
Abstract
Objective:
The study aimed to identify and map the factors that shape the delivery of hospital-based lactation care for bereaved mothers to inform quality improvement initiatives targeting hospital-based lactation care.
Methods:
Focus groups and interviews were conducted at three large hospitals in Australia with 113 health professionals including obstetricians, neonatologists, midwives, neonatal nurses, lactation consultants, social workers or pastoral care workers, Human Milk Bank (HMB) staff, and perinatal bereavement nurses. Thematic and interactional data analysis identified the nature, scope, and pattern of bereavement lactation care.
Results:
A bereaved lactation care pathway was generated from health professionals' reports. Bereaved lactation care, if provided, was limited to brief encounters aimed at facilitating lactation suppression. The type of lactation care offered, and any exploration of the variable biopsychosocial significance of lactation after infant death, was conditional on (i) availability of health professionals with suitable awareness, knowledge, capacity, confidence, and comfort to discuss lactation; (ii) hospital culture and mode of suppression primarily practiced; (iii) mother's breast milk being visible to hospital staff; (iv) mother expressing interest in expanded lactation management options; (v) availability of, and eligibility to, donate to a HMB; and (vi) support beyond the hospital setting being facilitated.
Conclusion:
Mothers should be presented with the full array of lactation management options available after stillbirth or infant death. Inclusion of evidence-based, biopsychosocial and patient-centered approaches to lactation care is urgently required in health professionals' bereavement training and in the policies of hospitals and HMBs.
Introduction
After late miscarriage, stillbirth, or neonatal and infant death many bereaved mothers need to manage the initial onset or continuation of their lactation. Lactation after stillbirth and infant death elicits a wide range of responses and needs from bereaved mothers.1–3 Health professionals and Human Milk Banks (HMBs) play a critical role in the provision of lactation information and support in bereavement. Clinical guidelines stipulate that bereaved mothers should be advised on their lactation and the methods to manage milk supply, 4 with resources specific to bereavement also available for HMBs.5–7 While suppressing lactation may be the most common practice in bereavement, sustaining lactation, keeping milk as a memento, or donating breast milk can assist some mothers to cope with their grief,2,3,6,8 thus indicating the emotional and social significance of lactation and breast milk in bereavement.6,8–10
At the center of safe maternal health care delivery is the premise that women have the necessary information, time, consideration, and respect to make decisions about their physical and emotional needs. 11 However, lactation care offered to bereaved mothers within hospital settings is currently limited. A survey of parents of stillborn infants in Australia revealed less than half (42%) were informed about lactation and given the option of seeing a lactation consultant. 12 Moreover, in Australia milk donation remains an elusive option for bereaved mothers.13,14 These findings reflect the experiences of bereaved mothers from other countries, who also report receiving inadequate guidance to manage or make decisions about their lactation or breast milk.1–3,15
Engaging in shared decision making with bereaved families who have experienced a stillbirth or infant death is a difficult and confronting task for hospital-based health professionals. 16 Health professionals may have a lack of grief and bereavement care training 17 and limited knowledge and awareness of lactation options after stillbirth or infant death and lack the confidence to initiate or manage lactation care discussions with bereaved families.7,18 Furthermore, care discussions or lactation management options may be curtailed due to health professionals' concerns about adding distress to bereaved families.16,19 Lactation management options may also be withheld due to system constraints, such as limited access to HMB facilities 13 or a lack of clarity over who is responsible for providing lactation support and when support is best provided. 18 This is compounded by the onset of lactogensis II and/or changes in bereaved mother's lactation practices often occurring once they have left hospital when they are unlikely to be in receipt of midwifery care.7,18
To improve maternal health care quality, attention needs to be paid to complexities and uncertainty present at the clinical-organizational interface. 20 The aim of this study was to work with practicing health professionals to explore their experiences of providing hospital-based lactation care to bereaved mothers. The study aimed to identify the factors that shape clinical encounters with bereaved mothers and inform quality improvement initiatives targeting hospital-based lactation care.
