
Abstract
Introduction:
Insufficient milk supply is the most common reason for premature breastfeeding cessation. Breast hypoplasia is one reason why women may be inherently unable to make a full milk supply. This review aimed to systematically explore the relationship between breast hypoplasia and breastfeeding duration, milk supply, and lactation onset.
Materials and Methods:
Medline, CINAHL, ProQuest Central, and the Cochrane Library databases were searched using the keywords “insufficient glandular tissue” or “mammary hypoplasia” or “breast hypoplasia” or “mammary gland hypoplasia” or “droopy breasts” or “snoopy deformity” or “tubular breast*” or “tuberous breast*” AND breastfeeding or “breast feeding” or breast-feeding or lactation. After initially screening 20 records, including reference lists, 9 full texts were assessed for eligibility; 2 were excluded as no breastfeeding outcomes were reported, leaving 7 studies (N = 42 women).
Results:
The studies in this review drew on results from the oldest included study and plastic surgery literature to define breast hypoplasia. Most women in this review (40/42) ceased exclusive breastfeeding before 1 month postpartum. One case study reported 24-hour milk production, which was 52 mL at 26 weeks postpartum.
Conclusion:
The relationship between breast hypoplasia and breastfeeding outcomes is underresearched. The co-occurring medical conditions (e.g., polycystic ovary syndrome) of some women provide avenues for future research into the possible pathogenesis of breast hypoplasia resulting in insufficient milk supply. Research is needed to evaluate the reliability of measuring and classifying markers of breast hypoplasia, and prospective studies can help determine the role of breast hypoplasia in milk production. PROSPERO registration number CRD42020191228.
Introduction
Worldwide, insufficient milk supply is the most common reason women give for ceasing breastfeeding early.1–3 Various presentations of insufficient milk supply can be described, including a primary, secondary, or perceived insufficient milk supply.4,5 A primary insufficient milk supply results when a woman is physiologically unable to make a full milk supply to meet her infant's needs, while a secondary insufficient milk supply results from suboptimal breastfeeding management.4,5 A perceived insufficient milk supply is defined as when a woman believes she is not making sufficient breast milk to satisfy her infant's needs regardless of whether a primary or secondary insufficient milk supply exists or not. 5 It is unknown what proportion of women who report ceasing breastfeeding early due to an insufficient milk supply have a primary, secondary, or perceived insufficient milk supply.
There are a number of reasons why women may have a primary insufficient milk supply, including previous breast surgery or conditions such as diabetes, obesity, and polycystic ovarian syndrome (PCOS), which may interfere with hormones involved with breast development and milk synthesis.6–11 Breast hypoplasia refers to underdeveloped breasts and is another possible reason for primary insufficient milk supply.12,13 Common features of breast hypoplasia listed by breastfeeding textbooks include marked breast asymmetry, tubular shaped breasts, and a wide intramammary width.14,15 The same breastfeeding textbooks cite a case study and a case series as evidence that a primary insufficient milk supply is associated with breast hypoplasia.16,17
The terms breast hypoplasia and insufficient glandular tissue (IGT) are commonly used interchangeably in the context of a woman's ability to produce a full milk supply. However, Cassar-Uhl 12 indicated that the appearance of “hypoplasic breasts” does not always equate to an inherent inability to make a full milk supply, and hence reserves the term IGT for when there is a confirmed inability to make a full milk supply.
Because of the previous links between insufficient milk supply and breast hypoplasia, the objective of this review is to systematically explore the relationship between breast hypoplasia and breastfeeding duration, milk supply, and the onset of lactation.
Methods
Search strategy
Reporting for this systematic review followed the Preferred reporting items for systematic review and meta-analysis (PRISMA) checklist for systematic reviews (Supplementary Table S1). 18 The study protocol was registered with the University of York Centre for Reviews and Dissemination International prospective register of systematic reviews (PROSPERO registration number CRD42020191228). The following databases were searched on December 19, 2019, and again on January 21, 2021: Medline, CINAHL, ProQuest Central, and the Cochrane Library using the keywords “insufficient glandular tissue” or “mammary hypoplasia” or “breast hypoplasia” or “mammary gland hypoplasia” or “droopy breasts” or “snoopy deformity” or “tubular breast*” or “tuberous breast*” AND breastfeeding or “breast feeding” or breast-feeding or lactation. No restrictions were placed on publication date. A full electronic search strategy for the Medline database is presented in Supplementary Table S2. The PRISMA-P 2015 protocol for systematic reviews and meta-analyses was used to guide this review (Fig. 1). 18 A manual search of the reference lists of included studies was also conducted to locate relevant publications.
