both groups were similar. No quasi-experimental study completely fulfilled this criterium, which may have affected their results. Finally, the outcomes were not always measured in a reliable way (item 7) and the statistical analysis was not explained sufficiently (item 8).
Furthermore, for the randomized controlled trials, the study by Morelius et al. 27 was the only one that did not give a sufficient description of the statistical tests used. Another important item that was not completely satisfied is item 4 (“Were outcome assessors blind to treatment assignment?” 23 ) and, similarly, item 9 (“Were outcomes measured in a reliable way?” 23 ). In the randomized controlled trials,26–29 it was unclear whether the outcome assessors were blind to treatment assignment. That said, the outcomes measured were mostly objective outcomes that would not be impacted (much) by the personal ideas and beliefs of the outcome assessor. In addition, the intervention and control groups in the study of Hake-Brooks et al. 26 were not treated the same except for the intervention (point 5): the authors note that the intervention group did not only practice kangaroo care (KC; the intervention), but they also received more attention and instructions on how to recognize feeding cues and assistance with breastfeeding. Finally, none of the randomized controlled trials27–29 had a complete follow-up or an adequate explanation for the loss to follow-up (item 6).
Barriers to breastfeeding
Table 3 summarizes the relevant characteristics of the studies selected that describe the barriers to breastfeeding. They are all cohort-30–37 or cross-sectional38,39 studies, and they were conducted in the United States30,32,33,35 or Europe.31,34, 36–40 Most studies investigated infants of gestational ages 34–36 weeks (LPIs),30–36,38,40 but some included only infants of 32–34 weeks (MPIs).37,39 The outcomes described differed per study; for example, some studies investigated whether the infants received any breast milk, and others whether they breastfed at 3 months postpartum.
General Features of the Studies Describing Barriers to Breastfeeding
EBF, exclusive breastfeeding; GA, gestational age; KC, kangaroo care; MU, maternity unit; NICU, neonatal intensive care unit; PRAMS, pregnancy risk assessment monitoring system.
The following factors were found to have an unambiguous effect on breastfeeding rates (Table 4). Higher education has a positive effect on breastfeeding. Similarly, being in a relationship was very clearly correlated with more breastfeeding. Supplementary Table S2 shows the effect of all factors that were investigated in three or more studies on breastfeeding.
Factors That Have an Unambiguous Effect on Breastfeeding Rates
++: clear positive effect; +++: clear very positive effect.
The effect of several factors on breastfeeding rates
Maternal demographics
Maternal race/ethnicity
The three studies30,32,39 investigating this factor found conflicting results. Two studies conducted in the United States30,32 showed that black women breastfeed less than women of other ethnicities, but another study, 39 which was conducted in Europe, found that women with “other” ethnicity and black women breastfeed most. However, Chiang et al. 30 and Rayfield et al. 39 provided no level of significance, whereas the results of Demirci et al. 32 were statistically significant.
Maternal age group
The six studies30,31,34,35,37,39 showed different results on the effect of maternal age on breastfeeding rates: two studies31,34 found that younger women breastfeed most, another that women of ages 25–34 breastfeed most, 37 and three studies report that mothers breastfeed more when they are older.30,35,39 Crippa et al. 31 and Kair et al. 35 provided adjusted odds ratios (ORs), but the differences were not significant.
Socioeconomic status and education
Most studies30–32,35,37,39 found that parents or mothers with higher education and/or socioeconomic status breastfeed (significantly) more than those with lower education and/or socioeconomic status. Moreover, two studies reported that women who participated in Women, Infants and Children program (WIC) and/or used Medicaid insurance to pay for their hospital stay, which generally corresponds with lower socioeconomic status, breastfed less than those who did not.30,32 However, another study 35 found that having Medicaid insurance did not affect breastfeeding rates after adjustment for maternal age, maternal education, marital status, neonatal intensive care unit (NICU) admission, infant birth weight, maternal body mass index, and state residency. Jónsdóttir et al. 34 found no significant relationship between income or education and breastfeeding rates either. However, the general pattern across these studies is that usually women with higher socioeconomic status breastfeed more than those with low socioeconomic status.
