
Abstract
Background:
Aluminum exposure may originate from numerous sources, including antiperspirants. Aluminum toxicity can cause a wide range of neurological impairments. Infants are exposed to aluminum through human milk (HM), formulas, total-parenteral-nutrition and vaccines. Due to potential risk of toxicity to both infants and women, it has been advised that lactating women decrease their use of aluminum-based products and antiperspirants. Our study aimed to determine whether the use of aluminum-based antiperspirants (ABA) affects aluminum levels in HM.
Methods:
This cross-sectional study included healthy mothers who exclusively breastfed infants (1 week to 5 months). Questionnaires were used to collect data on demographics, antiperspirant use and aluminum exposure. Mothers were instructed to express HM during the morning at first breastfeeding session. Aluminum levels were measured by atomic absorption spectrometry with a 5 ppb limit of detection.
Results:
Fifteen of the 58 (26%) recruited mothers used an aluminum-free antiperspirant (AFA) and 43 (74%) used an ABA. The range of aluminum concentration in HM was 0–100.8 μg/L (mean 11.4 ± 17.4 μg/L). The median aluminum level (Q1–Q3) was 6.5 μg/L (5.2–11.9) and 5.2 μg/L (3.46–9.4) in the AFA and ABA groups, respectively (p = 0.19). The aluminum levels were not affected by maternal age, education, diet, number of children, infant age, lactation stage or self-reported aluminum exposure.
Conclusion:
The data from this preliminary study demonstrate that the use of an ABA by lactating mothers does not increase their HM aluminum content. Additional studies with a larger cohort are warranted to confirm these findings.
Introduction
Aluminum is the most abundant metal in the earth's crust and one that has no essential biological function. 1 Exposure to aluminum may originate from a variety of sources, including water, human milk (HM), infant formulas, various drugs, vaccines, cooking appliances, as well as personal care products, such as antiperspirants.1–4 Aluminum toxicity can cause a wide range of neurological impairments in both children and adults.2,3,5
Aluminum is absorbed through the gastrointestinal (GI) system and through inhalation, transdermal and parenteral routes, and eliminated mostly by the kidneys and about 2% through the bile.2,5 GI absorption is considered to be low, with only 0.2–0.4% of the ingested aluminum being transferred to the bloodstream. 6 Limited data exist on human skin absorption of aluminum in vitro and in vivo following topical application. 7 Transdermal absorption is reported to be less than 0.01% in adults with healthy skin, however, absorption may be more significant in infants and in adults with skin lesions or shaved skin.7–10
Infants are exposed to aluminum via the GI system through HM and infant formulas, via parenteral route through total parenteral nutrition (TPN) and via intramuscular exposure through aluminum-adjuvanted vaccines.6,11 Infants, especially preterm neonates, are at particular risk for aluminum toxicity due to the immaturity of their GI wall, their blood–brain barrier, and their renal system. Their limited capacity to excrete aluminum may result in its toxic accumulation.2,12 TPN may cause aluminum intoxication since it bypasses the intestinal barrier. 12 Fewtrell et al. 11 found that infants exposed to aluminum-containing TPN were at risk for developmental delays and altered bone metabolism.
In women, aluminum levels were found to be generally higher in breast milk than in blood serum, which may suggest that aluminum accumulates in breast milk. 13 In addition, data on the link between breast cancer and the use of aluminum-based antiperspirants (ABA) are conflicting.13–15
Aluminum levels measured in a wide array of infant formulas were found to be higher than in HM, especially in hydrolyzed, preterm, and soy-based formulas, with ranges of 176 to 700 μg/L.12,16–19 Less is known about the amount of aluminum in HM, with a number of studies having supported a typical average of 40 μg/L.6,12,20–22
Potential risks of aluminum exposure to women and infants have been reported, leading to their having been advised to reduce their use of aluminum-based cosmetic products and antiperspirants.12,23 We therefore designed the current study to test the hypothesis that the use of ABA may lead to an increase in aluminum content in HM.
Materials and Methods
This cross-sectional pilot study was approved by the Institutional Ethics Committee of Tel Aviv Medical Center, Tel Aviv, Israel (0070-18-TLV). A written informed consent was obtained from all participating mothers.