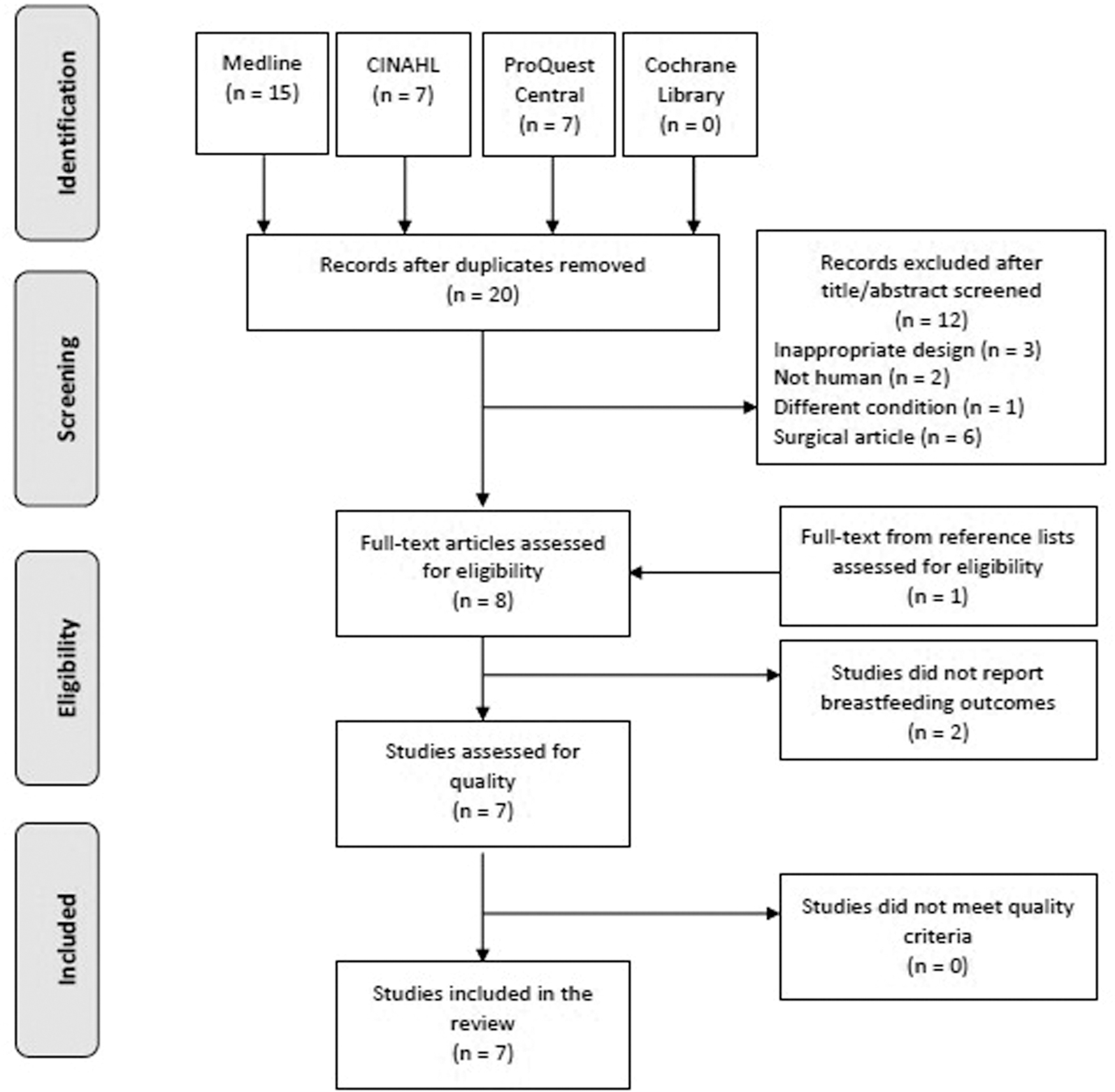
Preferred reporting items for systematic review and meta-analysis flowchart.
Inclusion and exclusion criteria
As described in the PROSPERO registry, predefined inclusion and exclusion criteria were set for the review, including type of participants, type of publication and study design, and context of studies.