Materials and Methods
Study design
Focus groups were used to investigate the perspectives, experiences, practices, and practice contexts of hospital-based health professionals who may provide lactation and/or grief care to bereaved mothers after infant death. Focus groups are an effective way for health professionals to share, question, debate perspectives and practice experiences, and to uncover issues yet to be considered by researchers.21,22
Focus groups were designed to be consistent with best practice in grief scholarship,23,24 and research into health care quality. 22 Researchers conducting the study were experienced in conducting qualitative studies on sensitive issues (including hospital-based care and grief) and carefully observed participants' comfort during data collection activities. All invited participants were able to access anonymous support from specialist infant bereavement counselors before or after focus group sessions.
Ethics approval for the study was provided by the Human Research Ethics Committee (HREC) and/or Research Governance Office of each participating hospital and by the researchers' University HREC. The Primary HREC for the study was ACT Health 2018.ETH.00190.
Setting and participants
Three large tertiary hospitals located in three eastern Australian states and territories were included in the study. Hospitals were purposively selected due to all having Level 4 or 6 Neonatal Intensive Care Units (NICU) and two of the three hospitals having an onsite HMB.
Health professional disciplines included in the study were identified by consultation with the study's Stakeholder Advisory Group (SAG). The central inclusion criteria being those professionals most likely to interface with bereaved families after stillbirth and infant death, and who may be called upon to offer lactation care. These included obstetricians, neonatologists, midwives, neonatal nurses, lactation consultants, social workers or pastoral care workers, HMB staff, and specialist perinatal bereavement nurses.
SAG members employed at each hospital site assisted in the recruitment of health professionals. Participation was voluntary and health professionals' made aware their employment would not be adversely affected if they chose not to participate. All participants provided written informed consent to participate in the study.
Data collection
Seventeen profession-specific focus groups (each with between 3 and 17 participants) with a total of 108 health professionals were conducted across three hospital sites. An additional four interviews were conducted with five health professionals who held unique roles in the hospital settings (including HMB Staff and Specialist Bereavement Nurses). All focus groups and interviews, each lasting ∼1 hour, were conducted between February and November 2019.
Each focus group was facilitated by one of two researchers (D.N.-C. and K.C.). Where resources allowed (at six focus groups) both researchers were present, with one assuming the role of note-taker and observer and occasionally asking clarifying questions of participants. Each focus group or interview discussed the same topics, listed in Table 1.
Interview Guide
Data analysis
Focus groups and interviews were audio recorded and transcribed for analysis. Each transcript was read in full by two researchers (D.N.-C. and K.C.) before one researcher (D.N.-C.) applied thematic analysis, using NVIVO coding software, to identify the main themes and patterns within the data. 25 Themes were inductively and deductively deduced and then further interrogated utilizing critical questions for interactional analysis from Willis et al. 26 and Moen et al. 27 . This further analytical step allowed us to uncover significant meanings and relationships across themes by asking questions such as which lactation care practices were freely and openly discussed?; which perspectives or care practices elicited the most consensus, contradictions, or conflict?; what factors impacted on competing and contradictory views or practices?; and how did group interactions challenge or confirm participants' stated views? A final coding document outlining key themes that identified and explained current lactation care practices (and their exceptions) was produced and refined after discussion between two researchers (D.N.-C. and K.C.).
Our analysis also drew inspiration from Iedema et al.'s practice of mapping of health care pathways. 28 Mapping can assist health professionals and policy makers to apprehend care delivery from a new angle, and assists in pinpointing where strategic resolution is required and how such interventions may have flow-on effects for the patient or health care system.20,28 Thus, we embarked on mapping the typical lactation care practices and pathways as described by health professionals in the focus groups.
Results
Demographics
One hundred thirteen hospital-based health professionals participated in the study. Detailed characteristics of the participants are shown in Table 2.
Participant Characteristics: Professional Groups by Gender and Years of Professional Experience
Provision of lactation care to bereaved mothers
Health professional participants represented a good mix of the medical, midwifery, and nursing and allied health staff who may interface with bereaved families after stillbirth or infant death (Table 2). Regardless of profession and years of experience, health professionals revealed the acute sense of responsibility they feel to ensure quality compassionate care is provided to bereaved families. This includes attending to the physiological needs of the mother, while also guiding decision making and supporting families to spend time with their deceased infant and create memories in ways that honor their unique circumstances and wishes.
