
Abstract
Background:
There are no national data on the prevalence of breastfeeding during pregnancy (BDP) in the world. Also, there is no consensus for the BDP.
Aim:
The purpose was to determine the prevalence of breastfeeding status in pregnant mothers having children younger than 24 months of age and to evaluate the associated sociodemographic factors and characteristics of the last-born child and current pregnancy through two consecutive national health survey.
Methods:
Data from the 2012 and 2017 Jordan Family Health and Population Survey were merged. Individual, household, and community-level factors associated with BDP were analyzed by using complex sample multivariate logistic regression.
Results:
Two surveys enrolled 6,858 women having at least one child younger than 24 months and 8.8% (weighted count: 603) of them got pregnant also. Of the pregnant women, 8.9% continued breastfeeding their last-born children. Being younger than 12 months positively affected breastfeeding compared to last-born child aged 12–23 months. Multivariate analysis revealed that BDP was associated positively with wealth index (richest vs. poorest) and postnatal care for the last-born child within 2 months (presence vs. absence), whereas negatively with bottle use (presence vs. absence), traditional contraceptive methods (abstinence/withdrawn vs. modern, lactational amenorrhea vs. modern), short interpregnancy interval (months), and current pregnancy duration (months) in Jordan.
Conclusions:
The prevalence for BDP differs according to some maternal, last-born infant, and current pregnancy characteristics. Prospective cohort studies are necessary to evaluate the impact of BDP on “mother, last-child, and future-child,” and to detect the duration and prevalence of BDP in different countries.
Introduction
Breastfeeding confers a wide range of health benefits to children, including lower risks of newborn and infant mortality, the incidence of leukemia, acute otitis media, asthma, pneumonia rates, and strengthens the relationship between mother and baby pairs. In addition, breastfeeding has social, economic, and environmental benefits for society.1,2 The majority of mothers want to breastfeed as long as possible to get the benefits of breastfeeding for their children, but the overlap of an unplanned pregnancy with breastfeeding leaves mothers in a dilemma about breastfeeding. 3
Some mothers do not use active and regular contraceptive methods, considering temporary contraception due to the prolongation of amenorrhea period of breastfeeding, and might get pregnant. 4 Despite the lack of no recommendation to encourage breastfeeding during pregnancy (BDP), the general advice from obstetricians is not to breastfeeding. 5 The lack of consensus on advice on the safety of continuing BDP affects the breastfeeding prevalences of infants with new occurring pregnancies. 6 Undoubtedly, among the factors that contribute to BDP, fear of miscarriages is the most important. In limited studies on this subject, a significant relationship between miscarriages and BDP has not been shown.3,7,8 BDP is shown to reduce maternal fat capacity and is associated with lower pregnancy weight gain and higher risk of maternal anemia.9,10 BDP is affected by many conditions, including regional factors, socioeconomic, living conditions, and the trimester of pregnancy. 11 Estimates from low- and middle-income countries show that the prevalence of BDP is between 4% and 35% in the first trimester, while this rate declines to 0–8% in the third trimester.12,13 Up to the present, the prevalence and associated factors for BDP were examined neither in national data nor with a further analysis of demographic health survey data in the world. In addition, only 30% of children younger than the age of 2 years are receiving age-appropriate breastfeeding in Jordan.
When the targets of achieving Sustainable Development Goals 2 and 3 to improve nutrition and secure healthy lives are considered, all infants, including those mothers who got pregnant with shorter succeeding interpregnancy interval, should get age-appropriate breastfeeding as a primer for a healthier life. 14 However, suboptimal breastfeeding practices are prevalent in Jordan. When trends for breastfeeding prevalence in three consecutive Jordan Population and Family Health Survey (JPFHS) were evaluated, the median duration of any breastfeeding is seen to be 9.7 months among children born in the 3 years preceding the survey in 2017, 11.7 months in 2012, and 12.5 months in 2007.15,16 There is an worsening in breastfeeding parameters in the last 15 years. On the contrary, there are no data about the status of breastfeeding in infants having pregnant mothers.