19
Peer-reviewed observational (including case studies, case series, cohort studies, case–control studies, and cross-sectional studies) or experimental studies (including randomized controlled and quasi-experimental designs) reporting primary data on an association between breast hypoplasia and breastfeeding outcomes in breastfeeding women were included in this review. The primary outcome for this review was the duration of exclusive breastfeeding. Secondary outcomes included the duration of partial breastfeeding, timing of secretory activation (onset of lactation), and maternal 24-hour milk production. The outcome definitions used in this review were as follows:
Exclusive and partial breastfeeding: in this review, exclusive breastfeeding means that the infant only receives breast milk from his/her own mother since birth, and partial breastfeeding means that the infant receives a combination of the mother's own breast milk as well as formula, donor milk, or solid food.
20
Secretory activation 24-hour milk production: research on term infants demonstrates the intake of breastfed infants varies from feed to feed.
26
Hence, to accurately determine a woman's overall milk supply, test weighing an infant before and after every feed in a full 24-hour period (as well as measuring any milk expressed in the same 24-hour period) is necessary.
26
Breast hypoplasia was the exposure of interest in this review. Breast hypoplasia may be the result of any etiology or association such as congenital syndromes (e.g., Poland syndrome), chest wall deformities (e.g., pectus excavatum), or secondary to abnormal breast development.27,28 Participants of interest for this review were women with breast hypoplasia from any geographical region and of any ethnicity, who had given birth and had an intention to breastfeed. No restrictions were placed on publication date or language.
Review articles, conference proceedings and abstracts or low-quality studies defined as three or more questions rated “No” or “Unclear” according to Joanna Briggs Institute (JBI) Critical Appraisal Checklists, 29 and women who had breast surgery were excluded from this review.
Quality appraisal
JBI Critical Appraisal Checklists were used for the quantitative study designs included in this review. 29 The appraisal process was independently undertaken by two reviewers. Any disagreement was resolved by a third reviewer. Reviewers identified strengths and weaknesses, and validity and biases of each study by answering standardized questions with “Yes, No, Unclearm or Not applicable.” If any study had more than three “No” or “Unclear” responses, the study was excluded.
Data extraction
Data extracted included (i) authors, year of publication, and country; (ii) study design; (iii) aim of study; (iv) participants; (v) breast hypoplasia definition; and (vi) breastfeeding outcomes. In one of the included studies, the corresponding author was contacted to determine the age of the women with breast hypoplasia. 30
Data synthesis
Due to the studies' heterogeneity, it was not possible to perform meta-analyses. Narrative synthesis with tabulation of studies was used to summarize data. This review reports breastfeeding outcomes for the women with breast hypoplasia identified in the included studies. Ethical approval was not required for the research because it did not involve human participants.
Results
Search outcomes and assessment of methodological quality
As shown in the PRISMA flowchart (Fig. 1), the literature search resulted in a total of 29 records. After removal of duplicates, 20 records remained. Following screening of titles and abstracts, a total of eight full articles were assessed further for eligibility. Two of these studies did not report any breastfeeding outcome and thus were not included in this review.31,32 One additional record, Huggins et al., 16 which appeared to fit the inclusion criteria, was identified from the reference lists. These seven full texts were assessed for their quality using the relevant JBI assessment of methodological quality checklist tool. 29 The quality indicators for these seven studies are presented in Supplementary Table S3, JBI methodological quality assessment. All seven studies were rated as acceptable quality and included in the review. The quality appraisal process was independently undertaken by two reviewers with 100% agreement.
Study characteristics
Table 1 provides details of the reviewed studies. The publication dates of the studies ranged from 1985 to 2019 with one, one, two, and three being from the 1980s, 1990s, 2000s, and 2010s, respectively. Of the seven included studies, six were case studies4,17,30,33–35 and one was a case series. 16 Most of the studies were conducted in the United States of America (n = 4), with the remaining conducted in Australia (n = 3). Sample sizes ranged from 1 woman to 34 women (median = 1) and, where age was reported, the age of participants varied between 17 and 39 years of age. Almost all study outcomes were self-reported. In one case study, 24-hour milk production was assessed. 30
Summary of Included Studies
Range of normal milk production between ∼500 and 1,000 mL/24 hours with a mean of 750–800 mL/24 hours. 21
BMI, body mass index; EBF, exclusive breastfeeding; G, gravida; IGT, insufficient glandular tissue; P, parity; PBF, partial breastfeeding; PCOS, polycystic ovary syndrome; SA, secretory activation.
