
Abstract
Objective:
We aimed to investigate prospective associations between milk bioactives related to metabolic health (glucose, insulin, leptin, C reactive protein [CRP], and interleukin 6 [IL-6]) and incident formula initiation at 3 and 6 months postpartum.
Design:
This study included 363 mother–infant dyads who were fully breastfed at 1 month and participated in the prospective Mothers and Infants Linked for Healthy Growth study from pregnancy to 6 months postpartum. Associations between milk glucose, leptin, insulin, CRP, and IL-6 at 1 and 3 months and incident formula feeding (FF) at 3 and 6 months, respectively, were tested using multiple logistic regression, adjusting for numerous potential confounders such as maternal age and prepregnancy body mass index.
Results:
At 3 months postpartum, 1-month glucose (odds ratio [OR] 0.45 [95% confidence interval (CI): 0.27–0.75], p ≤ 0.01) and smaller decreases in glucose from 1 to 3 months (OR 0.51 [95% CI: 0.28–0.92], p = 0.03) were associated with lower odds of FF, whereas 1-month leptin (OR 2.30 [95% CI: 1.30–4.07], p < 0.01) and larger increase in insulin (OR 1.86 [95% CI: 1.23–2.81], p < 0.01) and leptin (OR 2.17 [95% CI: 1.29–3.68], p < 0.01) from 1 to 3 months were associated with increased odds of FF. At 6 months, insulin increases (OR 2.08 [95% CI: 1.03–4.17], p = 0.04) were associated with higher odds of FF.
Conclusions:
In a cohort of women with established lactation, 1-month milk glucose, insulin, and leptin predicted initiation of FF at 3 months. Early milk composition may provide a window into mammary gland function, allowing identification of women at risk of not meeting their breastfeeding goals.
Introduction
Breastfeeding and the provision of human milk are the gold standards for infant feeding, as evidenced by their numerous short- and long-term immunologic, metabolic, and neurodevelopmental benefits compared with formula feeding (FF).1,2 The American Academy of Pediatrics recommends exclusive breastfeeding until infants are 6 months of age followed by continued breastfeeding (and introduction of complementary foods) for at least 1 year or as long as mutually desired by the parent and child.1,3,4 However, ∼75% of women in the United States do not meet exclusive breastfeeding guidelines, and 60% of mothers do not meet their own breastfeeding goals.5,6 Although the social determinants and behavioral/psychological factors that predict breastfeeding outcomes are important and fairly well understood (including smoking, education, income, and maternal age),7–9 the interplay between maternal metabolic status and the complex physiological changes underlying lactation initiation, maintenance, and weaning, including individual-level factors such as maternal metabolic health and inflammation have not yet been fully elucidated.10,11 Such mechanisms are important to explore given the changes in maternal nutritional status over the previous 30 years, with increasing rates of obesity 12 and gestational diabetes mellitus (GDM). 13
Research indicates a possible link between altered metabolic health in pregnancy and delayed onset of lactation (the transition from production of colostrum to mature milk secretion, also known as lactogenesis II), which has been associated with the cessation of exclusive breastfeeding at 4 weeks postpartum and conditions such as diabetes and hypertension.14–18 Our group found positive associations between prepregnancy body mass index (BMI) and excessive gestational weight gain (GWG) with bioactive components of human milk correlated with maternal obesity and metabolic health, including C reactive protein (CRP), 19 leptin, 20 insulin, 21 and interleukin 6 (IL-6). 21 Subsequently, human milk biomarkers may provide a noninvasive assessment of mammary gland function at a given moment in time. 22
Less clear, however, is whether the concentrations of (and changes in) milk bioactives may be associated with later breastfeeding outcomes, independent of individual risk factors such as maternal BMI, age, and parity.
In this study, we aimed to investigate the prospective associations between milk bioactives related to metabolic health and incident initiation of FF by 3 and 6 months. We hypothesized that higher concentrations of glucose, insulin, and leptin would be associated with decreased odds of FF, and higher concentrations of CRP and IL-6 would be associated with increased odds of FF.
Methods
Study sample
Data were obtained from the Mothers and Infants Linked for Healthy Growth (MILk) study, a prospective cohort study conducted at the University of Minnesota and University of Oklahoma Health Sciences Center in collaboration with HealthPartners Institute in Minnesota. Inclusion and exclusion criteria have been described elsewhere. 23 A total of 367 pregnant women were enrolled in the study; the final imputed analytic data sample included 363 women after exclusion of four women with BMI outside the inclusion criteria. This study was approved by the Institutional Review Boards of the University of Minnesota, University of Oklahoma Health Sciences Center, and the HealthPartners Institute. Informed consent was obtained from all adult participants. The MILk study is registered with ClinicalTrials.gov (identifier NCT03301753).