Relationship status parents
All six studies30,32,34,35,37,39 investigating relationship status found that being married, having a partner, or living together increases breastfeeding rates noticeably or significantly. For example, Jónsdóttir et al. 34 found an OR of 6.63 (95% confidence interval [CI]: 2.51–17.48) for not breastfeeding exclusively when the mother has no partner.
Parity and history of prematurity
One study 35 found no significant difference between breastfeeding rates of multiparous and primiparous women, 35 but two studies32,37 reported that primiparous women breastfeed significantly more than multiparous women. Demirci et al. 32 showed that the OR for not breastfeeding as a multiparous woman is 1.59 (95% CI = 1.44–1.76), and also that mothers who had a previous preterm birth breastfed significantly less than those who did not (OR = 1.33, 95% CI = 1.13–1.55).
Infant characteristics
Gestational age and birth weight
In three studies, gestational age (32, 33, 34, 35, or 36 weeks)32,34,39 did not affect breastfeeding rates. One study 35 investigated the effect of birth weight (<1,500, 1,500–2,499, >2,500 g) on breastfeeding, and they reported that infants of 1,500–2,499 g were breastfed significantly less than those with weights of <1,500 or >2,500 g. 35 For gestational age, only Mitha et al. 37 found a significant difference: infants born at 33 weeks were breastfed significantly more than those born at 32 or 34 weeks gestational age. 37
Multiples and singletons
One study 31 about exclusive breastfeeding showed a significant difference between twins and singletons (exclusive breastfeeding of twins: OR = 0.2, 95% CI = 0.1–0.5). The two other studies32,37 looking at breastfeeding initiation and breastfeeding at discharge found no significant difference between breastfeeding rates of singletons and multiples.
NICU admission
In four studies, NICU admission did not affect breastfeeding rates.30,32,34,35 However, Rayfield et al. 39 found that any breastfeeding after 6 weeks was higher in mothers whose infant was not admitted to the NICU breastfed, compared with mothers whose infant was admitted to the NICU (81.7% versus 67.8%, respectively).
Delivery, postpartum and breastfeeding characteristics
Type of delivery
Three studies31,34,35 found no significant or large difference in breastfeeding rates after different types of deliveries, especially after calculating an adjusted OR.31,35 However, Demirci et al. 32 found that significantly more mothers initiated breastfeeding when a certified (nurse) midwife was present at the delivery and also if the women did not have any labor anesthesia, and Mitha et al. 37 found that significantly fewer women breastfed at discharge after having a cesarean section.
Bonding (KC, skin-to-skin contact, and rooming-in)
Mitha et al. 37 found that KC improves breastfeeding and Gianni et al. 38 reported that encouraging mothers to practice KC also increases breastfeeding rates. Goyal et al. 33 concluded that rooming in improves breastfeeding, but also that LPIs are less likely to be roomed-in with their mother. Crippa et al. 31 found no significant difference in breastfeeding rates after skin-to-skin contact or rooming-in. Gerhardsson et al. 40 reported that 96% of the LPIs who bed-shared with their parents received any breast milk, compared with 84% of the infants who did not bed-share (p = 0.046).
Breastfeeding factors
Breastfeeding characteristics that significantly affect breastfeeding rates are: a feeling of reduced milk supply, 31 breastfeeding self-efficacy, 40 expressing breast milk (decreases chances of exclusive breastfeeding), 38 using a nipple shield, 34 time to first breastfeeding (shorter is more likely to breastfeed exclusively), and breastfeeding frequency on day 1 and 2 (more frequently is more likely to breastfeed exclusively). 36 Not having experienced enough help and support in the hospital significantly decreased breastfeeding rates at 10 days (OR = 0.61 [0.50–0.74]) and at 6 weeks (OR = 0.75 [0.62–0.90]). 39 Gerhardsson et al. 40 found that 79% of the LPIs who did not use a pacifier breastfed exclusively at 3 months corrected age, compared with 65% of those who did use a pacifier (p = 0.016).