Definition of breast hypoplasia used in the studies
The oldest of the included studies, Neifert et al., 17 reported IGT as a “previously undescribed entity” and described three cases of lactation failure reported to be due to IGT characterized by the following:
A previous history of lactation failure in close female relatives;
Obvious abnormal development of at least one breast;
The absence of notable breast changes in pregnancy;
A failure of postpartum engorgement; or
Inadequate milk production despite appropriate breastfeeding management.
Subsequent studies4,16 drew on results from Neifert et al. 17 as well as plastic surgical literature36,37 to describe breast hypoplasia. From the plastic surgery literature, Chan et al. 37 used the following criteria to define tuberous deformity:
Lower quadrant hypoplasia (medial, lateral, or entire);
Subareolar skin deficiency resulting in elevated inframammary fold;
Breast base constriction;
Large nipple areola complex; and
Breast parenchyma herniation.
A surgical article by von Heimburg et al. 36 described the following four types of tuberous breast deformities:
Type 1—Hypoplasia of the lower medial quadrant.
Type 2—Hypoplasia of the lower medial and lateral quadrants, sufficient skin in the subareolar region.
Type 3—Hypoplasia of the lower medial and lateral quadrants, deficiency of skin in the subareolar region.
Type 4—Severe breast constriction, minimal breast base.
The most recent of the included studies30,33,35 used the descriptions of breast hypoplasia provided by Huggins et al. 16 to define breast hypoplasia. Huggins et al. 16 identified the following six features they associated with low milk supply due to hypoplasia:
Minimal breast tissue in the inferomedial and inferolateral breast quadrants;
A noticeable difference in shape or size between the woman's breasts;
A wide intramammary space (≥3.8 cm or 1.5 inches);
Stretch marks on the breasts;
A lack of pregnancy breast changes; or
A lack of engorgement postpartum.
Furthermore, Huggins et al. 16 modified the von Heimburg et al. 36 breast hypoplasia classification to come up with a new breast hypoplasia classification as follows:
Type 1—Round breasts, normal lower medial and lateral quadrants
Type 2—Hypoplasia of the lower medial quadrant
Type 3—Hypoplasia of the lower medial and lateral quadrants
Type 4—Severe constrictions, minimal breast base
Bodley and Powers only vaguely described breast hypoplasia by reporting the case had a lack of breast growth during pregnancy. 34
Co-occurring medical conditions
Information about co-occurring medical conditions (or lack thereof) was provided in five of the seven included studies or a total of 38 women. Out of the 38 women, 34 were reported to have no fertility issues or previous breast surgery, 16 1 woman was reported to have PCOS, including fertility issues and menstrual cycle dysfunction, 30 1 woman had fertility issues related to a luteal phase defect, 34 and 2 women were reported to have unremarkable obstetric, medical, surgical, family, and social histories.4,35
Breast hypoplasia and breastfeeding outcomes
Table 1 displays the outcomes of interest in this review: timing of secretory activation, breastfeeding duration (exclusive and partial), and 24-hour milk production. The primary outcome of exclusive breastfeeding duration was reported in all of the seven studies. Partial breastfeeding was reported in all, timing of secretory activation in six,4,16,17,33–35 and 24-hour milk production in one 30 of the seven studies.
Primary outcome
Exclusive breastfeeding duration
The duration of exclusive breastfeeding since birth in the studies was estimated by the reported introduction of formula. One study 33 reported the exclusive breastfeeding duration of one woman over three of her five lactations, which ranged from 13 days to 5 weeks. Data from 42 women in total from the seven studies were available about exclusive breastfeeding duration. Almost all women (40/42; 95%) had ceased exclusive breastfeeding before 1 month.
Secondary outcomes
Partial breastfeeding duration
The durations of partial breastfeeding were at least 1 month 16 ; at least 2 months 30 ; around 11 weeks 35 ; 5 months 17 ; 6 months 17 ; 7 months4,33; and at least 1 year.17,34 One study reported the partial breastfeeding duration of one woman over five lactations, which ranged from 3 weeks to 4 years. 33
Data from 42 women from the seven studies were available about partial breastfeeding duration. All these women achieved at least 1 month of partial breastfeeding. Given that the information pertaining to partial breastfeeding duration for 34 of these 42 women was limited by the length of follow-up (i.e., 1 month), 16 it is possible that this duration could have been longer. Furthermore, the next shortest length of partial breastfeeding duration provided (at least 2 months) was limited by the length of follow-up. 30 No article reported the proportion of infant diet from other sources.