The determination of the prevalence of BDP and the associated factors will help to design health policies that will ensure that children whose breastfeeding is abandoned due to early pregnancy can be BDP. This study aimed to examine the prevalence of breastfeeding status in pregnant mothers having children younger than 24 months of age and to evaluate the associated sociodemographic factors and characteristics of the last-born child and current pregnancy in two consecutive JPFHS.
Methods
Study settings
In this study, we used merged data of the 2012 and 2017 JPFHS. The survey is designed to obtain results representative of the country as a whole, of urban and rural areas separately, and of three regions. More details on sampling techniques and data collection methods can be found in the JPFHS report.15,16
Overall, two surveys enrolled 6,858 women having at least one child younger than the age of 24 months. Our analysis was limited to pregnant mothers who had at least one child younger than 2 years of age at the survey and the total unweighted sample size was 670. Taking the sample weights into account, this number was calculated to be 603 (8.8%). The prevalence of pregnancy was 4.1% in mothers having a child younger than 12 months and 14.0% in those having a child between 12 and 23 months. While 55.7% of children younger than 24 months of age were breastfed, only 8.8% of babies whose mothers got pregnant; this condition was 75.4% and 21.7% in those with last-born child younger than 12 months, respectively, while it was 31.0% and 4.5% between 12 and 23 months old.
Outcome variables
The outcome variable in the study was BDP, and based on reports of the pregnant women who answered “yes” to the “Are you still breastfeeding?”, they were interviewed in JPFHS surveys.
Independent variables
We analyzed the data in our study under three main groups according to the characteristics of the mother (place of residence, region, the wealth index, maternal age, educational level, employment status, and tobacco use), characteristics of last-born child (age, gender, birth order, mode of delivery, birth weight, postnatal care within the first 2 months, and bottle use), and current pregnancy [maternal method use for family planning, preceding interpregnancy interval, wanted pregnancy when became pregnant, and duration of current pregnancy (gestational week)]. The place of residence is as stated in both JPFHS (urban–rural). In terms of regions, central, north, and south were taken into account. The wealth index was “poorest,” “poorer,” “middle,” “richer,” and “richest” as reported in the JPFHS. Mother's age at birth was recorded as “<20,” “20–34,” and “≥35 years”. The education status of mothers was categorized as “uneducated-primary school,” “secondary school,” and “higher”. The employment status of mothers was divided into “with no job” and “working”. Tobacco use was categorized as “yes” and “no”. The birth order of the last-born child was recorded as “1,” “2–3,” and “4th” and more. In addition, we included independent variables such as bottle feeding, mode of delivery that we think may influence breastfeeding success.17,18 The mode of delivery was considered “normal” or “cesarean.” The birth weights of babies were divided into two groups: “<2500 g” and “ ≥2500 g”. The presence of postnatal care within the first 2 months was grouped as “yes” and “no”. Maternal last family planning method was grouped as absence, abstinence/withdrawal, lactational amenorrhea (LAM), and modern methods. Wanted pregnancy when became pregnant was classified as “then,” “later,” and “no more”. The gestational weeks of the current pregnancy were examined in three parts as 1st, 2nd, and 3rd trimesters. The interpregnancy interval was calculated by period spanning from the birth of the last-born child to the start of the current pregnancy and divided into three groups; 2–5, 6–11, and ≥12 months.
Statistical analysis
Data were analyzed using IBM SPSS version 22.0 statistical software package program. Initially, weighted case numbers and frequencies were taken as descriptive statistics of the general characteristics. Median and interquartile range values of interpregnancy internals were calculated. Then, distributions of BDP according to the characteristics of mother, last-born child, and future child were given as unweighted and weighted frequencies. The differences in independent variables for BDP were analyzed with the Chi-square test and complex sample logistic regression analysis. Then, independent variables with p < 0.250 in the univariate logistic regression analysis were included in the complex sample multivariable logistic regression analysis method. Odds ratio (OR) or adjusted odds ratio and 95% confidence interval (CI) were taken.
Ethics
For ethical clearance, JPFHS protocols had been present. For the present research, the Demographic and Health Surveys (DHS) Program permitted to access data (Oct 12, 2020).
