
Abstract
Background:
An individual's personal social network influences behavior; one is more likely to adopt behaviors consistent with norms within the network to avoid social stigma. Personal social network types, which are associated with individual behaviors, have been identified for new mothers: exclusive (kin centric) and expansive (not kin centric).
Objective:
To analyze the impact of personal social network type on breastfeeding practices in U.S.-born Black and White mothers.
Methods:
Mothers of infants <6 months old completed surveys about their personal social networks and feeding practices. Multinomial logit models examined how social network types moderated effects of sociodemographic factors on feeding practices.
Results:
Of 402 mothers, 67% self-identified as Black and 33% as White. Forty-six percent were exclusively breastfeeding; 26% were mixed breast and formula feeding. The likelihood of exclusively breastfeeding was positively associated with percentage of network members who had breastfed; this association was stronger for mothers with exclusive networks than those with expansive networks (β = 2.74, p < 0.001 versus β = 1.78, p = 0.03). Black race was positively correlated with exclusive breastfeeding or mixed feeding for mothers with exclusive networks (β = 1.50, p = 0.046; β = 1.86, p = 0.02, respectively). Lower educational level was negatively correlated with exclusive breastfeeding; this correlation was stronger for mothers with exclusive networks (β = −1.91, p = 0.002 versus β = −1.70, p = 0.04). Lower educational level was also negatively correlated with mixed feeding for mothers with exclusive networks (β = −1.61, p = 0.02).
Conclusions:
Mothers' personal social network type likely moderates the relationship between sociodemographic variables and feeding practices. While the influence of having network members with breastfeeding experience is important, the magnitude of influence is stronger in exclusive networks.
Introduction
Despite the numerous health benefits for both mothers and infants associated with breastfeeding, 1 and despite recommendations from national and international organizations to exclusively breastfeed for ∼6 months,2,3 breastfeeding rates in the United States are far below Healthy People 2030 Objectives that 42.4% of infants be exclusively breastfed through 6 months, and 54.1% of infants continue to receive any breast milk at 1 year. 4 In 2017, 84.1% of U.S. mothers reported ever breastfeeding, 25.6% were exclusively breastfeeding through 6 months, and 35.3% were continuing to receive any breast milk at 12 months. 5 The rates are even lower for U.S. Black mothers. 6
There are many sources of information that mothers use to make decisions about their infant care practices, including feeding practices. 7 Among these sources are the mother's family members, friends, colleagues, and acquaintances—that is, the mother's personal social network. In fact, mothers may consider the information received from their social network members to be more trustworthy than the information received from medical professionals. 8 In addition, one's personal social network influences one's perceptions of what are normal and acceptable behaviors—that is, social norms. One is more likely to act in a manner that is consistent with these social norms to avoid judgment, criticism, and ostracization by others. 9
Indeed, a mother's perception that breastfeeding is normative behavior may be highly influential in her decision to initiate and continue breastfeeding,10,11 and positive social norms regarding breastfeeding may explain why more highly educated women 12 and foreign-born Black women 13 are more likely to breastfeed than women with lower educational status and U.S.-born Black or White women, respectively. Thus, personal social networks and the norms within these networks may help explain the Black–White racial disparities seen in the United States with regard to infant feeding practices.
In social network analysis, every personal social network includes a focal person referred to as the “ego”—in this case, a new mother, defined here as the mother of a young infant, regardless of parity—and all contacts with whom the ego has close interpersonal ties (referred to as her “alters” or “network members”). Research regarding personal social networks has tried to understand how alters influence the ego's behavior, and which features of the network impact the strength of this influence. 14 Network features that have been found to be important include network size (number of alters), the proportion of family members (kin) within the network, and strength and density of the ties among the alters and between the ego and alters (e.g., how long each of the alters have known each other and the ego, and how often they are in contact). 14 When one's network is large, the influence of a single alter is reduced, whereas the influence of the alters is increased if the ties within the network are strong and dense, 15 likely because there is more pressure to conform to social norms within the network.16,17
We previously identified new mothers' personal social networks by asking mothers to name up to 10 persons with whom they regularly interact and discuss important issues and, using latent class analysis, we defined 2 mutually exclusive types of personal social networks for new mothers: (1) “exclusive” networks (primarily kin centric, with most alters ≥15 years older than the ego) and (2) “expansive” networks (not primarily kin centric, with alters of similar age to the ego). 18 When we analyzed the sociodemographic characteristics of new mothers with these two personal social network types, we found that mothers with exclusive networks are more likely to be Black, unmarried, young, and with lower socioeconomic and educational levels, whereas mothers with expansive networks tend to be older, more educated, and White.18,19 In general, those with socially disadvantaged backgrounds tend to have less access to wide-ranging social capital and networks, and are more likely to rely on local kin disproportionately for social resources. There are numerous reasons for this, including disadvantaged groups' disproportionate isolation in areas of concentrated poverty, and their resulting separation from larger social networks and institutions due to residential segregation, discrimination, and related factors.20–22
We also found, using social network analysis, that mothers with expansive networks are more likely to regularly use recommended safe infant sleep practices. 18 However, it is yet unclear whether these personal social network types influence infant feeding practices. We now use social network analysis to understand the influence of personal social network type on breastfeeding practices. Given the literature that adults with more diverse (i.e., comprising both kin and friends) social networks have more positive health behaviors,19,23–26 we hypothesize that mothers with expansive networks are more likely to breastfeed.
