
Abstract
Background:
Human milk from coronavirus disease 2019 (COVID-19)-recovered women may be useful as oral antibody therapy to prevent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and provide long-term immunity to neonates and young children. As convalescent plasma is already used as antibody therapy, this study aimed to compare the binding capacity of antibodies specific to the receptor-binding domain (RBD) of SARS-CoV-2 between human milk and serum from COVID-19-recovered women.
Materials and Methods:
The areas under the curve (AUCs) for IgA, IgM, and IgG specific to the SARS-CoV-2 RBD in human milk and serum samples were measured using enzyme-linked immunosorbent assay. Milk samples were collected from 12 COVID-19-recovered women, while serum samples were from 10 COVID-19-recovered women. The antibody concentrations were also determined.
Results:
Our study reveals that SARS-CoV-2 RBD-specific antibody titers differed between human milk and serum samples from COVID-19-recovered women. When the AUCs were not divided by the antibody concentration, SARS-CoV-2 RBD-specific IgA, IgM, and IgG levels were higher in the serum sample group than the human milk group (p < 0.001). However, the titers of SARS-CoV-2 RBD-specific IgM (AUC/μg of IgM) and IgG (AUC/μg of IgG) were higher in human milk samples than serum samples (p < 0.05). The titer of SARS-CoV-2 RBD-specific IgA (AUC/mg of IgA) was higher in the serum sample group than the human milk group (p < 0.01).
Conclusions:
Human milk antibodies specific to the RBD of SARS-CoV-2 must be purified to obtain comparable binding capacity observed with SARS-CoV-2 RBD-specific serum antibodies.
Introduction
Convalescent plasma therapy can provide a prophylaxis treatment to prevent and treat infectious diseases. Plasma from patients who have recovered from coronavirus disease 2019 (COVID-19) provides short-term immunity to the subject at risk of infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and improves the clinical outcomes in severe COVID-19 cases. 1 Our recent findings demonstrated that levels of IgG reactive to SARS-CoV-2 S1 and S2 subunits and the nucleocapsid protein were higher in mothers during the COVID-19 pandemic than in unexposed mothers in 2018. 2 We also demonstrated that S2 SARS-CoV-2 IgG levels in human milk were higher in mothers with a confirmed COVID-19 polymerase chain reaction (PCR) test or in mothers with previous viral symptoms than in prepandemic mothers (2018). 3 Fox et al. 4 also observed that SARS-CoV-2 receptor-binding domain (RBD) antibody levels (secretory IgA [IgA] and IgG) were higher in COVID-19-recovered women than in unexposed women. Therefore, human milk antibodies from COVID-19-recovered women could be used as oral antibody therapy to prevent and treat SARS-CoV-2 infection and provide long-term immunity to vulnerable infants.
The antibody composition of serum samples differs from human milk samples. Serum samples contain ∼80% of IgG, ∼12% IgA, ∼8% of IgM, and 0% of SIgA or SIgM, 5 whereas human milk samples have ∼80–90% of SIgA, ∼10% of IgA, ∼18% SIgM/IgM, and 4% of IgG.6–10 Our recent study revealed that human milk SIgA was the most abundant antibody reactive to SARS-CoV-2 S1 and S2 subunits (∼79% SIgA versus ∼9% IgG versus ∼12% SIgM/IgM). 2 The survival of human milk SIgA is higher than IgG, IgM, and IgA during digestion in preterm infants as the secretory component (SC) protects IgA against the proteolytic digestive enzymes.8,11–13 The SC is also a critical constituent of SIgA and SIgM to perform immune exclusion and prevent pathogen attachment to epithelial cells.7,14,15 Therefore, SIgA is likely the most effective antibody to be used as oral therapy due to its higher neutralizing capacity and abundance in human milk.12,13 However, SIgM may also play a relevant role in neutralizing SARS-CoV-2 as it is an elusive player in mucosal immunity. 16 No study has compared the binding capacity of antibodies specific to SARS-CoV-2 between human milk and serum samples.
The RBD of the spike protein (on the surface of the S1 subunit) allows the attachment of SARS-CoV-2 to the angiotensin-converting enzyme 2 (ACE) receptor of human epithelial cells. The RBD is specific to SARS-CoV-2 and less conserved than other human coronaviruses, reducing the presence of cross-reactive antibodies. The binding capacity of serum antibodies specific to the RBD of SARS-CoV-2 was strongly correlated with their neutralizing capacity against SARS-CoV-2 in COVID-19-recovered patients.17–19 This RBD antibody assay was correlated with the protective immune response against SARS-CoV-2, suggesting that this enzyme-linked immunosorbent assay (ELISA) can be used as a surrogate for neutralizing potency in SARS-CoV-2. 17
Most studies on SARS-CoV-2 RBD-specific antibodies involve samples obtained from symptomatic patients with severe illness and hospitalization.20–22 However, investigation of mild infection by SARS-CoV-2, especially breastfeeding mothers, is essential to understand their antibodies secreted in human milk. Worldwide, fever is the most frequent symptom (69.4%), followed by cough (35%), in mothers diagnosed with COVID-19 by reverse transcription–polymerase chain reaction (RT-PCR), whereas 13.4% of mothers with SARS-CoV-2 infection were asymptomatic. 23 Headache (54.9%), cough (51.3%), fever (39.3%), muscle aches (45.2%), sore throat (34.6%), and chills (29.2%) were the most reported symptoms in mothers with laboratory-confirmed SARS-CoV-2 infection in the United States. 24 This study aimed to compare the titers of SARS-CoV-2 RBD-specific antibodies between human milk and serum from COVID-19-recovered women. These results can underline the potential of human milk antibodies to treat and protect against SARS-CoV-2 infection in vulnerable infants.