Finally, Rayfield et al. 39 reported that multiparous mothers who previously breastfed for longer than 6 weeks had higher breastfeeding rates at 10 days and 6 weeks than primiparous mothers, and even higher breastfeeding rates than those who breastfed for shorter than 6 weeks, and Crippa et al. 31 also found that previous positive experience with breastfeeding significantly improved breastfeeding rates (adjusted OR of 3.0 [1.0–8.5]). 31
Interventions to improve breastfeeding
All six intervention studies24–29 are randomized controlled trials26–29 or quasi-experimental studies24,25 (Table 5). They were conducted in North America 26 and South America, 28 Africa, 24 and Europe.25,27,29 The setting of two studies was a maternity service, 25 the other studies were set in NICUs24,27–29 and one study took place in a maternity service and NICU. 26
General Features of the Intervention Studies
C, control; GA, gestational age; I, intervention; KC, kangaroo care; MDT, multidisciplinary team; NICU, neonatal intensive care unit; RCT, randomized controlled trial; T, total.
Three studies investigated cup feeding as an intervention compared with bottle feeding,24,28,29 one study was about providing parents with more information and health care support, 25 another about having continuous skin-to-skin contact between parents and infants instead of standard skin-to-skin contact, 27 and one about providing KC compared with no KC. 26 The outcomes for studies investigating interventions to improve breastfeeding were grouped into endpoint categories. The definition of “(exclusive) breastfeeding” was different for some studies; breastfeeding can mean either feeding of the infant directly at the breast or feeding breast milk through any method. These definitions are provided in Tables 6–8.
Effect of Interventions on the Initiation of Breastfeeding (at Discharge)
Breastfeeding was not defined in this study—it is unclear whether this is feeding of breast milk in any way, or directly at the breast.
Total numbers of patients in results and design do not match because of loss to follow-up.
C, control; GA, gestational age; I, intervention; KC, kangaroo care; MDT, multidisciplinary team; n.s., not significant; RCT, randomized controlled trial; T, total.
The Effect of Interventions on the Continuation of Breastfeeding (5 Days Postdischarge up to 6 Weeks)
C, control; GA, gestational age; I, intervention; KC, kangaroo care; n.s., not significant; RCT, randomized controlled trial; SD, standard deviation; T, total.
The Effect of Interventions on the Continuation of Breastfeeding for 3 to 6 Months
C, control; GA, gestational age; I, intervention; KC, kangaroo care; n.s., not significant; RCT, randomized controlled trial; T, total.
For initiation of breastfeeding (Table 6), cup feeding was shown in one study to significantly affect the number of infants breastfeeding exclusively or partially directly at the breast, 29 but in another there was no significant change in breastfeeding exclusively or partially directly at the breast. 28 Providing parents with more information and direct health care support significantly improved the number of mothers exclusively or partially breastfeeding (feeding expressed breast milk or directly at the breast). 25 Continuous skin-to-skin contact did not significantly affect breastfeeding compared with standard skin-to-skin contact, 27 and neither did standard skin-to-skin contact compared with no skin-to-skin contact. 26
For continuation of breastfeeding for 5 days to 6 weeks (Table 7), the results are the same as for breastfeeding initiation: no significant effect of cup feeding 28 or continuous skin-to-skin contact 27 or KC 26 on breastfeeding directly at the breast, but a significant improvement of the number of feeds that consisted of breast milk when infants are cup fed instead of bottle fed. 24
At 3 months postdischarge (Table 8), cup feeding showed no significant effect on feeding exclusively or partially at the breast at 3 months in one study, 28 but it did improve exclusive breastfeeding at 3 months and breastfeeding partially or exclusively at the breast at 6 months in another study. 29 Continuous skin-to-skin contact compared with standard skin-to-skin contact showed no significant difference in breastfeeding rates at 6 months either. 27 Breastfeeding rates at 3, 6, 12, and 18 months were reported in the study of Hake-Brooks et al., 26 but there was no significant difference between breastfeeding after practicing KC compared with no KC at any time point.
Hake-Brooks et al. 26 also reported on exclusivity and duration of breastfeeding after practicing KC compared with no KC. They found that KC dyads breastfed significantly more exclusively over time (from hospital discharge to 18 months), p = 0.047. At 6 months, this difference was statistically significant (p = 0.041). Furthermore, they reported that KC dyads breastfed (exclusively or not) significantly longer than infants who did not experience KC: 5.08 ± 5.48 months compared with 2.05 ± 2.15 months, respectively (p = 0.003).