Maternal and infant characteristics
Pregnancy history data were collected from electronic health records, including parity, delivery mode, prepregnancy BMI, GWG, and maternal age, race, and education level. Participants were screened for gestational diabetes per standard clinical guidelines. Maternal diet was assessed in the third trimester of pregnancy and at 1 and 3 months postpartum, using the NCI DHQ II food frequency questionnaire, 24 and then the healthy eating index (HEI-2015) total dietary quality score, 25 a measure of adherence to dietary guidelines, was calculated from the frequency of foods reported at each time point and averaged. Infant gestational age at birth and sex were obtained from delivery records.
Participants also completed a prenatal questionnaire on employment, health, social support and beliefs about breastfeeding, and infant feeding intentions and practices in the third trimester of pregnancy (Infant Feeding Practices Study Project First prenatal questionnaire). 26
Breastfeeding status
Breastfeeding status was assessed during study visits when infants were 1, 3, and 6 months of age and was classified based on detailed maternal self-report. All infants were fully breastfed at 1 month.
At 3 and/or 6 months, infants that were provided <24 oz (720 mL) of formula since birth or their last study visit and only human milk for 2 weeks before the study visit were considered fully breastfeeding (FBF). Up to 24 oz of formula (∼1 day worth of formula for an infant receiving 2–3 oz for 8–12 feedings over 24 hours) was allowed for infants in the FBF group to accommodate potential temporary medical indications for formula (early life hypoglycemia, illness, or maternal mastitis). Infants who received >24 oz (720 mL) of formula in addition to some milk since birth or their last study visit were categorized as receiving mixed feedings. Infants who received only formula were fully FF. For these analyses, infants receiving mixed feedings or exclusive FFs were considered to have initiated FF.
Human milk collection
Mother–infant dyads were seen at the study centers within 5 days of the 1 and 3 month time points, between 8:00 and 10:00 am. Mothers were instructed to be ready to breastfeed the infant upon arrival, and then were asked to feed their infant ad libitum from one or both breasts as per usual practice. Two hours after feeding, the mother provided a single complete breast expression sample (until the milk flow stopped) from the right breast using a hospital-grade electric breast pump (Medela Symphony; Medela, Inc., Zug, Switzerland), to account for variations in milk concentration as previously described.27,28 The volume and weight of milk collected from the single breast expression were recorded. Milk was gently mixed, aliquoted, and stored at −80°C within 20 minutes of collection.
Milk hormone assays
Skimmed milk samples were prepared and stored at −80°C for up to 6 months. Insulin, leptin, CRP, and IL-6 were assayed using commercially available enzyme-linked immunosorbent assay kits as previously described. 29 The inter- and intra-assay coefficients of reliability were <6% for all hormones, and limits of quantitation were 0.24 μU/mL for insulin and 7.86 pg/mL for leptin. The inter- and intra-assay variability was 5.5% and 4.7% for CRP and 12.8% and 9.1% for IL-6, respectively. 19 Glucose was measured using the glucose oxidase method (2300 STAT Plus; Yellow Springs Instruments). Assays were batched by dyad over the course of the 4-year study (total of five batches), with the 1 and 3 months samples for each dyad assayed within the same batch.
Statistical analysis
To characterize the study sample, maternal and infant characteristics are presented by feeding status at 6 months as means ± SE for continuous variables and frequencies (n, %) for categorical variables. Differences in responses to the maternal prenatal survey between those in the FF and FBF groups at 3 and 6 months postpartum were compared using Fisher's exact tests.
Multiple imputation by chained equations with fully conditional specification was conducted to form a more comprehensive analytic data set. Before imputation, 276 participants had complete sets of milk bioactives and maternal characteristics available for analysis (24% missing). The percentage of missing values for individual variables ranged from 6% to 15%.
The data were first assessed for influential outliers by plotting the Pearson chi-square difference and deviance difference against predicted probability. Outliers with a confidence interval displacement diagnostic >1.5 were flagged and only retained in the model if they did not significantly change the associations between predictors and outcome variables (no outliers removed from the final data set). Model fit was assessed using the Hosmer and Lemeshow test. A total of 40 data sets were then imputed using predictive mean matching before pooling for analysis. Data were assumed to be missing at random. For comparison, we also performed analyses on the subset of complete cases and obtained similar results.