Materials and Methods
Study design and participants for milk collection
A screening survey was completed by 200 donors at Mother's Milk Cooperative (Boulder City, NV) to identify donors who had the SARS-CoV-2 infection confirmed by RT-PCR. The survey also identified donors with viral symptoms associated with COVID-19, but did not get a PCR test due to lack of accessibility. Participants reported when they were sick (including duration and frequency) and their symptoms. Human milk samples for a control group were collected from mothers in 2018 before the COVID-19 pandemic. The inclusion criteria were donors with confirmed COVID-19 PCR test or donors with previous viral symptoms related to SARS-CoV-2 infection, living in the United States, with lactation time between 4 and 10 months, passing blood tests, and completing a health questionnaire. Lactation time between 4 and 10 months was selected to reduce the effect of lactation time on the levels of antibodies. Our previous studies3,6,7 demonstrated that antibody concentrations were stable between 4 and 10 months of lactation. Written consents to use their milk for research were obtained from all participants. Donors were approved through Mother's Milk Cooperative. Milk collection was approved by the institutional review board (IRB00012424) of Medolac Laboratories. The exclusion criteria were mothers who had no viral symptoms related to COVID-19 and no COVID-19 PCR test and donors who had medical conditions and were smoking, taking medications, or on drugs.
Serum collection
Serum samples (1 mL for each donor) from ten women were purchased from Sanguine BioSciences, Inc. (San Francisco, CA), a multisite tissue repository providing annotated biospecimens for approved investigator-directed biomedical research initiatives (Pro00035204). The IRB (CR00198527) was approved by ADVARRA (Columbia, MD). Serum samples were frozen and transported in a box with dry ice to Medolac Laboratories, where they were kept frozen and stored at −80°C until the ELISA measurements.
Human milk collection
Human milk samples (150–250 mL) were collected at home with clean electric breast pumps into sterile plastic containers and stored immediately at −20°C in deep freezers. The breast was cleaned with a wet washcloth (no soap or alcohol) before pumping. Human milk samples were frozen and transported in insulated boxes to Medolac Laboratories, where they were kept frozen and stored at −80°C until the ELISA measurements. Frozen samples were rapidly thawed at 37°C and centrifuged at 1,301 g for 20 minutes at 4°C. The supernatant was collected, separated into aliquots, and stored at −80°C until analyzed.
SARS-CoV-2 RBD-specific antibody titers
The areas under the curve (AUCs) of SIgA/IgA, SIgM/IgM, and IgG specific to the RBD of SARS-CoV-2 were determined using ELISAs, as described in our recent study with some modifications. 2 Briefly, ELISAs were recorded with a microplate reader (SpectraMax iD5; Molecular Devices, Sunnyvale, CA). Clear flat-bottom microplates were coated with 100 μL of recombinant SARS-CoV-2 RBD (Sino Biological US, Inc., Wayne, PA) at 1 μg/mL in 1 × phosphate-buffered saline (PBS). Microplates were incubated overnight at 4°C. After incubation, plates were washed three times using PBS 1 × with 0.05% Tween 20 (PBST), and 200 μL of blocking buffer (PBST with 3% of bovine serum albumin fraction V) was added in all wells for 1 hour at room temperature. Samples (serum or human milk supernatants) were diluted from 5 × to 640 × for IgA and IgM (for both milk and serum) and milk IgG and from 5 × to 5,120 × for serum IgG in serial twofold dilutions in blocking buffer. For each step (addition of 100 μL standards/samples and secondary antibodies at 1 μg/mL), washing and incubation for 1 hour at room temperature were performed. Detection was completed using goat anti-human IgM mu-chain HRP for total IgM, goat anti-human gamma-chain HRP for IgG, and goat anti-human alpha-chain HRP for total IgA (Abcam, Cambridge, MA). Interpolation of a standard curve (sigmoidal, 4PL) was created using 8–10 points (in duplicate) for each sample, and the AUC was calculated using GraphPad Prism (version 8).
Concentration of antibodies
The concentrations of IgA, IgM, and IgG were determined using the ELISA described in our recent publication. 6
Statistical analysis
The Mann–Whitney test was applied using GraphPad Prism (version 8) to compare AUCs of RBD-specific antibodies between human milk and serum samples. The sample size of mothers was determined based on antibody levels detected in our previous study.9,10 The AUC of the SARS-CoV-2 RBD antibody was divided by the respective antibody concentration for each sample (serum and human milk). The effect of infant gender on the antibody levels in human milk samples was determined using unpaired t tests. The effect of the type of symptom on the antibody levels in human milk and serum samples was evaluated using unpaired t tests. Linear regressions were evaluated between maternal age and antibody levels and between the elapsed time from infection to sample collection and antibody levels for human milk and serum samples.
Results
Maternal demographics
The survey allowed screening of COVID-19-recovered women for the milk collection. Among 200 women in the cohort, eight mothers had a confirmed COVID-19 PCR test and eight mothers had no PCR test, but had viral symptoms associated with COVID-19. Among those 16 COVID-19-recovered women, four of them were excluded due to their low titers of SARS-CoV-2 RBD-specific antibodies (Fig. 1). These four women had no COVID-19 PCR test and reported to have nasal congestion or cough, thus they were not likely to have been previously infected by SARS-CoV-2. The demographic details of COVID-19-recovered women who donated human milk samples and those who donated serum samples are presented in Table 1 (see Supplementary Tables S1 and S2 for the description of individual women, including the presence of a confirmed COVID-19 PCR test, symptoms, and their age). The control group collected human milk samples from six mothers in 2018 before the COVID-19 pandemic (see Supplementary Table S3 for the description of individual women). Age was comparable between the COVID-19 human milk group, COVID-19 serum group, and human milk control group.