Health professionals explained lactation care practices are ideally situated within the broader multidisciplinary bereavement care families receive in hospital after infant death. Yet, in contrast to the careful and comprehensive bereavement care practices described by health professionals, lactation care was less considered. Common across all sites were concerns that some bereaved mothers may not receive any lactation care or guidance. Moreover, participants explained when lactation care was provided, clinical encounters were likely to be brief and rarely included any recognition of the variable biopsychosocial significance of lactation or breast milk or bereaved mothers' consequent feelings or thoughts about this.
A range of lactation care options were reported by health professionals in focus groups (Fig. 1). Yet, health professionals explained that the full complement of these lactation care options were rarely presented to bereaved mothers. If any lactation care was provided, it was most commonly restricted to facilitating bereaved mothers to suppress their lactation. The modality to achieve this was either through the provision of health information on suppression techniques or the prescription of a pharmaceutical lactation suppression agent. Information on other lactation management options such as sustained expression, the use of milk for other purposes including as memento, or breast milk donation were seldom provided. Figure 1 demonstrates that options other than lactation suppression were only presented to bereaved mothers when certain pre-existing conditions were met. We label these “conditions of care”.
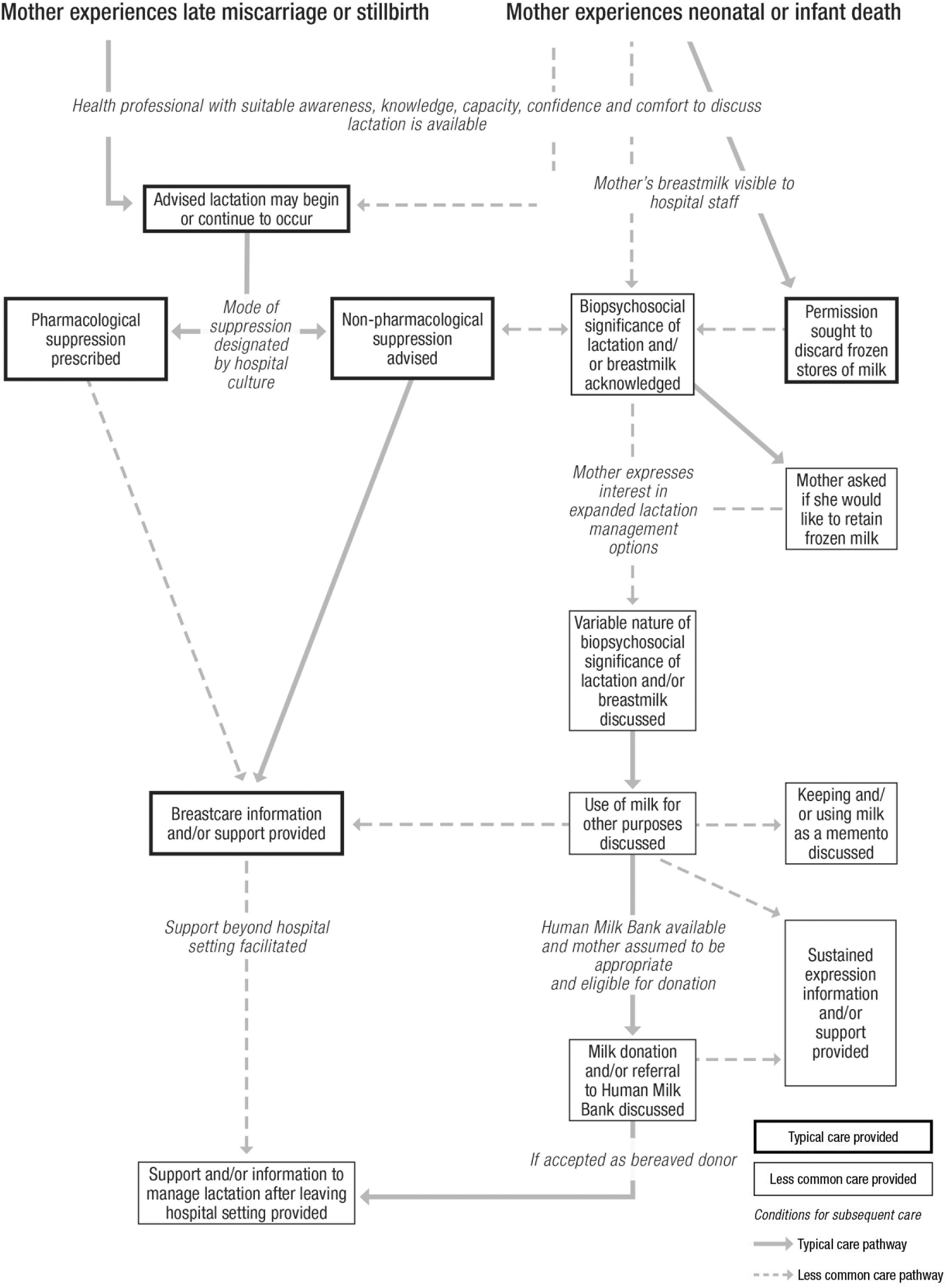
Bereaved lactation care pathway.