Participants
Healthy mothers, who exclusively breastfed their infants, were recruited through an advertisement posted on the Tel Aviv Medical Center Facebook page, in several baby-related forums on the internet, and at the “Lis” Maternity Hospital at the Tel Aviv Medical Center between December 2018 and June 2019. Mothers with a history of chronic illness, chronic medication treatment, breast cancer, plastic surgery of the breast, and breast implants were excluded.
Maternal demographic data were collected by means of a questionnaire whose items included age, number of children, ethnic origin, education, occupation, diet, and previous breastfeeding experience. Details (brand and aluminum content) of the antiperspirant routinely used by the mothers were recorded. We collected infant gestational age (GA) and infant age at the time of HM sampling. HM samples were collected between 1 week (transitional milk) and 5 months (mature milk) after birth.
Data on other possible sources of aluminum exposure were collected with a 5-point Likert scale measuring the frequency of use according to the following score: 1 = no use at all, 2 = use less than once a month, 3 = use several times a month, 4 = use several times a week, and 5 = daily use. The mothers were asked to rate the frequency of use of aluminum appliances (aluminum cans, coffee capsules, aluminum cooking appliances, and so on), aluminum-containing drugs (e.g., antacids and so on together with their brand names), aluminum-containing food additives (including vitamin supplements), and aluminum-based cosmetic products (providing the brand names).
For statistical analysis, “aluminum exposure” per participant was defined as the sum of points on the Likert scales, thereby ranking the amount of reported exposure from a minimum of 4 (none) to a maximum of 20 (daily exposure for all categories).
HM samples
Mothers were instructed to express 5 mL of HM (manually or by pump) at the time of the first morning breastfeeding session. The milk samples were collected by a single researcher (M.R.) and stored at −20°C until thawed and analyzed.
Laboratory methods
Aluminum levels were measured by atomic absorption spectrometry with a limit of detection of 5 ppb at the Clinical Pharmacology and Toxicology Unit of the Assaf Harofeh Medical Center. The operator who performed the analyses was blinded to the sample details (name, group, and lactation time).
Statistical analyses
The statistical analyses were performed with the Minitab Statistical Package, version 16 (Minitab, State College, PA). Fisher's exact test was applied for categorical variables and Mann–Whitney U tests for continuous variables. Correlation was evaluated by the Spearman rho test. The results are expressed as mean ± standard deviation (range) and as median (Q1–Q3). Categorical parameters were expressed as percentages. A p-value ≤0.05 was considered significant.
Results
A total of 72 mothers agreed to participate in the study, of whom, 4 were excluded due to chronic medication treatment, 1 due to chronic illness, and 9 due to the inability to ensure proper delivery and storage of the HM samples. Of the 58 mothers who were included in the study, 15 used an aluminum-free antiperspirant (the AFA group) and 43 used an ABA (the ABA group). The major demographic characteristics of the participants are depicted in Table 1. The AFA and ABA groups did not differ in terms of maternal age, education, diet, previous breastfeeding experience, number of children, infant age at HM sampling, infant GA, and extent of reported aluminum exposure.
Demographic Characteristics of the Participants (n = 58)
Data are expressed as mean ± standard deviation (range) and n (%).
ABA, aluminum-based antiperspirants; AFA, aluminum-free antiperspirant; NS, not significant.
The overall mean of aluminum concentration in HM was 11.4 ± 17.4 μg/L with a range of 0 to 100.8 μg/L. In the AFA group, the mean (range) of aluminum concentration was 12.18 ± 13.51 (3.77–51.02), with a median (Q1–Q3) of 6.5 μg/L (5.2–11.9). In the ABA group, the mean (range) of aluminum concentration was 11.1 ± 18.7 (0–100.8), with a median (Q1–Q3) of 5.2 μg/L (3.46–9.4). There was no statistically significant difference in aluminum content between the groups (p = 0.19) (Table 2).
Aluminum Concentration of Human Milk by Category
Data are expressed as median (Q1–Q3).
Transitional HM = 1 week–2 weeks.
Mature HM = 1 month–5 months.
HM, human milk.
The aluminum contents in the HM of mothers who breastfed for the first time did not differ from those of mothers with previous breastfeeding experience (p = 0.54). Aluminum contents also did not differ between omnivorous and vegetarian/vegan mothers (p = 0.46). Maternal age, education, stage of lactation (calculated by infant age), and number of children did not affect the aluminum content of the HM (rs = 0.077, p = 0.56; rs = −0.04, p = 0.75; rs = 0.209, p = 0.11; rs = 0.03, p = 0.82; respectively) (Table 2).