Results
Descriptive findings
The number of pregnant women having infants younger than 24 months was 603 (n = 285 in 2012, n = 318 in 2017). Demographics are summarized in Tables 1 and 2.
Maternal Sociodemographic Characteristics
Column percentage.
Weighted row percentages.
Complex sample logistic regression.
CI, confidence interval; OR, odds ratio.
Characteristics of the Last Child
Column percentage.
Weighted row percentages.
Complex sample logistic regression.
The last-born children included in the study were categorized as <12 months and 12–23 months according to age: 75.1% of the babies were between 12 and 24 months, and 24.9% of them were <12 months (Table 2).
When the last contraceptive method of enrolled mothers was evaluated, we found that more than 1/3 of mothers did not use any method, 30.2% of them used abstinence, withdrawal method, 26.7% of them using modern methods, and 4.6% of them used LAM method. The status of wanted pregnancy did not differ among the mothers who want the baby when pregnant, later, and no more (Table 3). The median interpregnancy interval (interquartile range) was 12 (7–15) months in those using modern methods, 12 (9–16) months in withdrawal/abstinence, 10 (5–11) months in those using the LAM method, and 8 (6–14) months in those who do not use any family planning method.
Characteristics of Used Contraceptive Methods and the Last Pregnancy
Column percentage.
Weighted row percentages.
Complex sample logistic regression.
The status of being in the first, second, and third trimesters of gestation was 31.5%, 35.9%, and 32.6%, respectively (Table 3).
Current breastfeeding and associated factors in pregnant women
Overall, 9.7% of mothers never breastfed their last-born infants. The prevalence of BDP was 8.9% (95% CI: 6.0–13.0).
When factors affecting BDP were examined by univariate complex sample logistic regression analysis, we found no change in BDP among the 2012 and 2017 JPFHS data (OR: 1.37, 95% CI: 0.58–3.24). There was no difference in BDP over the three geographical regions of Jordan. Maternal age, mode of delivery, current employment status of the mother, smoking status, and place of residence did not have a significant effect on BDP (Table 1, Table 2). Logistic regression revealed that wealth index and maternal education had a significant interaction with BDP.
Among last-born child variables, birth order, child's age, the presence of postnatal care had a significant influence on BDP (Table 2). We found that postnatal care was 71.3%, and there was a 10.3% of BDP in those who were followed within 2 months postnatal. Furthermore, the last-born child with the 4th and above birth order had upper odds for being breastfed compared to those who had the 2nd–3rd birth order (OR: 2.83, 95% CI: 1.06–7.56). In the last child's age group, it was found that being in the group <12 months positively affected the BDP ratio (OR: 5.89, 95% CI: 2.46–14.13) compared to the group aged 12–23 months.
BDP prevalence was lower in ≥12 months of interpregnancy interval by 78% (95% CI: 0.07–0.67) compared to the 2–5 months (p = 0.006). It was found that the rate of breastfeeding of the last child in the third trimester of new pregnancy decreased by 96% compared to the first trimester period (OR: 0.04, 95% CI: 0.01–0.16). As a result of our study, it was found that the breastfeeding rate, which was 31.9% in the first trimester, decreased to 21.4% in the second trimester in the group with the last child's age <12 months; in the group whose child's age is 12–23 months, the breastfeeding rate which was 8.9% in the first trimester decreased to 4.8% in the second trimester (Fig. 1).