Milk bioactives and their changes from 1 to 3 months were standardized to a distribution of mean = 0, standard deviation = 1 before regression analysis to aid comparison of effect sizes, due to the wide variability among them in mean concentration and units of measurement. Crude and adjusted logistic regression models were then used to test associations of 1 month milk bioactive concentrations and the change in these concentrations from 1 to 3 months, with incident FF by 3 months. Among the 87% of women who were still FBF at 3 months, the association of 3 months milk component concentrations and the change in concentrations from 1 to 3 months were then tested as predictors of incident FF by 6 months.
Adjusted models controlled for potential confounders and technical factors (study center, maternal education level, race, age, parity, prepregnancy BMI, oral glucose challenge test (OGCT) value, delivery mode, average dietary quality score, and milk assay batch). Because decreased milk output is linked to early breastfeeding cessation, we also constructed a model adjusting for milk output volume from a single feed for bioactives associated with the outcome. p-Values <0.05 were considered significant. Statistical analyses were performed using SAS Enterprise (SAS Institute, Inc., Cary, NC).
Results
Maternal characteristics
Of 363 mothers, all of whom exclusively breastfed for at least 1 month for inclusion in the study, 86% were FBF at 3 months, and 74% were still FBF at 6 months (Table 1). Most (85%) mothers were non-Hispanic white and had a bachelor's/graduate degree (76%). Approximately 31% had prepregnancy BMI classified as overweight and 23% as obese.
Maternal Characteristics by Infant Feeding Status at 6 Months Postpartum (n = 363)
Formula feeding defined as receiving only formula at 3 and 6 months postpartum or receiving >24 oz (720 mL) since birth or their last study visit.
Full breastfeeding defined as receiving <24 oz (720 mL) since birth or their last study visit and only breast milk for 2 weeks before the study visit.
American Indian 1.5%, Asian 3%, Black 5%, Pacific Islander <1%, other 3%, more than one race 1.5%.
Milk output is a single complete breast expression sample in mL.
BMI, body mass index; GED, general educational development; SE, standard error.
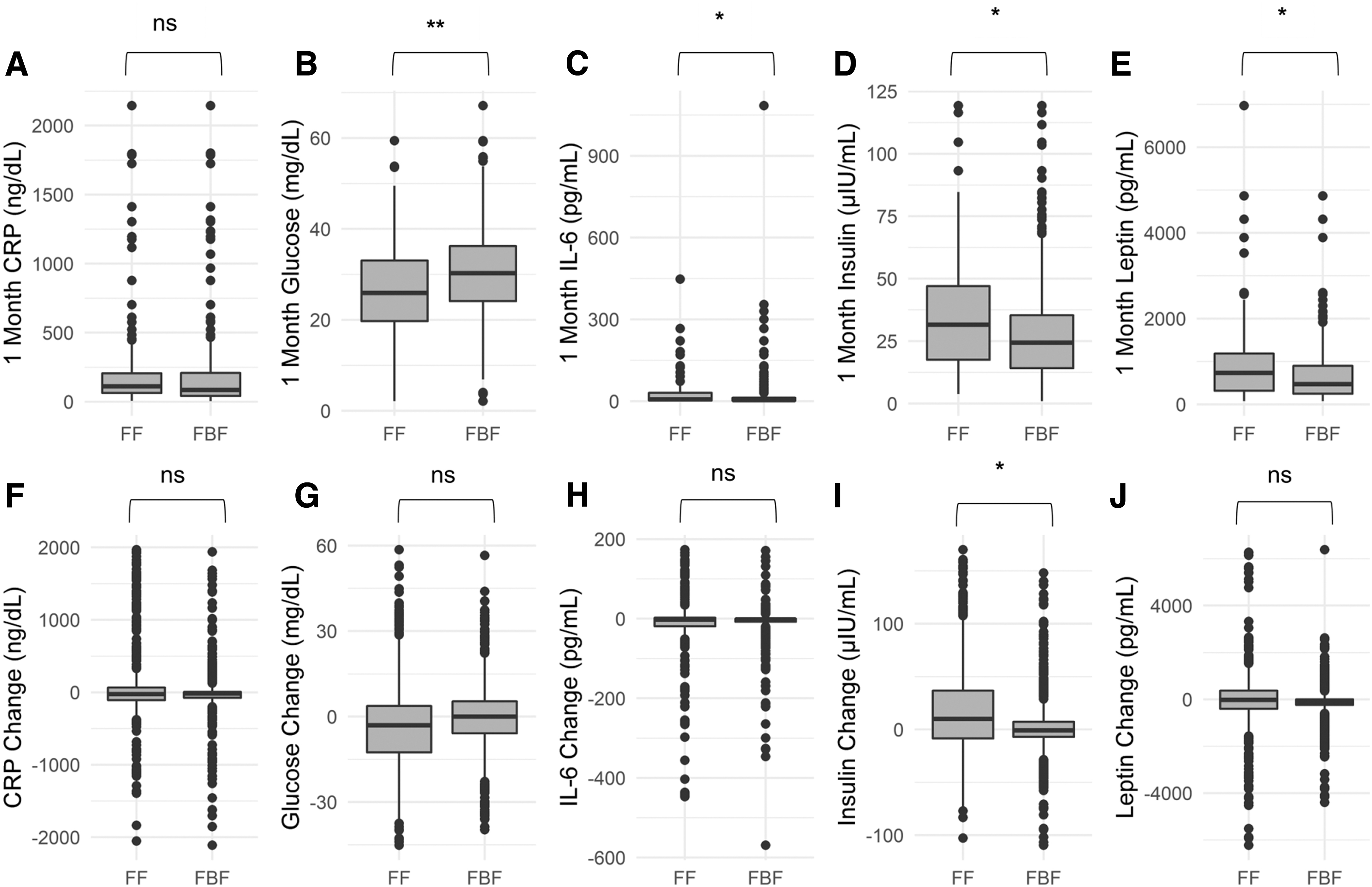