There was no correlation between the aluminum level of HM and the calculated “aluminum exposure” score (rs = 0.117, p = 0.381). Comparison of the median frequency of aluminum exposure between the ABA and AFA groups revealed no differences in any of the predefined categories, and that the total overall exposure was similar in both groups (Table 3). The reported frequencies of exposure for each category are shown in Figure 1.
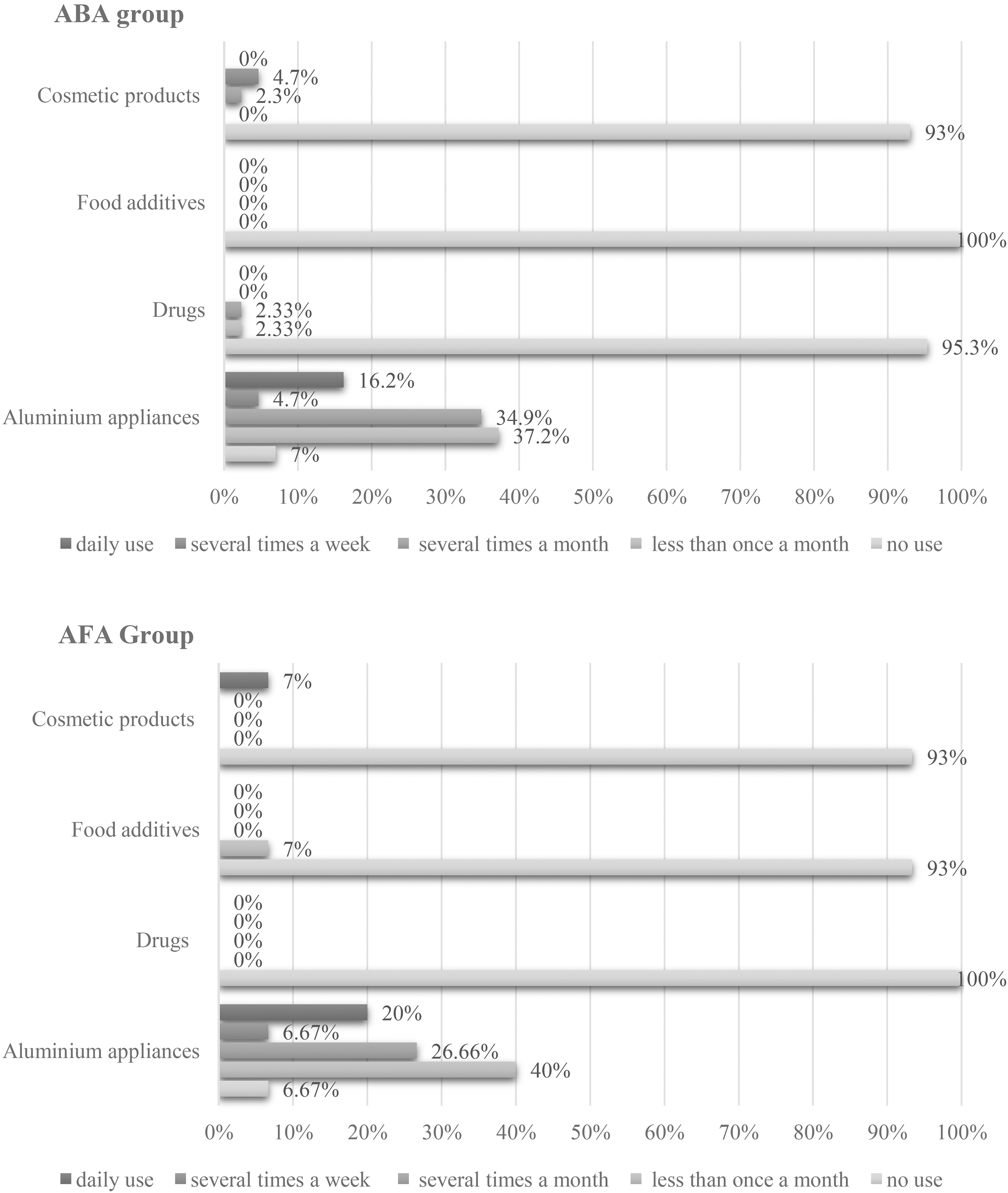
Reported aluminum exposure by group.