The six conditions of comprehensive bereaved lactation care
Health professionals' revealed six conditions of care that influenced the type and scope of lactation care discussed with bereaved mothers (Table 3). Written in “italics” in Figure 1, the conditions of care differentially emphasize the biological, psychological, emotional, or social realm of health care delivery. We label these “conditions of care” because they acted as flow gates through which health professionals need to enter and engage in for a bereaved mother to be offered comprehensive lactation management options. It is only when these multiple and potent conditions of care are satisfied that diverse lactation care and management practices (and their concomitant attention to both the physiological and psychosocial aspects of lactation after infant death) are made available to bereaved mothers. An explanation of each of these conditions of care and the impact they have on the nature and scope of lactation care available to bereaved mothers is summarized below and evidenced in Table 3.
Conditions of Care and Example Quotations
HMB, Human Milk Bank.
Availability of health professionals' with suitable awareness, knowledge, capacity, confidence, and comfort to discuss lactation
The first condition of care reveals that a bereaved mother would only receive lactation care upon interaction with a health professional who has sufficient awareness and knowledge of lactation after infant death, considers bereaved lactation care as a priority in their role, and feels sufficiently comfortable and confident to discuss lactation options with bereaved mothers (Fig. 1). Health professionals possessing each of these characteristics were rare (Table 3).
Health professionals at each hospital site described a lack of well understood policies and practice pathways to designate the provision of lactation care and ensure bereaved mothers received appropriate care before leaving hospital. Rather, lactation care was described as being left to the discretion of individual health professionals, and as a result was haphazard in its delivery or, as the next condition of care exemplifies, relied on established and largely unquestioned hospital practice cultures.
Mode of suppression designated by hospital culture
The second condition of care highlighted the many implicit rules and assumptions about lactation that shape hospital-based lactation care provided to bereaved families (Table 3). The dominant lactation care practice was to advise and facilitate the efficacious and safe suppression of lactation. Prevailing hospital culture determined whether mothers would be offered pharmacological or nonpharmacological suppression options, and health professionals reported that bereaved mothers were rarely presented with a choice between these options. The type of suppression appeared critical in determining the extent of subsequent lactation care information or discussions (Fig. 1). Only mothers advised to pursue nonpharmacological suppression would be likely to receive expanded guidance on how to care for their breasts, or to be engaged in discussion regarding the thoughts and feelings that may accompany the experience of suppressing milk. This points to something of an unquestioned assumption among health care professionals that pharmacological suppression was effective, both physiologically and psychologically, for the mother.
For mothers with existing lactation, for example with infants who had died in a NICU, nonpharmacological suppression was assumed as the most appropriate care option across all hospital sites. Where possible, this was incorporated into care provided to mothers in preparation for infant death. Health professionals explained, however, that the many demands of the NICU setting ensured that mothers may not routinely receive lactation care after the death of their infant.