Discussion
Barriers to breastfeeding consistent across all studies are socioeconomic status and relationship status. Higher socioeconomic status and more education are consistently associated with breastfeeding success and being in a relationship is associated with higher breastfeeding rates even more than higher socioeconomic status and education.
The interventions investigated were cup feeding; providing parents with more information and health care; and skin-to-skin contact/KC. Providing parents with more information and health care improved initiation of breastfeeding and continuation for 5 days to 6 weeks, but more skin-to-skin contact/KC did not. Cup feeding had conflicting effects on initiation of breastfeeding, continuation for 5 days to 6 weeks and continuation for 3 or 6 months. More skin-to-skin contact/KC did not affect breastfeeding rates at hospital discharge, 3, 6, 12 and 18 months, but it did significantly improve duration and exclusivity of breastfeeding at 6 months in one study.
The intervention of providing parents with more information and health care may be related to the barrier of “low socioeconomic status”: when these women receive more support and education on the importance of breastfeeding, this may reduce the adverse impact of low socioeconomic status.
Possible interpretations of differences in the effect of interventions
First, the critical appraisal shows that the quasi-experimental studies (Abouelfettoh et al. 24 and Estalella et al. 25 ) were of lower quality than the randomized controlled trials (Hake-Brooks et al., 26 Morelius et al., 27 Rocha et al. 28 and Yilmaz et al. 29 ). Abouelfettoh et al., 24 Rocha et al., 28 and Yilmaz et al. 29 all examined the effect of cup feeding instead of bottle feeding on breastfeeding rates. Abouelfettoh et al. 24 and Rocha et al. 28 evaluated breastfeeding rates at 5–15 days and at 1 week, respectively. Whereas Abouelfettoh et al. 24 found a significant improvement for infants who were cup fed, Rocha et al. 28 found no significant difference. This difference in results may be related to the lower quality of the study of Abouelfettoh et al., 24 or owing to the fact that the studies were carried out in different countries (Egypt and Brazil), and infants of different age groups were included (Rocha et al. 28 also included infants of gestational ages 32–34 weeks, whereas Abouelfettoh et al. 24 only included infants of 34–37 weeks), which was also reported in Table 5. Moreover, Abouelfettoh et al. 24 included only 60 infants in their study, and Rocha et al. 28 included 78. The low number of participants may also have contributed to the difference in results.
The randomized controlled trials by Hake-Brooks et al. 26 and Morelius et al. 27 both examined the effect of skin-to-skin contact/KC on breastfeeding rates. There are several differences between these two studies. Most importantly, Hake-Brooks et al. 26 compared an average of 4.47 hours of KC per day to no KC, whereas Morelius et al. 27 compared an average of 19.7 hours of skin-to-skin contact per day with an average of 7 hours of skin-to-skin contact per day (standard care). Moreover, the intervention and control groups in the study of Hake-Brooks et al. 26 did not receive the same care other than the intervention, because the mothers in the KC group also received more assistance with breastfeeding and recognizing infant clues. Nevertheless, both studies found that more skin-to-skin contact/KC did not significantly affect breastfeeding rates at any time point. Hake-Brooks et al. 26 reported that KC did significantly improve duration and exclusivity of breastfeeding, which was not investigated by Morelius et al. 27
Furthermore, quasi-experimental studies (lower quality) generally found a significant improvement after implementation of their intervention (2 of 2 results—100%) than randomized controlled trials (higher quality) (5 of 12 results—41.6%), which may reflect differences in methodological quality. This suggests that more high-quality research is necessary to find the true relationship between these interventions and breastfeeding rates.
Finally, the randomized controlled trials of Rocha et al. 28 and Yilmaz et al. 29 reported conflicting results on the effect of cup feeding on partial and exclusive breastfeeding rates at discharge and at 3 months postdischarge. Yilmaz et al. 29 found a significant improvement when cup feeding instead of bottle feeding, whereas Rocha et al. 28 reported no significant effects. This may be owing to the fact that the studies were conducted in two different countries (Brazil 28 and Turkey 29 ) and in different years (1998–200028 and 2006–200829). Most importantly, Rocha et al. 28 only included infants weighing <1,700 g, who were fed using an orogastric tube until they weighed 1,600 g. This might indicate that cup feeding is less effective in more premature and/or lighter infants, or that the intervention is more effective if applied earlier in life.