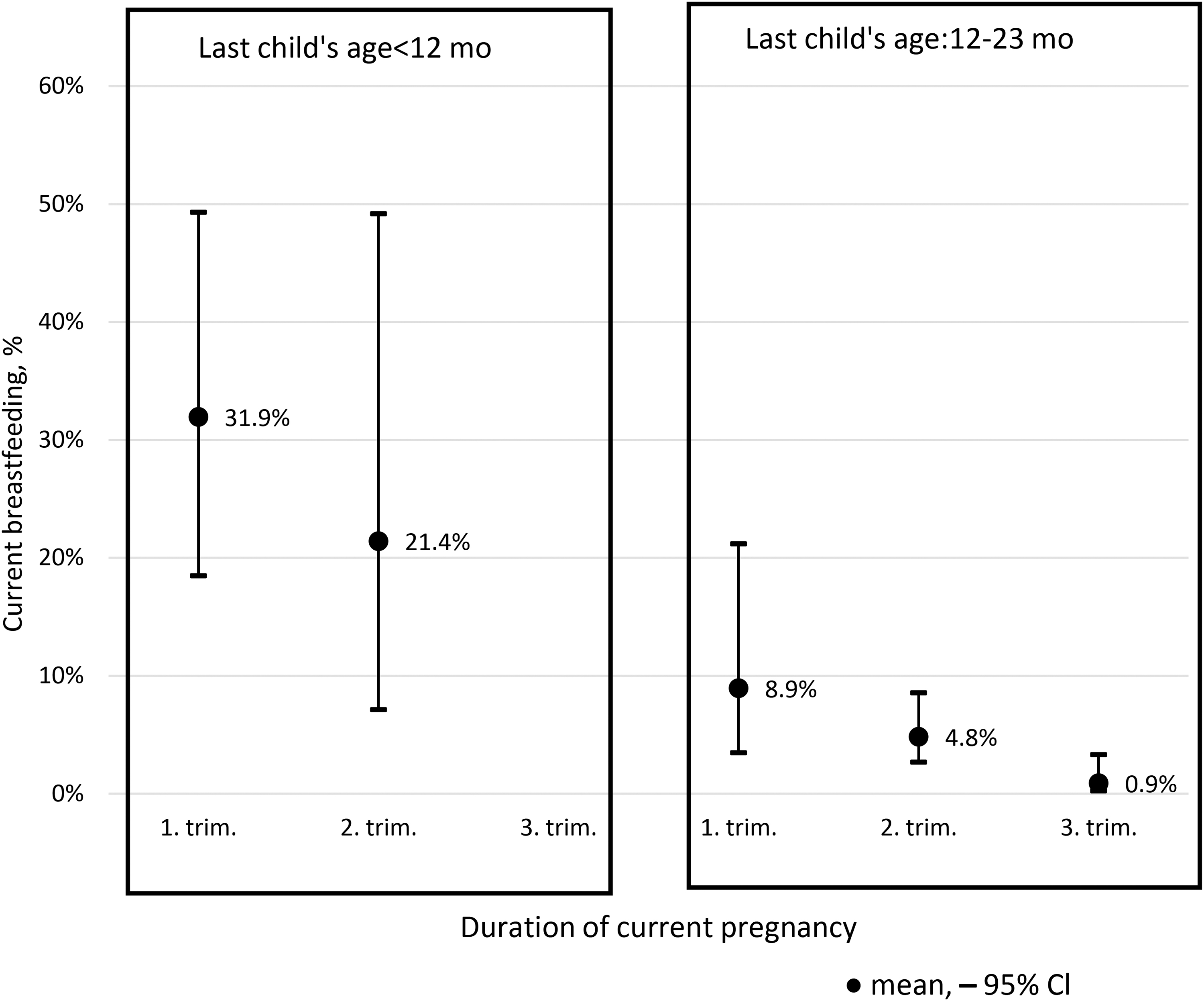
Continued breastfeeding according to last child's age and gestational duration of current pregnancy. CI, confidence interval.
Interestingly, while 13.1% of mothers using modern contraception breastfed their babies, this prevalence decreased to 3.3% (OR: 0.22, 95% CI: 0.05–0.98) in mothers using LAM and to 1.2% (OR: 0.08, 95% CI: 0.03–0.23) in mothers used abstinence and withdrawal (Table 3).