Methods
We recruited mothers of infants <6 months old in the Washington, DC metropolitan area using a combination of hospital-based and chain-referral recruitment. Because the purpose of the original study was to understand if personal social network features and social norms could provide insight into disparities in infant care between Black and White mothers,27–29 women were eligible if they self-identified as Black or White, had U.S.-born parents, and were English speaking. Other eligibility criteria included maternal age of ≥18 years, and having a full-term infant with no significant health problems or prolonged hospitalization. To reflect the proportions of Black and White women in Washington, DC, a recruitment aim was for 55–70% of the study population to self-identify as Black.
Hospital-based recruitment occurred on the postpartum unit of an urban hospital in Washington, DC. Each recruited mother was given up to five “coupons” to distribute for chain-based recruitment. As previously described, 30 these coupons contained basic information (e.g., study purpose, basic inclusion criteria) about the study, and mothers could give these coupons to any other new mother whom they knew. Women who received coupons (“referrals”) could contact study staff to determine if they were eligible to participate.
Once enrolled, mothers completed a phone-based survey when their infants were ∼2 weeks of age. The survey used validated questions to assess characteristics of their personal social networks, 31 perceived beliefs of their alters about infant feeding practices, and their own feeding practices. Participants received a gift card after survey completion and for each referral who was successfully recruited into the study.
The primary outcome variable was type of infant feeding (exclusive breast, exclusive formula, or mixed breast and formula). Strength of perceived breastfeeding norms within each mother's personal social network was determined by the proportion of alters who had at least one child who had been breastfed. The effects of sociodemographic factors (e.g., race, mother's age, education, marital status, parity, and medical insurance) on breastfeeding practice, as well as how such effects were moderated by the type of personal social network, were examined using a multinomial logit model.
To examine the effects of sociodemographic factors on both the social network type and feeding practices, the newly developed three-step approach32,33 was applied to account for measurement errors in the estimates for social network type. In the first step, an unconditional latent class analysis model was estimated using only the latent class indicator variables (network variables in the study). Step 2 calculated the measurement errors or class classification uncertainty, based on the results of Step 1. Finally, in Step 3, the desired model was estimated by incorporating the measurement errors calculated in Step 2. The three-step model estimations were conducted simultaneously in Mplus 8.2. 34
Sample size was calculated using Kim's method, 35 and was based on model fit index of the root mean square error of approximation (RMSEA). To achieve power of 0.80, α = 0.05, and RMSEA = 0.05 (close fit), the estimated sample size ranged from n = 243 to 163 as the degrees of freedom changed from 50 to 100.
This study was approved by the institutional review boards of Children's National Medical Center and the University of Virginia.
Results
We enrolled 402 mothers, of whom 67% self-identified as Black and 33% self-identified as White; 305 were recruited at the birth hospital, and 97 through the chain recruitment. Mean maternal age was 29.3 years, and 49% were college graduates. Nearly half (46.5%) of mothers reported exclusively breastfeeding, 27.4% reported exclusively formula feeding, and 26.1% reported mixed breast and formula feeding. Overall, mothers with expansive personal social networks were more likely to exclusively breastfeed than those with exclusive networks (60.4% versus 38.3%, p < 0.0001) (Table 1). Consistent with national data, 6 we found that older mothers were also more likely to breastfeed than younger mothers. The median age of mothers who were exclusively breastfeeding was 31.2 years, compared with 28.3 years for mixed feeding and 27.2 years for exclusive formula feeding (p < 0.0001).