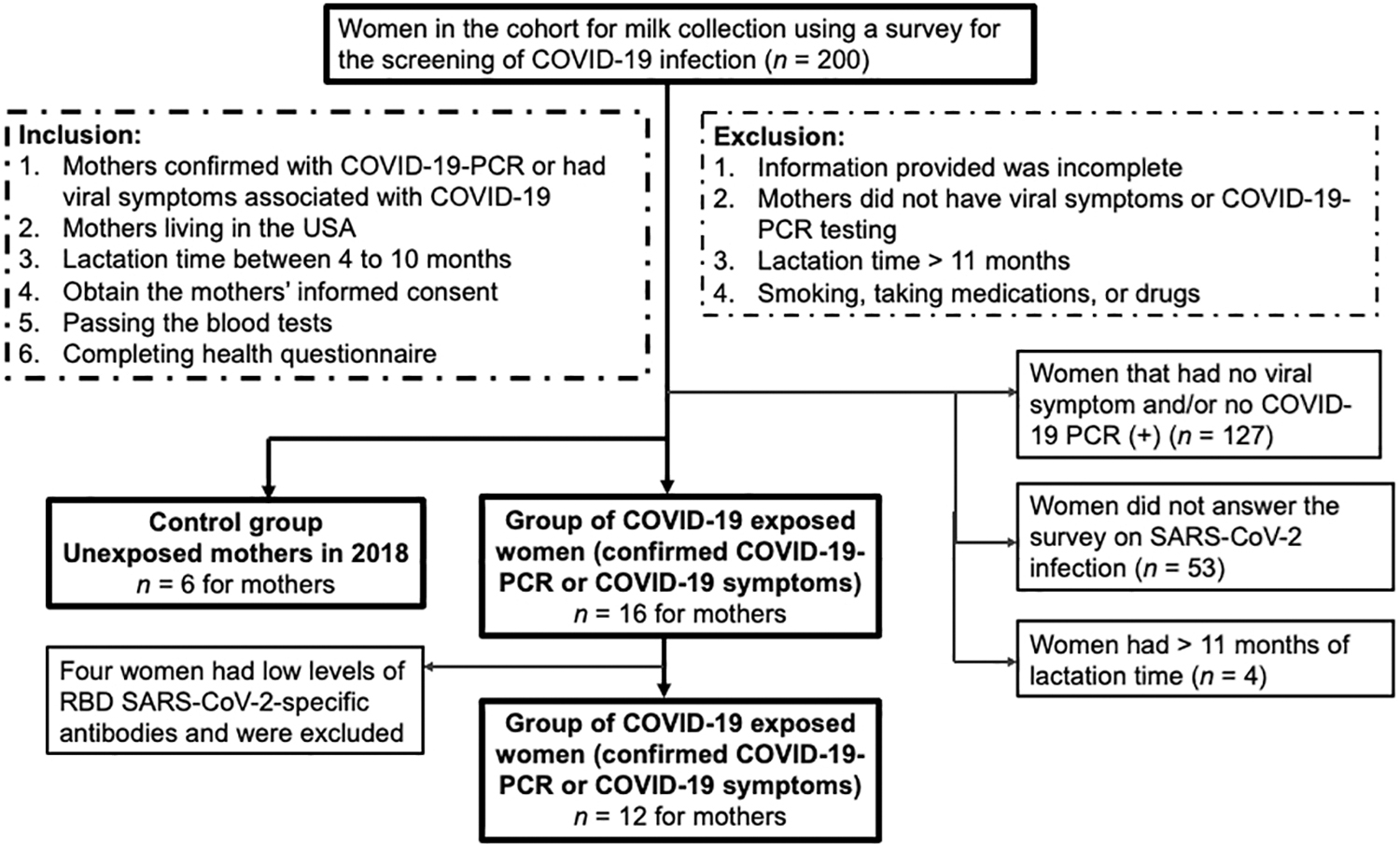
Flow chart and screening for selection of COVID-19-recovered women who donated human milk in the study. COVID-19, coronavirus disease 2019.
Demographic Description of Coronavirus Disease 2019-Recovered Women for the Milk Collection and Serum Sample Collection
Women did not have autoimmune and infectious diseases and gynecologic, hematologic, gastrointestinal, cardiovascular, respiratory, or rheumatologic issues.
Data are mean ± SD (minimum to maximum).
Frequent COVID-19 symptoms are fever, cough, and fatigue, and less frequent symptoms are loss of taste/smell, nasal congestion, chills, body aches, headache, and runny nose (see Supplementary Tables S1 and S2 for the characteristics of individual mothers).
COVID-19, coronavirus disease 2019; PCR, polymerase chain reaction; SD, standard deviation.
Concentration of antibodies
IgA concentration was comparable between human milk and serum samples (p = 0.20) (Fig. 2A). IgM and IgG concentrations were 54-fold and 617-fold higher in serum samples than human milk samples, respectively (p < 0.001) (Fig. 2B, C).