Timing of secretory activation
In the six studies that provided information on the timing of secretory activation, it was at least delayed in four4,16,33,34 and reported to not occur in two.17,35
Twenty-four-hour milk production
Only one study reported 24-hour milk production, which was a total of 52 mL at 26 weeks postpartum. 30 The 24-hour milk production measurement was undertaken by the Hartmann Human Lactation Research Group at the University of Western Australia, whereby the infant was weighed before and after every breastfeed for 24 hours using electronic scales sensitive to ±2 g. 38
Discussion
For most breastfeeding conditions, the number of studies increases over time. For example, searching PubMed for studies related to breastfeeding and tongue-tie identified 3 published in the 1980s, 6 in the 1990s, 34 in the 2010s, and 209 in the 2010s. In addition, for studies related to mastitis (limited to humans), 547 were published in the 1980s, 479 in the 1990s, 729 in the 2000s, and 1,102 in the 2010s. However, for breastfeeding and breast hypoplasia, only one article was published in the 1980s and 1990s, two in the 2000s, and three in the 2010s. This demonstrates the significant lack of research devoted to investigating this condition.
For the women in this review for whom there was information about exclusive breastfeeding duration, only 5% exclusively breastfed for at least 1 month. In comparison, in the United States of America, based on cellular telephone sampling, 59% of infants were exclusively breastfed for 1 month. 39 In Australia, based on results from a large-scale, specialized, national survey of infant feeding practices, 56% of infants were exclusively breastfed to the first completed month postpartum. 40 However, no firm conclusions can be drawn from these comparisons due to the small numbers of participants included in this review.
All the women included in this review partially breastfed for at least 1 month. In comparison, in the United States of America, 80% of infants are provided with any breast milk to 1 month, 39 and in Australia, 75% of infants are provided with any breast milk to the first month. 40 The discrepancy between the rates of exclusive breastfeeding and partial breastfeeding among the women in this review may reflect the strength of the women's desire to breastfeed. The women in the reported case studies were likely to have a strong intention to breastfeeding, as exemplified in two reports. Thorley reported that the case “had always wanted to breastfeed.”33(p. 14) Similarly, Neifert et al. reported that case one “had planned to breastfeed and attended La Leche League meetings for several months before delivery.”17(p. 824)
By 2 weeks, the 24-hour milk production of women of full term exclusively breastfed infants remains relatively constant up to 6 months, with a mean of 750–800 mL per 24 hours and a range of 500–1,000 mL per 24 hours.21,26 In comparison, the 24-hour milk production reported by McGuire and Rowan of 52 mL at 26 weeks postpartum is extremely low. 30 However, no conclusions can be made relating to the potential effect of breast hypoplasia and 24-hour milk production based on a sample size of one.
The co-occurring medical conditions of some women included in this review provide some avenues for future research into the possible pathogenesis of breast hypoplasia resulting in primary insufficient milk supply. For example, McGuire and Rowan described a case with PCOS and breast hypoplasia, who experienced insufficient milk supply. 30 Endocrinological changes associated with PCOS (such as insulin resistance,41,42 hyperandrogenism, 43 and low progesterone levels 9 ) may impact pubertal breast development and/or alveolar growth in pregnancy depending on the timing of onset.
Studies have reported conflicting results when examining the breastfeeding success in women with PCOS.9,43 A case series by Marasco et al. reported insufficient milk supply in three women with PCOS. 9 A case–control study by Vanky et al. of 36 women with PCOS versus 99 controls found that fewer women with PCOS exclusively breastfed to 1 month compared to women in the control group (75% versus 89%); however, no difference was found in breastfeeding rates at 3 and 6 months postpartum. 43 The heterogenous results may reflect the range of severity of PCOS. 44
Various syndromes have been linked with breast hypoplasia such as Poland and ulnar-mammary syndromes. 45 Poland syndrome is a rare congenital disorder, which encompasses a range of chest and upper arm anomalies. 27 Ulnar-mammary syndrome is a congenital genetic disorder characterized by ulnar defects, apocrine gland hypoplasia, and hypoplasia/aplasia of the breasts/nipples. 46 Bamshad et al. present clinical descriptions of 33 members with ultra-mammary syndrome from six family generations. 31 Seven, 12, and 13 women in this study had “hypoplastic,” “normal,” or “unknown” breasts, respectively. 31 Three women had “normal” lactation combined with “normal” breasts. 31 Three women had “absent” lactation, two and one of whom had “normal” and “unknown” breasts, respectively. 31 One woman had “diminished” lactation and “normal” breasts. 31 Despite there being no studies in this review regarding breastfeeding outcomes for women with these syndromes, it is important to be aware of their existence.