Mother's breast milk being visible to hospital staff
The NICU was the clinical unit where lactation management options were most likely to be expanded beyond solely advising on suppression. This was mostly due to the higher visibility of frozen stores of breast milk or of a mother's pre-existing pumping of breast milk prompting lactation discussions. If frozen stores of breast milk were present (and the bereaved mother did not have a surviving twin to feed) health professionals explained they were obliged to ask for the mothers' permission before discarding surplus breast milk from the NICU. If the responsible health professional recognized that frozen milk may continue to retain some biopsychosocial significance in the wake of infant death, further lactation management options (such as the mother taking breast milk home with her) may also be presented to mothers.
The mother expressing interest in expanded lactation management options
The majority of health professionals were reticent to raise options other than suppression with bereaved mothers. Consequently, the variable nature of the biopsychosocial significance of lactation and breast milk, and expanded lactation management options were only presented if the mother herself indicated that she was open to, and interested in, pursuing lactation management options beyond suppression.
The onus placed on the mother to instigate these conversations ensured that only a few health professionals had any experience in discussing use of milk for other purposes (perhaps to feed to an older child), keeping milk as memento, or donating milk or sustaining lactation. Health professionals who entered these discussions reported that they did so with trepidation, explaining they received little guidance or support in how to provide this care to grieving families. Health professionals explained that even when some mothers raised these possibilities they were not always supported by the clinical unit or hospital. Informal milk sharing, raised by health professionals in some focus groups, is not depicted in Figure 1 because health professionals explained if it was raised by mothers it was not endorsed, discussed, or supported within hospital settings.
Availability and eligibility to donate to a HMB
If a HMB was easily accessible and breast milk donation considered by the health professional to be an appropriate option for bereaved mothers, mothers may be presented with the option to donate their breast milk. Two hospitals included in our study had an onsite HMB, however, only one of these currently accepted breast milk from bereaved mothers. Furthermore, only a few health professionals working within this setting were aware of the option of bereaved donation. With limited understanding of potential benefits of bereaved donation, mothers wanting to consider donation were reliant on having an interaction with a health professional prepared to raise this discussion, able to articulate the potential benefits that could stem from bereaved milk donation and prepared to refer them to the HMB for further eligibility checks and donor screening.
Support beyond the hospital setting facilitated
Health professionals explained bereaved mothers would rarely receive any lactation information, advice, or support from them that extended beyond the hospital setting. The exceptions to this were mothers who were eligible to receive home visits from a hospital midwife (due to the model of pregnancy or birthing care they were enrolled in) or those who had been referred to the HMB. Social workers or pastoral care workers appeared to have the most flexibility in extending care beyond hospital settings, but these workers had not previously considered lactation relevant to their bereavement care practices. Health professionals assumed that mothers requiring further lactation support would most likely consult their General Practitioner (GP). GPs, however, were not included in our study.
Discussion
The results of this study provide important insights into the nature and scope of contemporary hospital-based lactation care after stillbirth or infant death. Our results indicate that lactation often remains a little considered aspect of Australian hospital-based bereavement care and confirm bereaved mothers are unlikely to receive support to make informed decisions about their lactation or breast milk after the death of their infant.1–3,12,15 Discussions with health professionals indicate any omission of comprehensive lactation care was not deliberate, nor consistent with their expressed desire to provide quality bereavement care to families. By mapping the complex factors involved in clinical decision making and care trajectories described by health professionals, we were able to understand why lactation care is typically limited and then identify several clear entry points for quality improvement to bereaved lactation care.