Demographic Characteristics by Social Network Type (n = 402)
ANOVA, analysis of variance; SD, standard deviation.
p-Values were obtained from ANOVA or Pearson's chi-square test.
Table 2 describes the results of the multinomial logit model. While mothers in general were more likely to exclusively breastfeed if they had expansive networks, positive breastfeeding norms were particularly important for women with exclusive networks. Mothers were more likely to exclusively breastfeed rather than exclusively formula feed if they reported a more positive breastfeeding norm (i.e., a higher proportion of their alters had breastfed), and this relationship was stronger for mothers with exclusive networks (β = 2.74, p < 0.001) than those with expansive networks (β = 1.78, p = 0.03). Figure 1 demonstrates the link between network norms and mothers' feeding practices by comparing the personal social networks of mothers who reported either exclusive breastfeeding (left panel) or exclusive formula feeding (right panel).
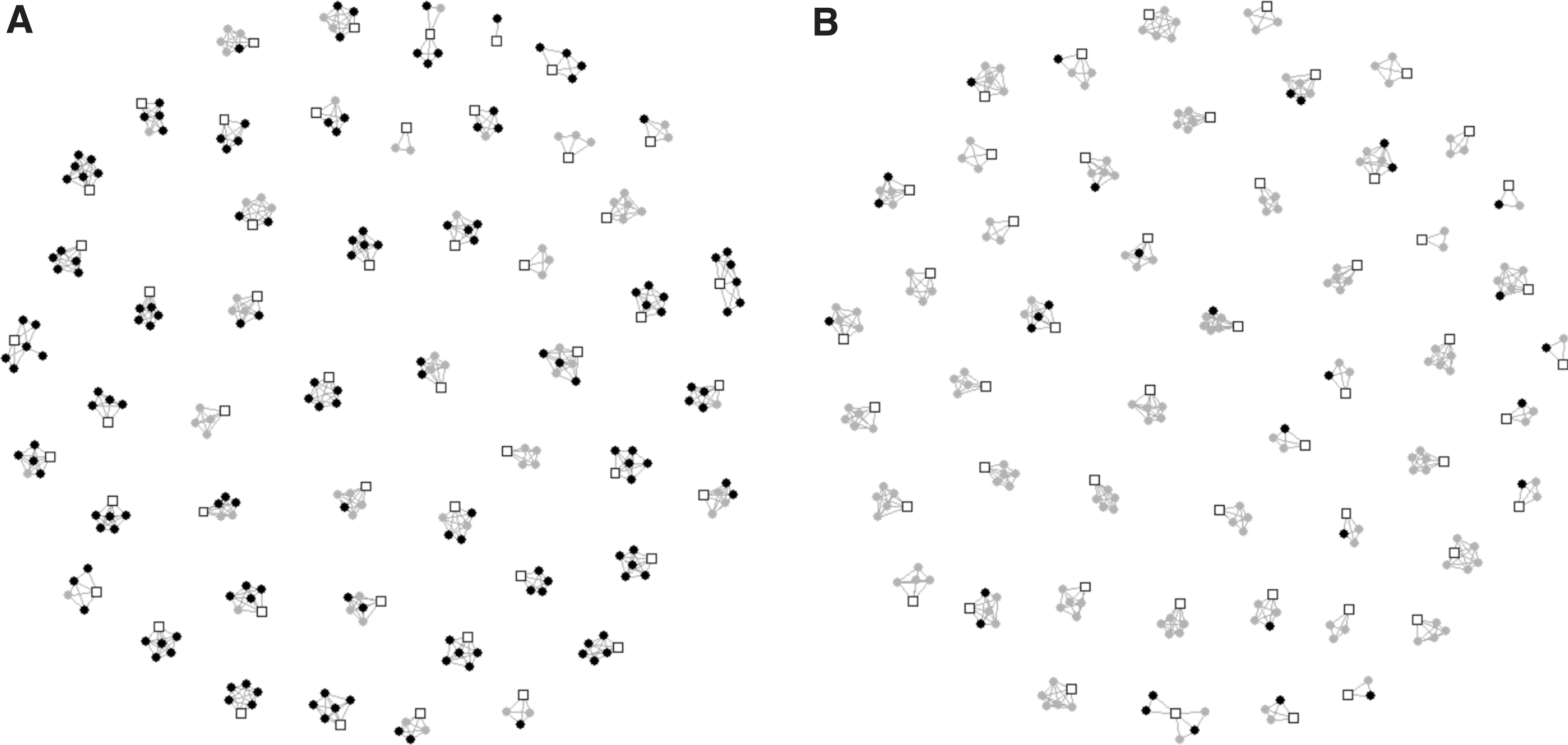
Presence of social network members (alters) who have breastfed, among
The Effect of Sociodemographic Factors on Breastfeeding by Network Type: Selected Results of Multinomial Model Using Three-Step Approach
Bold text indicates statistically significant values.