In the survey year, the characteristics of mother (wealth index, education), last-born child (birth order, delivery type, age, gender, postnatal care, and bottle use), and current pregnancy (last contraceptive method, interpregnancy interval, and duration of pregnancy) were examined using the complex sample multivariate logistic regression method we found following the significant results on BDP (Table 4): The richest group of wealth index increased BDP by 6.45 (95% CI: 1.10–37.84) fold compared to the poorest group; The postnatal care of the last child in the first 2 months increased BDP by 4.46 (95% CI: 1.41–14.13) fold compared to absence; bottle use reduced BDP by 73% (95% CI: 0.11–0.65); compared to mothers who used modern contraceptive methods, those using LAM and abstinence/withdrawal methods decreased BDP by 88% (95% CI: 0.02–0.93) and 94% (95% CI: 0.01–0.39), respectively; 14% (95% CI: 0.78–0.94) of breastfeeding prevalence decreased with each 1-month increase in preceding interpregnancy intervals, and each 1-month increase in duration of current pregnancy decreased by 39% (95% CI: 0.50–0.75).
Association Between Breastfeeding During Pregnancy and the Characteristics of Maternal-Child-New Pregnancy
Complex sample multivariable logistic regression.
AOR, adjusted odds ratio.
Discussion
To our knowledge, this is the first study conducted through the further analysis of two consecutive JPFHS. The results indicate that the household wealth index, postnatal care and bottle use of last-born child, last contraceptive methods of mother, the duration of current pregnancy, and interpregnancy interval are associated with continued BDP.
Pregnancy can be seen in mothers who do not use modern contraceptive methods during breastfeeding periods. New pregnancy creates a dilemma for the mother against breastfeeding and wants the breastfed child not to be deprived of the immunological and protective properties of the human milk that support growth and development. In Southeast Asian, African, and South American countries, especially in Peru and Guatemala, mothers continue to BDP.11,19 In studies conducted in various parts of the world, the prevalence of BDP has been shown to vary between 4% and 50%.11,12 We determined that the overall BDP rate was 8.9% in our study.
According to a limited number of studies, it has been shown that the prevalence of breastfeeding cessation during a later pregnancy is high.12,20 The rates of BDP in the northern African countries Egypt, Morocco, and Tunisia, decreased from 30.9% to 4%, from 9.9% to 2.3%, and from 17.3% to 3% toward the third trimester, respectively. 12 A study conducted in Bhutan showed that around 18% of lactating mothers breastfeed their children until the last stages of pregnancy. 20 Breastfeeding rate in women whose last child is <12 months decreased from the 1st trimester to the 2nd trimester from 31.9% to 21.4%; and in children aged 12–23 months, this rate decreased from 8.9% in the first trimester to 0.9% in the third trimester in the current study. When the interaction between trimesters and BDP was examined with the complex sample logistic regression analysis, we found that the rate of breastfeeding in the third trimester was lower by 96% compared to the first trimester (OR: 0.04, 95% CI: 0.01–0.16).
It is more common for breastfeeding to overlap with pregnancy when birth intervals are close to each other, and it is a practice preferred by mothers to continue breastfeeding the last child.12,21,22 BDP was found to be negatively correlated with the age of last-born infant and interpregnancy interval in the present study; breastfeeding prevalence was detected to be 14% (CI: 0.78–0.94) lower with each 1-month increase in succeeding interpregnancy intervals. The age range of the last breastfed sibling in the previous studies was reported to vary from 4 months to 3 years.5,13,23 However, in these studies, there was no conclusion about the effect of the age of the last breastfed sibling on the duration of BDP.
In data of JPFHS-2017, 47.5% of infants aged 9–11 months and 26.1% of 12–23 months were reported to be breastfed. However, breastfeeding prevalence is much lower in infants older than 12 months when their mother got pregnant (Fig. 1) compared to all infants in JPFHS-2017 and 2012 data.15,16 Similarly, Molitoris 13 showed BDP decreases with the age of the last born child in low- and in middle-income countries.
Last-born infants fed with bottle had lower prevalence for being breastfed in the present study. The use of bottle has a negative effect on breastfeeding, due to differences in sucking mechanism. 18 Besides, pacifier is shown to shorten duration of breastfeeding. 24 However, the bottle-fed child may not be breastfed even when his/her mother becomes pregnant, it is difficult to say which one is first, and we have no data to clarify this subject. Cohort studies with larger populations are needed on this subject.