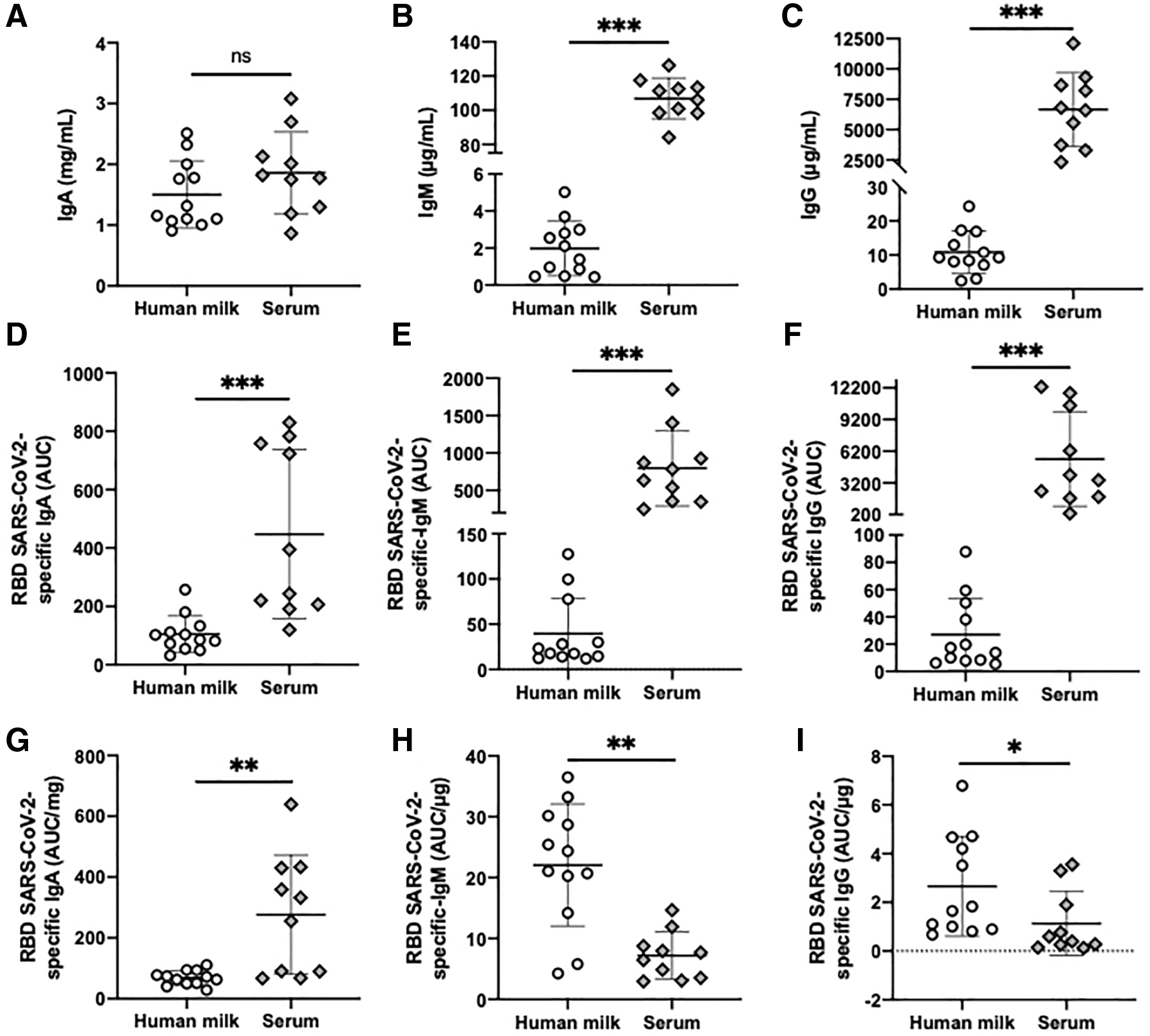
Comparison of titers (AUC) of antibodies specific to the RBD of SARS-CoV-2 between human milk and serum from COVID-19-recovered mothers.
SARS-CoV-2 RBD-specific antibodies
Human milk and serum from COVID-19-recovered women
For the antibody titers, AUCs of SARS-CoV-2 RBD-specific IgA, IgM, and IgG (without dividing by the antibody concentration of the sample) were 4.2-, 20-, and 202-fold higher in serum samples than in human milk samples (p < 0.001) (Fig. 2D
For the titer/antibody concentration, levels of SARS-CoV-2 RBD-specific IgA (AUC/mg of IgA) were fourfold higher in serum than in human milk (p = 0.004) (Fig. 2G). The levels of SARS-CoV-2 RBD-specific IgM (AUC/μg of IgM) were 3.1-fold higher in human milk than in serum (p = 0.002) (Fig. 2H). The levels of SARS-CoV-2 RBD-specific IgG (AUC/μg of IgG) were 2.3-fold higher in the human milk group than in the serum group (p = 0.014) (Fig. 2I). The calculation of AUC/antibody concentration provides the antibody level specific to the SARS-CoV-2 RBD among the total antibodies of the same isotype in each sample.