Additional results found in published articles
Maternal factors that negatively affect breastfeeding in MLPIs
First, at 3–8 days postpartum, copious milk production begins (lactogenesis II), which is preceded by lactogenesis I, which started during pregnancy. Because mothers of MLPIs have often already been discharged from the hospital when milk production starts, it may be more difficult to get support from lactation specialists, for example, to start breastfeeding or expressing milk. This may increase the chances of poor attachment (latch) and/or incomplete emptying of the breast, which may negatively impact lactogenesis and reduces the likelihood of prolonged breastfeeding. 12
Second, mothers of MLPIs experience more stress than those of full-term infants, both physically and emotionally. Concerns about their own and their infant's health may negatively affect lactation 41 owing to the inhibitory effect of stress on oxytocin and prolactin production. The additional stress of a limited milk supply may further decrease lactation. 42 Studies suggested that this stress may be aggravated because mothers of preterm infants may feel like they have to compensate for the preterm birth by breastfeeding to help reduce the risk of complications, while noticing that they are not producing enough milk. 43 Mothers of MLPIs also have a higher risk of depression and anxiety, 44 which may adversely affect continued breastfeeding.42,45 Hallowell et al. 12 described several other maternal factors that affect breastfeeding rates in LPIs: intent to breastfeed, previous lactation experience, higher gestational age, more milk output, early frequent breastfeeding, more breastfeeding support, and extracting breast milk using a high-quality breast pump all improve breastfeeding.
Infant factors that negatively affect breastfeeding in MLPIs
First of all, MLPIs often have difficulties breastfeeding because the skills necessary to breathe and drink simultaneously develop in the last weeks of pregnancy: they have to create an intra-oral vacuum to stimulate the breast, with subsequent stimulation of maternal oxytocin production and breast milk production. 12 Without proper feeding technique, infants may tire more quickly and may not be able to drink enough to support their growth. 42 When exhaustion causes them to stop drinking, this may be interpreted as a sign of satiety, which increases the risk of impaired enteral intake and growth.12,17
Not consuming enough breast milk may also increase the risk of jaundice, leading to readmission and separation of mother and infant and therefore less contact between the two, which will negatively impact oxytocin production and milk production owing to the physical contact between the mother and infant. 12
Furthermore, MLPIs often need medical interventions soon after birth, which also reduces the physical contact between mother and infant despite it being necessary to start milk production. 17 Similarly, MLPIs are more likely to be born through Cesarean section,46,47 which may also decrease the initiation of lactation. 47
Other interventions that can be implemented
First of all, there are some conflicting results on the use of nipple shields to improve breastfeeding: Spatz et al. 48 and Hallowell et al. 12 found that nipple shields increase breastfeeding rates, but (systematic) reviews of Cartwright et al. 18 and Lapillonne et al. 49 report that some studies found that nipple shields decrease breastfeeding.
Second, Briere et al., 17 Cartwright et al., 18 and Lapillonne et al. 49 reported that rooming-in and possibly increased skin-to-skin-contact improve breastfeeding. Other interventions that improve breastfeeding rates according to several studies are (frequently) using a breast pump,12,17,50 following up on breastfeeding progress after discharge,12,17,50 educating mothers on (the importance of) breastfeeding,17,18,49 having a (daily) weight goal for the infant, 12 helping parents to recognize feeding cues from their infants,17,18 and additional support by a nurse or lactation specialist to help with breastfeeding.12,17
Furthermore, as mentioned before, studies found that mothers of MLPIs are more stressed, more often depressed and experience more anxiety than mothers of full-term infants.41,44 It is important to reduce this stress, because the mother's mental state is crucial for breast milk production. 42 According to Chertok et al., 51 interventions that may significantly reduce stress in parents of preterm infants are educating parents on premature newborn infants in person, or by providing books or video; using the Mother-Infant Transaction Program (pre- and postdischarge intervention sessions for parents); being taught how to observe the infant and be more engaged in their care; receiving the Creating Opportunities for Parent Empowerment model, which also educates parents about their preterm infant; and parent-to-parent peer support.