In addition, case reports have identified congenital conditions resulting in breast hypoplasia, which clinicians should be aware of. For example, Velter et al. reported a case of a 19-year = old woman with a noticeably smaller right breast compared to her left, who had a right breast hemangioma diagnosed in infancy. 47 Given that congenital hemangiomas have been associated with Poland syndrome, 48 Velter et al. proposed that cases of breast hypoplasia and infantile hemangioma could be syndromic infantile hemangiomas with breast malformation. 47
This review demonstrated the lack of robust definitions and classifications of breast hypoplasia in the context of breastfeeding. The most commonly reported markers of breast hypoplasia are those identified by Huggins et al. 16 These variables have not been quantified and their validity and reliability remain unknown. In addition, there is no agreed list of features to diagnose breast hypoplasia, nor is it known which factors may be more or less relevant when it comes to a woman's ability to make a full milk supply.
Strengths and limitations
To our knowledge, this was the first systematic review to assess the association between breast hypoplasia and breastfeeding outcomes. The major strength of this study is its design. Being a systematic review, all the evidence on the subject was collected in a systematic way.
It is important to indicate the limitation in interpreting the results of the review. For two of the seven included studies, no information about the women's medical history was provided.17,33 Since various factors have the potential to contribute to a primary insufficient milk supply, this information would be helpful for readers. Also, selection bias is a risk for the case series, which did not recruit consecutive participants, but rather recruited women who demonstrated characteristics the researchers identified as being suggestive of breast hypoplasia. 16 In addition, the lack of reliable methods for assessing breast hypoplasia is another limitation. 49
Overall, the most significant limitations of this review are that only seven studies were eligible, in that, they explored the association between breast hypoplasia and breastfeeding outcomes, and all the studies included were either case studies or case series. Hence, the overall quality and total number of participants are low and the review could only provide a descriptive analysis rather than report on any strength of association.
Future research
Future research is needed to evaluate the reliability of markers of breast hypoplasia and their association with breastfeeding outcomes. Such research would be helpful to ensure consistency in quantifying or categorizing markers of breast hypoplasia, and may pave the way for the development of diagnostic tools and treatment for women with breast hypoplasia, enabling more women to reach their breastfeeding goals.
Anecdotal reports from lactation professionals working with postpartum women suggest breast hypoplasia is a rare condition.4,17 Case studies provide a useful starting point when researching such conditions as they help form hypotheses that can be further investigated. 50 Where relevant, case studies should include the presenting concerns, clinical findings, diagnoses, interventions, outcomes (including adverse events), follow-up, rationale for any conclusion, and any key messages. 51 Future case studies or case series reporting breast hypoplasia and breastfeeding outcomes should include the following (whenever possible): breast development, medical and reproductive histories, family history of insufficient milk supply, lactation history, and breast examination details. Breast development should include the timing of thelarche, breast growth in pregnancy, and when any stretch mark may have appeared. Medical and reproductive histories should include details about any endocrine condition (e.g., PCOS), menstrual cycle dysfunction, overweight or obesity, or fertility issues; even simply reporting the nonexistence of such conditions would be valuable. Indicating if the woman has any close female relative report of insufficient milk supply would be helpful to suggest a possible hereditary component to the condition. A detailed lactation history (ideally presented as a timeline) should include timing of secretory activation, exclusive and partial breastfeeding duration and 24-hour milk production, volume of formula use, infant growth details, and management of insufficient milk supply (including dosage of any galactagogue use), and outcomes of such management. Finally, a report of the examination of the woman's breasts should include comment about any breast asymmetry, intramammary width measurement, presence of stretch marks, and breast type classification.
Conclusion
Firm conclusions from this review cannot be made due to the low quality of studies and small number of participants. Findings from this systematic review suggest the need for prospective, high-quality studies to assess for an association between breast hypoplasia and breastfeeding outcomes. It has also highlighted that research to evaluate the reliability of measuring and classifying markers of breast hypoplasia is needed. Priority research addressing these gaps will assist health professionals working with breastfeeding women to better identify and address these problems and hence improve the breastfeeding experiences of women with this condition.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.