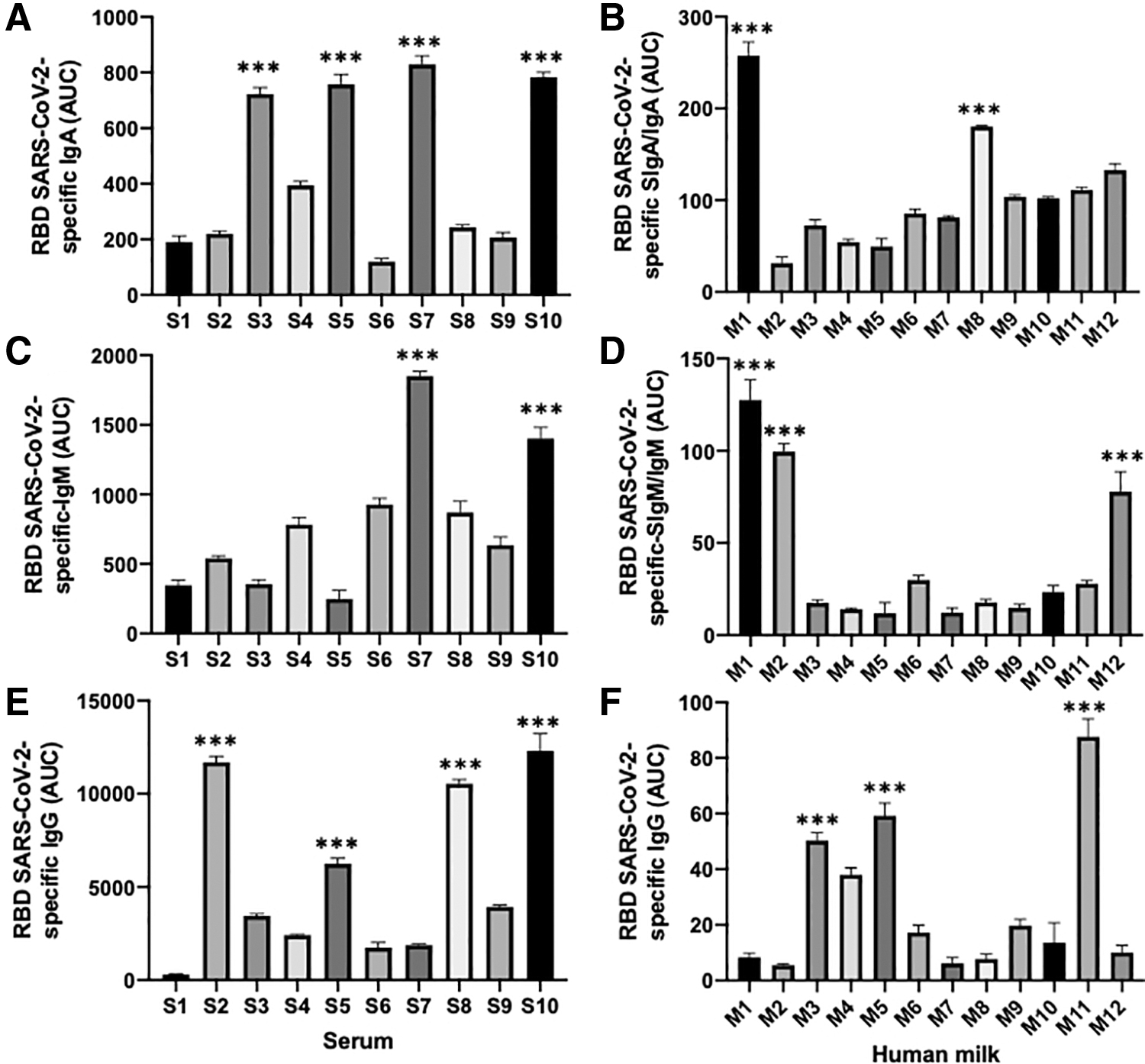
Among serum samples, SARS-CoV-2 RBD-specific antibodies had the highest AUC in S3, S5, S7, and S10 for IgA (Fig. 3A); S7 and S10 for IgM (Fig. 3C); and S2, S8, and S10 for IgG (Fig. 3E). Among human milk samples, SARS-CoV-2 RBD-specific antibodies had the highest AUC in M1 and M8 for SIgA/IgA; M1, M2 (Fig. 3B), and M12 for SIgM/IgM (Fig. 3D); and M3, M5, and M11 for IgG (Fig. 3F).
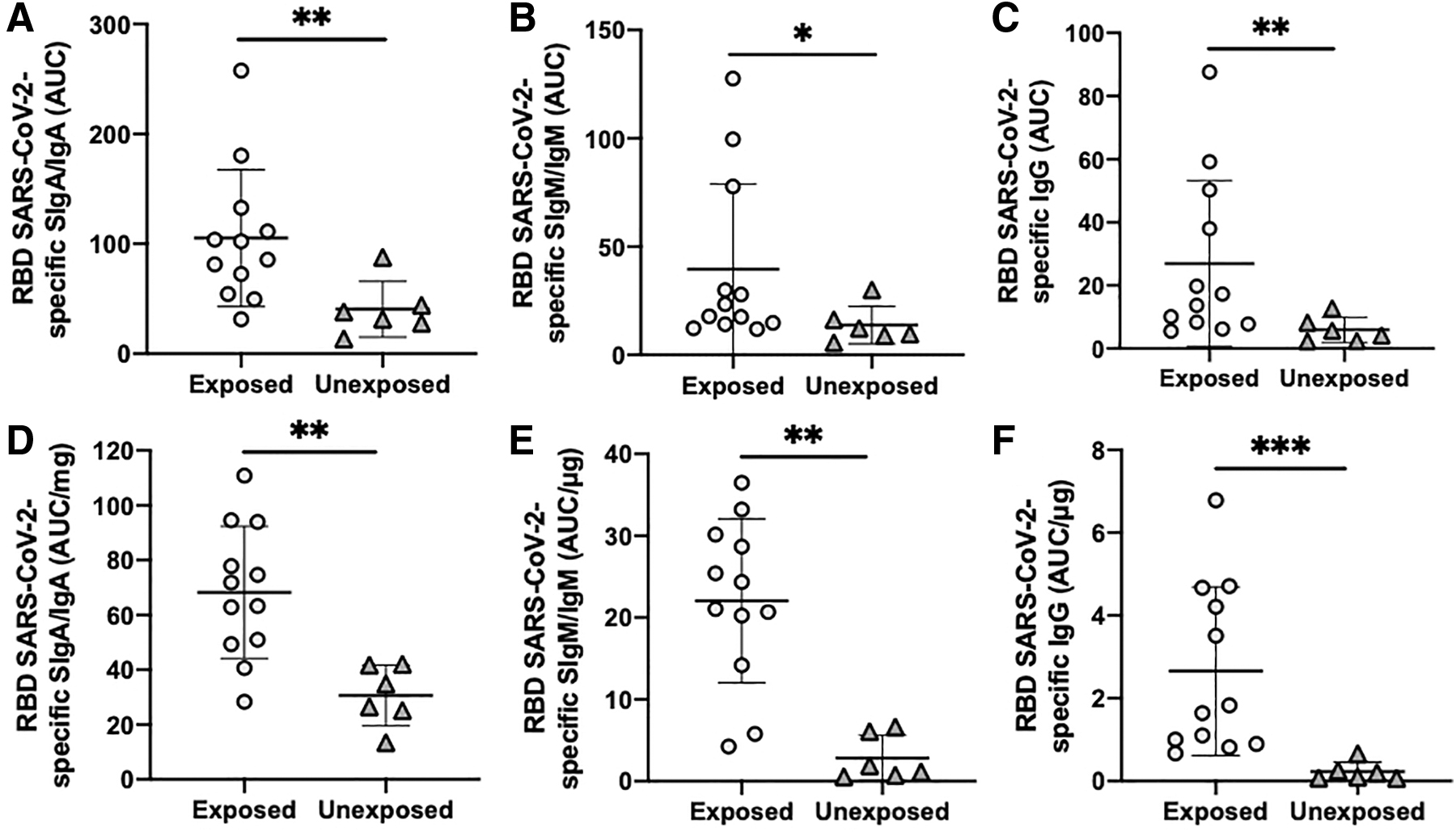
Comparison of titers (AUC) of human milk antibodies specific to the RBD of SARS-CoV-2 between COVID-19-exposed mothers and unexposed mothers.
COVID-19-exposed and unexposed mothers
AUCs of SARS-CoV-2 RBD-specific SIgA/IgA, SIgM/IgM, and IgG in human milk were 2.6- (p = 0.010) (Fig. 4A), 2.9- (p = 0.041) (Fig. 4B), and 4.8-fold (p = 0.010) (Fig. 4C) higher in the COVID-19-exposed mothers (recovered women who donated milk and had a +COVID-19 PCR test or COVID-19 symptoms) than in the unexposed mothers (women who provided milk from 2018 before the COVID-19 pandemic), respectively. AUCs