Obtaining professional support in breastfeeding, living in a supportive environment for breastfeeding, having adequate information and experience in breastfeeding, play a key role in mothers' long-term breastfeeding of their babies.25–27 The higher rate of breastfeeding in babies who were followed up in the postnatal period of 2 months, in mothers using modern contraceptive methods, and in mothers belonging to the richest wealth index compared to counterparts may be related to the fact that the mothers received breastfeeding counseling from health care professionals during the period mother-baby received health care services. Policymakers, especially the World Health Organization, emphasize that breastfeeding counseling and training programs should be given to mothers to increase breastfeeding rates and improve misconceptions.28,29
The most important factor in the baby's healthy growth and development is undoubtedly the care and endeavor of the mother.30,31 Breastfeeding plays a key role in this process.5,32 The mother's planning for her baby and the intended pregnancy will increase the care and maintenance of the baby in the postnatal period. The family planning method in Jordan is affected by sociocultural structure, generational differences, and women's religious and traditional beliefs, and it has been shown in studies that women have limited knowledge on contraceptive methods. The withdrawal method was the most preferred among traditional methods, while pills were used more among the modern methods in Jordan.33,34 Similar to the literature, the most preferred contraceptive methods were withdrawal and modern methods. One of the remarkable results in the current study was that the prevalence of BDP was found considerably lower in those who used LAM and withdrawal/abstinence method, which cause more unintended pregnancy, compared to the use of modern methods that are not planned by pregnancy or using no method in line with beliefs.
When the relationship between the duration of BDP and the time of wanted pregnancy was examined, no relationship was found. Similarly, no relationship was reported between the planned pregnancy and the BDP. 5
Yalçın et al. 17 in 2014 examined the factors that continued breastfeeding for beyond 12 months, it was shown that having at the ≥5th birth order increased the duration of breastfeeding by 2.56 times than 1st birth order (95% CI: 1.80–3.64). Similarly, the prevalence of BDP was 2.83 times higher in babies with birth orders of 4 or above than babies with 2nd and 3rd birth orders (OR: 2.83, 95% CI: 1.06–7.56) in univariate analysis. However, the significance was disappeared in multivariate analysis in the present study. Additional studies with a large sample size can give more knowledge about this subject.
Strengths and limitations
Our study has some limitations. First, due to the cross-sectional nature of the study design, a cause-effect relationship cannot be made between BDP and determining factors, and secondly, no comment can be made on the reason for stopping breastfeeding. Although it is the strength of the study to examine two DHS data, only 603 cases (weighted count) were available. This situation created limitations in subanalyses. More comprehensive and prospective cohort studies are needed in the future to establish and develop a consensus on BDP.
Conclusion
Overall, this is the first study in the literature on the BDP of children younger than the age of 24 months using DHS data. It was also determined that there is no association for BDP with the region, type of place of residence, working status of the mother, birth weight, the mode of delivery, and gender of last-born child. The prevalence of breastfeeding was higher in shorter interpregnancy interval, earlier gestational age, usage of modern contraceptive methods, presence of postnatal care within the first 2 months, and absence of bottle use for the last-born children. As there is no evidence that BDP is harmful to the supported mother, the future child or breastfed child who is under a close follow-up, families/mothers should be encouraged to BDP, and health care professionals should be made aware of this.
Footnotes
Authors' Contributions
S.S.Y. performed conception, design of the work, and analysis; S.Y. conducted acquisition, pulled data, and analysis. M.S.D. have reviewed published studies and drafted the work. All authors reviewed and edited the final version of the article.
Ethics Approval and Consent to Participate
The present research relied on the secondary data analysis of a deidentified data set. Ethical standards were upheld in the research process. DHS programs were given permissions and survey data.
Availability of Data and Materials
The data that support the findings of this study are available from DHS, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Disclosure Statement
Authors declare that they have no competing interests.
Funding Information
The current research received no specific grant from any funding agency, commercial, or not-for-profit sectors. No other entity besides the authors had a role in the design, analysis, or writing of the current article.