Aluminum Exposure–Frequency of Use a (n = 58)
Data are expressed as median (range).
Frequency of use:1 = no use, 2 = less than once a month, 3 = several times a month, 4 = several times a week, and 5 = daily.
Sum of points on Likert scales, from a minimum of 4 (no reported exposure) to a maximum of 20 (reported daily exposure in all 4 categories) per participant.
Discussion
The results of the current study revealed that the overall low aluminum content in HM was similar in the ABA and AFA groups. Pregnant and lactating women have been advised to decrease the use of aluminum-based cosmetic products and ABA due to the potential risks of aluminum exposure.12,23 We sought to test the hypothesis of whether the use of ABA has any impact on the level of aluminum in HM.
The aluminum concentrations in HM reported in the scientific literature vary considerably. Based on works done in the late 80s and 90s numerous studies have supported a typical average of 40 μg/L, 6,12,20–22 while numerous other publications reported aluminum averages ranging between 9 and 380 μg/L.1,22,24–33 The level of aluminum in HM samples collected in our cohort was in the lower range, with a mean of 11.4 μg/L, comparable to values reported by others.1,29,32
There are limited data on human skin absorption of aluminum following topical application. 7 In 2004, Guillard et al. published a case report describing antiperspirant use that led to a toxic aluminum level in plasma and urine along with clinical symptoms of bone pain and fatigue. 34 However, most publications on aluminum transdermal absorption suggested a rather low rate of absorption. In 2008, the Agency for Toxic Substances and Disease Registry (ATSDR) noted that aluminum is essentially not absorbed transdermally, 35 based on the report of Flarend et al. in 2001 who demonstrated transdermal absorption equivalents to 0.012% of the applied dose. 8 Moreover, in 2018, Rianne de Ligt et al. reported a mean estimated transdermal absorption of 0.0094%. 7 Those two studies used radioisotope 26 Al to measure absorption. In 2020, after initiating additional clinical studies (TNO studies) on this topic, a regulatory review by the Scientific Committee on Consumer Safety (SCCS) concluded that the calculated dermal bioavailability of 0.00052% is an appropriate value for use in risk assessment. 36 Letzel et al. recently showed that daily use of an ABA for 14 days did not increase plasma aluminum concentration. 10 We found no increased aluminum content in the HM samples of the ABA mothers compared to the AFA mothers in the current work. Both groups had similar aluminum exposure scores, suggesting low transdermal absorption and passage into HM, similarly to the previous findings on low transdermal absorption to blood and urine.
We also did not find any correlation between aluminum content in HM and maternal age, stage of lactation, or number of children. This absence of correlation between levels of aluminum and different stages of lactation was also reported by Taravati et al. 22 who compared HM samples taken at various time points of lactation (1 through 12 months), and by Fernandez-Lorenzo et al. 30 who found no significant differences between colostrum, intermediate-stage milk, and mature-stage milk. Interestingly, Chao et al. reported that colostrum samples contained higher levels of aluminum than transitional or mature HM. 32
Environmental and dietary exposure to aluminum and its effect on HM has been discussed in the literature with conflicting findings. There are some reports that the maternal diet may affect aluminum levels in HM,3,22 while others 32 found no significant influence of maternal dietary habits on metal concentrations in breast milk. Taravati et al. suggested that the high level of aluminum concentrations found in drinking water was a possible environmental factor that contributed to the high level of 191 μg/L aluminum in HM described in their study. 22 Likewise, we could not establish any correlation between the aluminum exposure score and aluminum levels in HM samples according to the results of our assessment of self-reported aluminum exposure. Furthermore, we found no difference in aluminum content in HM between mothers who followed a vegan/vegetarian or omnivorous diet.
Our preliminary findings should be interpreted in the context of a relatively small cohort of 58 participants. The questionnaire used for aluminum exposure assessment focused on the frequency and not the quantity of exposure, and relied on maternal self-reporting. In addition, although details on the routinely used antiperspirant were collected, its duration of use was not documented, thereby limiting our knowledge on the extent of exposure to the two types of antiperspirants.
Conclusions
The data that emerged from this preliminary study demonstrated that the use of ABA by lactating mothers does not necessarily increase their HM aluminum content. Additional studies with a larger cohort are warranted to confirm these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.