per antibody concentration of SARS-CoV-2 RBD-specific SIgA/Ig, SIgM/IgM, and IgG in human milk were 2.3- (p = 0.002) (Fig. 4D), 7.7- (p = 0.001) (Fig. 4E), and 11.6-fold (p < 0.001) (Fig. 4F) higher in the COVID-19-exposed women than in the unexposed women, respectively.
Comparison of titers (AUC) of antibodies specific to the RBD of SARS-CoV-2 in human milk and serum samples from COVID-19-recovered mothers.
Effect of maternal factors on antibody levels
No correlation was observed between maternal age and antibody levels (concentration, AUC, and AUC/μg) for human milk and serum samples, except for IgG concentration in serum samples. The concentration of serum IgG decreased with increasing maternal age (p = 0.011) (Fig. 5A). The antibody levels from human milk samples were not affected by infant gender. The types of symptoms did not influence the antibody levels in milk or serum samples.
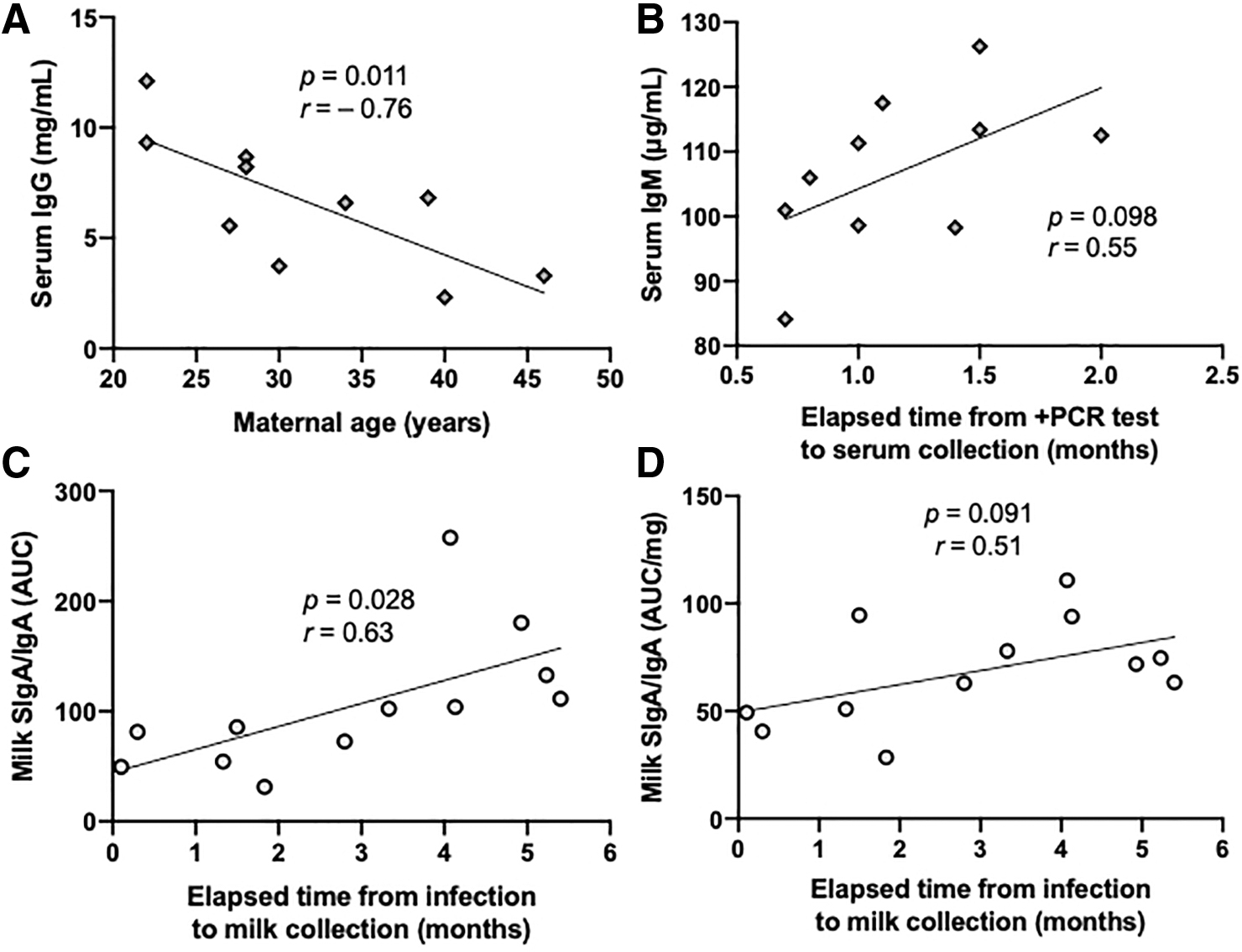
Effect of maternal age and elapsed time from infection to collection on the antibody levels.