For bereaved lactation care to be enhanced, our results indicate a fundamental shift in the way lactation after infant death is conceptualized. Comprehensive lactation care is dependent upon acknowledging that lactation is not just a physiological process, but an experience that has variable biopsychosocial significance. The elision of emotional, social, and relational aspects of lactation has long been acknowledged within NICU settings.29,30 Scholars in midwifery advise this elision results in lactation care that is “breast centered” rather than allowing for a “woman centered” approach that can tailor support to the individual needs of the mother.31,32
Sensitive care practices that address the emotional and physical aspects of bereaved mothers' experiences and that promote choice are especially critical for bereaved mothers' health and coping. 16 By reframing hospital-based bereaved lactation care as a biopsychosocial issue, the restrictive, sequential, linear, and gate-keeping pathway we found to be representative of contemporary bereaved lactation care would be disassembled. In its place, health professionals could provide information on the full scope of lactation management options available and ask open ended and nondirective questions. Such an approach would allow mothers to lead conversations and would shed light on the psychological and social components of their needs.33,34 Importantly, these conversations would also likely elicit information on the significant and diverse cultural and religious meanings and practices that may influence bereaved mothers' decision making about what to do with breast milk after loss.1,35 Research with bereaved mothers has demonstrated that respect and understanding of their individual needs and wishes and social and cultural context is critical and that some women benefit greatly from discussing lactation more fully and pursuing options beyond suppression (e.g., keeping milk as memento, or donating breast milk) that can help to honor their motherhood status, maintain connection with their deceased infant, or make meaning in the wake of their death.6,8–10
Moving to more inclusive and comprehensive lactation care is no small task. Utilizing existing evidence-based lactation care guidelines5–7 to enhance hospital policies and practice protocols would be an important first step for improving quality. Inadequate staffing and resourcing, however, often undermines the capacity of health professionals to enact evidence-based lactation practices. 36 These threats and tensions are likely to be intimately connected with multiple other complexities in the clinical microsystem and organizational constraints. 20
Professional role expectations, and policy or procedure development are enmeshed in a complex, unpredictable, and ethically charged clinical environment.20,28 Therefore, changes in one aspect of clinical practice can have unintended ripple effects that influence other areas of clinical practice or culture.20,28 Through mapping, our research depicts the conditions of care in terms of how they are situated in broader lactation care delivery, thus health professionals and quality improvement specialists can work together to anticipate how the ripple effects of policy change may impact both staff role expectations and patient care trajectories in the specific care contexts of individual health services or clinical units.
With complexity and relationships at the center of the conditions of care, it is clear that sustained and multiple strategies will be required to support hospital staff to review and adapt their lactation care practices.37,38 For example, it is likely evidence-based policies will only filter into everyday practices once health professionals feel equipped to hold difficult conversations that allow for shared decision making. 39 The inclusion of lactation care in targeted bereavement care training, recommended for all health professionals, 40 would also assist health professionals with guidance on how to have what are currently considered to be difficult conversations. Local champions who can act as mentors or practice exemplars to others and who advocate for practice change may also be critical in achieving sustainable changes to everyday hospital practices.17,37 The widespread availability of written lactation care resources would also be beneficial in assisting health professionals to provide sensitive information to grieving families. 6
Limitations
Further research is required to attend to some remaining gaps in knowledge, such as the lactation care presented to and required by mothers who experience the death of an older infant, outside of the maternity or NICU hospital system. Research that includes hospital staff from emergency departments, pediatric units, and community-based health professionals such as GPs and children's hospices may provide additional insights. Further research with bereaved mothers and their partners (currently being undertaken by the researchers) will also provide important insights on how they want and need lactation care to be provided. Researchers will be able to develop a further article drawing on the insights gained from health professionals and bereaved families to offer more specificity on the optimal delivery of comprehensive hospital-based lactation care.
Conclusion
High quality bereavement care is critical for the immediate and long-term well-being of women and families after infant death.12,16 Quality maternal health care delivery can be developed by seeking to understand the experiences and practices of health professionals, and then acting upon their unique knowledge and experiences to make positive changes within the broader organizational complexities. 11 Our discussions with hospital-based health professionals highlighted many areas for quality improvement. Like Iedema et al. in 2006, we hope that by mapping contemporary care practices, health professionals may be able to view organizational constraints and habitual patterns of practice from a new angle, and locate opportunities for practice change and quality improvement. 28
The implementation of evidence-based bereaved lactation care policies in HMBs and hospitals, combined with enhanced bereaved lactation care training is urgently required. Moreover, our results highlight the adoption of a biopsychosocial patient-centered approach to lactation care is fundamental to changing the current landscape of conditional care and to ensure mothers are well informed about lactation and presented the full array of lactation management options available to them after infant death.
Footnotes
Acknowledgments
We extend our thanks to the members of our Stakeholder Advisory Group and participating hospitals and health professionals. Thank you to Emily Downie (Australian National University) who assisted in graphic design of the Figure for this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study is funded by the Australian Research Council Discovery Project grant DP180100517 and the Australian National University.