The influence of breastfeeding norms was similar for mothers who were mixed feeding, regardless of personal social network type (β = 2.34 versus β = 2.93, p = 0.001 for both). Black race was positively associated with both exclusive breastfeeding (β = 1.50, p = 0.046) and mixed feeding (β = 1.86, p = 0.02) for mothers with exclusive networks, but not for those with expansive networks. Mothers who did not graduate from a 4-year college were less likely to exclusively breastfeed, but this association was stronger for mothers with exclusive (β = −1.91, p = 0.002) than expansive networks (β = −1.70, p = 0.04). Similarly, not graduating from a 4-year college was also negatively associated with mixed feeding for mothers with exclusive (β = −1.61, p = 0.02) but not expansive networks.
Discussion
We found, using network members' prior feeding practices as a measure of social norms, that stronger breastfeeding norms within mothers' personal social network were associated with breastfeeding, particularly for women with exclusive networks. Thus, personal social network type is likely an important moderator of the association between sociodemographic factors and infant feeding practices. This finding has important implications with regard to understanding reasons for the racial disparities seen in breastfeeding practices and the need for more targeted education toward influential network members. In addition to the finding that exclusive networks are more prominent among Black mothers, 18 we have found that positive breastfeeding norms are a significant mediator of the relationship between Black mothers' birth nationality and their infant feeding practice, and that non-U.S.-born Black women have seven times and three times higher odds of breastfeeding than U.S.-born Black or White women, respectively. 13 Thus, while there are multiple additional social determinants of health that impact feeding practices, the potential impact of increasing the strength of breastfeeding norms within exclusive networks should not be underestimated, particularly in the Black community, where breastfeeding rates continue to be overall lower than they are for other U.S. racial and ethnic groups. 6
It is not surprising that, overall, new mothers who have expansive (e.g., friend- and colleague-based) personal social networks were more likely to exclusively breastfeed than women with exclusive (kin-centric) networks. Social network theory suggests that people with expansive networks may be more likely to adhere to recommended health behaviors because they are more exposed to a variety of ideas and new information 36 through a more diverse group of alters. 37 Analyses of personal social network types have largely been conducted for older adults, and have found that friend-based or “diverse” networks (those with both friends and family as alters) are associated with healthier practices 23 than networks that are either kin-centric or “restricted” (less contact with alters) networks.19,24–26 In fact, our previously published analysis found that new mothers who have expansive networks are also more likely to follow recommended safe infant sleep practices. 18
Some additional explanations possibly underlie our finding that Black mothers are more likely to have exclusive personal social networks. Theories of racial disparities in social capital contend that racial or ethnic minority groups may be subject to contextual determinants and sociocultural environments unique to their groups, which in turn shape their distinct trajectories of network formation and activation. 38 On the one hand, the structural conditions that perpetuate racial inequality could play a critical role in this respect. For example, mechanisms such as residential segregation and labor market discrimination may result in lower capacity for Black mothers to form diverse networks that encompass both kin and friends. 39 On the other hand, cultural beliefs and preferences may also contribute to the observed patterns here. For example, research consistently finds a higher proportion of extended and fictive kin (i.e., relationships based on social ties rather than blood, marriage, or adoption ties) among Black close ties, which may relate to the heavier emphasis and reliance on kin networks for everyday interactions and support among Black communities. 40
Although new mothers with expansive personal social networks are, in general, more likely to breastfeed, the importance of social norms is amplified for new mothers with exclusive networks. The finding that new mothers with exclusive networks are more likely than those with expansive networks to follow their social network's breastfeeding norm is consistent with social network theory. Smaller, denser, kin-centric networks are more likely to directly affect one's behavior than are more dispersed, larger networks.15,41,42 The effect that these smaller, more interconnected networks have on creating norms for behavior is equally strong for norms that are consistent with and divergent from established health recommendations. Smaller, more exclusive networks, which are populated by people who know and talk to each other frequently, have a greater capacity to enforce local social norms through informal social sanctioning and control. Breastfeeding norms within the network create powerful social pressures, particularly when they come from tightly interconnected network members, who can work in concert to compel a mother to maintain conformity with these norms.16,17 They can also provide support to help breastfeeding mothers reach their goals. 10 In addition, social pressures from family members, particularly older ones, may be particularly powerful if these family members provide material or emotional support to the mother. For women in expansive networks who are less dependent on family, adopting behaviors that contrast with network norms may not have as profound of a potential impact on access to support as it does for women in exclusive networks.