Limitations
Most studies used limited statistical analysis to evaluate the results. Only a few performed statistical analysis for significance, and most did not adjust for possible confounders. Studies that did adjust for confounders often demonstrated that apparently significant results became nonsignificant. This may reflect inadequate sample size and/or study design. In addition, “socioeconomic status” was difficult to robustly define. Several articles used different measures of socioeconomic status (educational level, income, WIC-participation, type of insurance, etc.), and in these cases the relationship with breastfeeding success was not always consistent. The effects of the different factors are described in Supplementary Table S2. It is challenging to compare socioeconomic status across countries, as different measures are used, and this may limit generalizability of our findings. In addition, most studies were conducted in Europe and the United States, which may lack generalizability to countries with different health care organizations and resources. The results of many studies exploring barriers to breastfeeding may have been affected by residual confounding that may be especially important in observational studies. It is also possible that some relevant studies were not found with the search string that was used: articles may not have included in the title or abstract that they also collected data for MPIs or LPIs. To minimize the probability of overlooking an important interventional study, the reference lists of all interventional studies were screened, and two more articles26,28 were identified this way.
In addition, the limited number of relevant articles meant that no selection based on specific outcome measures could be performed, so it was not possible to generate a general conclusion about exclusive breastfeeding at 6 months postpartum only. Another problem with the limited number of included articles is the heterogeneity of the studies for specific characteristics: for example, singletons or multiples or specific medical conditions. Because of this, only general conclusions about trends can be drawn.
Finally, some articles specifically stated in their inclusion and exclusion criteria that women had to intend to breastfeed to participate in the study (Abouelfettoh et al., 24 Yilmaz et al. 29 ), or noted that (almost) every woman intended to breastfeed (Morelius et al. 27 ); others reported that women had to have initiated breastfeeding to be included in the follow-up (Estalella et al. 25 ) and some studies reported nothing concerning this topic (Rocha et al. 28 ). Although this may not affect the level of effectiveness of the intervention, it may impact on generalizability. However, this difference should be taken into account when comparing general breastfeeding percentages across the studies, because studies that only investigated women who actually started breastfeeding will show higher breastfeeding rates than studies that included all women.
Strengths
Our comprehensive review presents data on both initiation of breastfeeding or continuation of breastfeeding, and the tables include detailed data presented according to maternal or infant factors.
We also provide detailed data on the quality of the studies, which provides context and facilitates better interpretation of the results. Furthermore, we specifically focused on MLPIs, whereas many previous studies focus on either <32 or >34 weeks gestational age.
Implications for research
Further high-quality studies investigating the effect of interventions on breastfeeding rates in MLPIs are necessary to improve the evidence base for practice, and specifically should aim to resolve uncertainties around the impacts of cup feeding and use of nipple shields.
Implications for practice
In conclusion, our study emphasizes the need to pay specific attention to women in risk groups, including low socioeconomic status/education and not having a partner. Further data on cup feeding and providing parents with more understandable information and greater support have the potential to greatly improve breastfeeding rates. It is important for health care workers and policy makers to be aware of these risk groups and design interventions to improve breastfeeding success.
Conclusion
The groups that are at risk for low breastfeeding rates are mothers with low socioeconomic status and/or low education and single mothers. For initiation of breastfeeding (until discharge from the hospital), providing parents with more information on breastfeeding and more health care support significantly improved breastfeeding. Continuous skin-to-skin-contact compared with standard skin-to-skin contact did not significantly improve initiation of breastfeeding, continuation for 5 days to 6 weeks, or continuation for 3 months or longer. KC compared with no KC did not significantly affect breastfeeding rates at hospital discharge, 3, 6, 12, or 18 months, but it did significantly improve breastfeeding duration and exclusivity of breastfeeding at 6 months. Cup feeding was shown to significantly increase breastfeeding initiation in one study, but another reported no significant effect. For the continuation of breastfeeding for 5 days to 6 weeks, there were again different results on the effect of cup feeding: one study found a significant improvement, another did not. Finally, for continuation for 3–6 months, cup feeding improved breastfeeding significantly in one study, but in another there was no significant difference.