Effect of elapsed time from infection to collection on antibody levels
The concentration of serum IgM tended to be positively correlated with the elapsed time from +PCR test to serum collection, but did not differ for the other antibody levels (p = 0.098) (Fig. 5B). Positive correlations were observed with the elapsed time from infection to milk collection for the SIgA/IgA titer (p = 0.028) (Fig. 5C), and correlations tended to be positive for SIgA/IgA concentration (p = 0.092) and SIgA/IgA titer/IgA concentration (p = 0.091) (Fig. 5D). No correlation was detected for SIgM/IgM or IgG from milk samples.
Standard curves of individual donors
The standard curves of individual donors (serum and human milk samples) are presented in Supplementary Figure S1A-S1I. The SARS-CoV-2 RBD-specific IgA titer was the highest in milk from mother 1 (M1) (Supplementary Fig. S1A) and mother 7 (M7) (Supplementary Fig. S1D) compared with other milk samples or serum samples. SARS-CoV-2 RBD-specific IgM and IgG titers in all human milk samples were lower than serum samples, except for IgM from M1.
Discussion
The present study demonstrated that SARS-COV-2 RBD-specific antibody binding capacity differed between human milk and serum samples from COVID-19-recovered women. When the AUCs were not divided by the antibody concentration, SARS-CoV-2 RBD-specific IgA, IgM, and IgG levels were higher in the serum group than in the human milk group. These observations are in accordance with Dong et al. 25 who showed that the serum SARS-CoV-2-specific IgG level was 292- to 2093-fold higher than human milk SARS-CoV-2-specific IgG from one mother who tested positive for SARS-CoV-2 PCR. However, the antibody specificity was not reported, and the titers of IgA and IgM were not measured. The titer (AUC) per antibody concentration was used to determine the antibody level specific to the SARS-CoV-2 RBD among the total antibodies from the same isotype in each sample. This measurement provides knowledge on the availability of antibodies in human milk for potential use in infant feeds. The titers of SARS-CoV-2 RBD IgM (AUC/μg of IgM) and IgG (AUC/μg of IgG) were higher in human milk samples than serum samples. On the other hand, the concentration of IgA was comparable between human milk and serum samples. The titer of SARS-CoV-2 RBD-specific IgA (AUC/mg of IgA) was higher in the serum group than the human milk group. The concentrations of IgA, IgM, and IgG in human milk6–8,26–29 and serum samples 5 were in the ranges found in previous studies.
Some women had greater antibody levels in human milk or serum samples than other women. We observed that the SIgA/IgA titer was positively correlated with elapsed time from infection to milk collection, but was not affected by maternal age and type of symptom. The concentration of serum IgG was negatively correlated with maternal age and positively correlated with the elapsed time from +PCR test to serum sample collection, but other antibody measurements were not changed. Our recent study showed that the duration of antibody levels reactive to the S1 or S2 subunit of SARS-CoV-2 in human milk varied between 3 and 4 months depending on the individual mothers and isotypes. 30 We did not find a specific time after COVID-19 infection with optimal IgA, IgM, and IgG levels when collecting human milk samples each month during a period of 4 consecutive months. 30 Dong et al. 25 showed that women had spike protein-specific IgG and IgA detected in human milk 2 weeks after the +PCR test and the highest antibody levels after 5 weeks, but no follow-up was performed before 2 weeks or after 5 weeks of postinfection. Pace et al. 31 demonstrated that RBD-specific IgA in human milk samples was detected from 3 to 20 days after the first day of COVID-19 symptoms, but no follow-up was performed after 20 days postinfection. Other factors influence antibody levels, including infection's severity, pre-existing immunity, 3 genetic factors, nutrition, and other factors affecting the immune response.7,32 Human milk with high SARS-CoV-2 RBD-specific antibody titers could be concentrated and purified to use as a supplement in infant feeds to reduce the neonatal risk of COVID-19 infection.