Our findings are particularly important as they may help differentiate between the effect of the primary demographic characteristics of each network type and the effect of the network type itself. For example, with regard to exclusive breastfeeding, previous studies have found that White women and women with higher levels of education are more likely than Black women and women with less education to breastfeed. 6 In our sample, both White women and those with higher education levels were more likely to have expansive personal networks. Given that normative factors (e.g., proportion of alters who had breastfed) within expansive networks had stronger associations with breastfeeding than demographic factors, our findings suggest that social network type is an important consideration. This information can potentially be used as an alternative to race and education to more accurately identify new mothers at risk for not breastfeeding.
Our finding that Black race is positively correlated with breastfeeding of any type (exclusive or mixed feeding) for those with exclusive networks is particularly interesting, given the historical Black–White disparity in breastfeeding prevalence among U.S.-born women. 6 (All of the mothers in our sample were U.S. born.) While further research with larger sample sizes will be necessary to confirm this finding, we are encouraged by the prospect that, when a mother has an exclusive personal social network, the impact of the breastfeeding norm has a powerful impact on her own breastfeeding behavior. This finding is also consistent with qualitative findings, suggesting that having at least one alter who serves as a breastfeeding champion for the mother can have a positive impact on her breastfeeding. 10
Our study presents several limitations. As with all survey data, our results are based on participant response and perception, not on observed behavior. It is therefore possible that there was response bias based on what participants believed to be the desired answer. In addition, we did not stratify the data by infant age, and we acknowledge that the proportion of breastfeeding infants declines with infant age. 5 However, we note that our findings are consistent with those derived from other large, epidemiologic datasets.5,43 Our norms were also defined by participant response, not by directly asking network members about their beliefs and practices; therefore, they may reflect participants' perceptions rather than actual norms. However, since it is the participant's perception of acceptable or prevalent behavior (rather than the real prevalence of the behavior) that defines the social norm for that individual, direct queries of alters would not be helpful in this regard.
It is important to note that numerous health-related behaviors are heavily influenced by respondents' perceptions and social desirability concerns, which may bias the estimates that we reported. We were also unable to distinguish whether the high degree of clustering of alters with similar breastfeeding behavior within a network (as evidenced by Fig. 1) was due to local social norms and social influence versus perceptual bias. Similarly, it is possible that the presumably greater correlation between mothers' and alters' breastfeeding behaviors within exclusive personal networks reflects not-yet-identified factors that inevitably make such clustering more likely. This analysis also did not account for influences outside of the personal social network, such as advice and encouragement from medical and lactation professionals, unless these individuals were specifically named by the individual as alters. In addition, as we recruited in only one geographic region, the results may not be generalizable, and additional studies in other geographic regions and among other racial/ethnic groups will be needed to confirm these results.
Conclusions
New mothers' personal social network type likely moderates the relationship between sociodemographic variables and infant feeding practices. While the influence of network members with breastfeeding experience is important, the magnitude of influence is stronger for those with exclusive, kin-centric personal social networks.
Footnotes
Authors' Contributions
R.F.C. made substantial contributions to data analysis and interpretation, and codrafted the initial article. B.C., J.W., and L.Y.F. made substantial contributions to the conception and design, data analysis and interpretation, and critically reviewed and revised the article for important intellectual content. A.M. made substantial contributions to data acquisition and critically reviewed the article for important intellectual content. Y.I.C. and X.Y. made substantial contributions to data analysis and interpretation, and critically reviewed and revised the article for important intellectual content. R.Y.M. made substantial contributions to conception and design, data analysis and interpretation, codrafted the initial article, and revised the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Disclosure Statement
No competing financial interests exist.
Funding Statement
This project was supported by the National Institute for Minority Health and Health Disparities 1R01MD007702. The study sponsor had no role in study design; collection, analysis, and interpretation of data; writing the report; and the decision to submit the report for publication. The authors have no other funding sources.