For both serum and human milk samples, some women (S1, S7, and M2) had higher levels of SARS-CoV-2 RBD IgM than IgG and IgA. Tosif et al. 33 also observed that the levels of S1 SARS-CoV-2-specific IgM from maternal serum were 1.1- and 8.5-fold higher than serum IgG and IgA, respectively, after 37 days postinfection. IgM is the first antibody to be produced during the primary infection. M2, S7, and S1 were collected at 55 days, 44 days, and <2 months after the confirmed COVID-19 PCR, respectively. As no correlation was detected between the IgM titer and elapsed time from infection to sample collection, other factors previously described could explain the difference in IgM production between women.
Most maternal serum samples had a higher titer of SARS-CoV-2 RBD IgG compared with IgA and IgM. IgG antibodies are primarily secreted after recovery from an infectious disease and last for months or up to 2 years. 34 Serum SARS-CoV-2-specific IgG was 11.8% after 7 days postinfection and increased progressively to 100% after 3 months. 34 On the other hand, most human milk samples had a higher titer of SIgA/IgA than SIgM/IgM and IgG. Fox et al. 4 also reported that SARS-CoV-2 RBD-specific SIgA was in a higher proportion in human milk samples compared with SARS-CoV-2-specific IgM and IgG after 14–30 days of postsymptoms. 4 SIgA is the most abundant antibody (80–90% of total Ig) in human milk, which explains the highest titer of SIgA/IgA among all other isotypes in human milk.
We demonstrated that titers of SARS-CoV-2 RBD SIgA/IgA, SIgM/IgM, and IgG in human milk samples were higher in COVID-19 mothers than in unexposed mothers (prepandemic 2018). These findings are in accordance with Fox et al. 4 reporting that SARS-CoV-2 RBD-specific SIgA, IgG, and IgM titers in human milk samples were higher in recovered COVID-19 mothers than in unexposed mothers (before December 2019).
The most frequent symptoms identified in the COVID-19-recovered mothers who donated human milk were fever (91.7%), cough (83.3%), fatigue (50%), nasal congestion (33.3%), body aches (16.7%), chills (16.7%), loss of taste/smell (8.3%), headache (8.3%), and sore throat (Supplementary Table S1). Observed symptoms in COVID-19-recovered women who donated serum samples were body aches (60%), loss of taste/smell (60%), fever (50%), fatigue (50%), headache (50%), cough (40%), chills (30%), breathing issues (30%), diarrhea (30%), congestion (20%), and chest tightness (20%) (Supplementary Table S2). These symptoms associated with COVID-19 infection were also often reported in previous studies. Common symptoms during pregnancy related to COVID-19 were fever, cough, sore throat, and headache. 22 Another study also observed that headache, cough, muscle aches, fever, sore throat, chills, and fatigue were the symptoms often reported during SARS-CoV-2 infection in pregnant and nonpregnant women aged between 18 and 44 years. 24 The symptoms experienced by the women who donated human milk or blood samples are likely related to mild COVID-19 infection. The type of symptom did not affect the antibody levels in this study. Whether mothers with severe symptoms have higher human milk antibody levels than mothers with mild symptoms during COVID-19 is still unknown. Future study is needed to compare the antibody levels in human milk between severe (hospitalization) and mild COVID-19 diseases.
Three limitations should be taken into consideration when interpreting the findings. First, the sample size for each group remained relatively small. However, we detected differences between human milk and serum sample groups even with this small size. Second, human milk and serum samples were not collected from the same women (paired samples). We could not collect blood samples from women who donated human milk due to the complexity of collecting blood during COVID-19. However, the maternal characteristics (age and health conditions) were comparable between mothers who donated serum and those who donated human milk. The elapsed time from infection to sample collection differed between serum and milk samples, but this factor did not correlate with antibody titers, except for human milk IgA. Variability of antibody levels between individuals can be increased by differences in pre-existing immunity, genetic factors, nutrition, and other factors affecting the immune response and likely affecting the results. Third, the neutralizing capacity of antibodies was not determined in this study.
Conclusions
Our study reveals that SARS-CoV-2 RBD-specific antibody titers differed between human milk and serum samples from COVID-19-recovered women. When the AUCs were not divided by the antibody concentration, SARS-CoV-2 RBD-specific IgA, IgM, and IgG levels were higher in the serum sample group than in the human milk group. The titers of SARS-CoV-2 RBD IgM (AUC/μg of IgM) and IgG (AUC/μg of IgG) were higher in human milk samples than serum samples. However, the titer of SARS-CoV-2 RBD-specific IgA (AUC/mg of IgA) was higher in the serum sample group than in the human milk group. Purification of SIgA from human milk is needed to evaluate the neutralizing capacity against SARS-CoV-2 spike-pseudotyped lentiviral particles and replication-competent live SARS-CoV-2. The future study will determine the dose–response and minimal effective dose required to neutralize SARS-CoV-2. Neutralizing antibodies are generally correlated with protection against reinfection. 35 Neutralizing SIgA from human milk could be used to prevent and treat COVID-19 in infants.
Footnotes
Authors' Contributions
V.D.-M. conceptualized and designed the study, carried out ELISAs and the statistical analysis, drafted the manuscript, and approved the final article as submitted. V.D.-M. has primary responsibility for the final content. C.D. helped V.D.-M. with recruitment of donors and completion of the survey. E.M. acquired funding for this study. C.D. and E.M. revised the article and approved the final article as submitted.
Acknowledgments
The authors thank all study participants for their valuable contributions.
Disclosure Statement
V.D.-M., C.D., and E.M. are employees at Medolac Laboratories.
Funding Information
The authors (V.D.-M., C.D., and E.M.) have received financial support from Medolac Laboratories, A Public Benefit Corporation, for the conduct of the study.