On average, participants who were FF by 3 months had lower milk glucose at 1 month postpartum than those in the FBF group (FF: 25.9 ± 1.68 mg/dL, FBF: 30.7 ± 0.57 mg/dL; p = 0.01) (Fig. 1). Concentrations of milk insulin were higher in FF participants (FF: 37.5 ± 4.04 μIU/mL, FBF: 28.9 ± 1.14 μIU/mL; p = 0.03), who also had larger increases in insulin concentration from 1 to 3 months (FF participants: 22.1 ± 8.45 μIU/mL, FBF participants: 0.41 ± 1.08 μIU/mL; p = 0.02). Similarly, higher mean leptin concentrations (FF: 1077.6 ± 194.1 μIU/mL, FBF: 658.7 ± 34.1 μIU/mL; p = 0.04) were observed for FF participants.
Milk bioactive concentrations at 1 month
Among participants who completed the prenatal questionnaire, confidence in breastfeeding, plans to breastfeed or express breast milk while at work, and beliefs about exclusive breastfeeding were not different between participants who had introduced formula and those who were FBF at 3 months. No difference in confidence in breastfeeding for the desired length of time was observed between groups (p = 0.07). However, among participants with parity >0 (n = 204), a greater percentage of FF participants had no previous breastfeeding history (11%) compared with those who were FBF at 3 months postpartum (2%, p = 0.03).
The 314 participants who were FBF at 6 months had similar prenatal plans to breastfeed at work (79% FBF, 83% FF, p = 0.30), agreed that exclusive breastfeeding is best for an infant's first 6 months of life (65% FF, 72% FBF, p = 0.38), although notably this is a difference of 7%. Both groups had similar breastfeeding experience (n = 177; 98% FBF, 100% FF, p = 1.0) and breastfeeding confidence (p = 0.35).
Breast milk components and incident initiation of FF
After adjustment for potential confounders, 1 month milk glucose (odds ratio [OR] 0.45 [95% confidence interval (CI): 0.27–0.75]; p = 0.003) and the smaller decreases in glucose concentration from 1 to 3 months (OR 0.51 [95% CI: 0.28–0.92]; p = 0.027) were associated with decreased odds of FF by 3 months (Table 2). Larger increases in milk insulin concentration from 1 to 3 months (OR 1.86 [95% CI: 1.23–2.81]; p = 0.004) were associated with higher odds of FF. Milk leptin at 1 month (OR 2.30 [95% CI: 1.30–4.07]; p = 0.004) and increases in milk leptin concentration from 1 to 3 months (OR 2.17 [95% CI: 1.29–3.68]; p = 0.004) were also associated with higher odds of FF. No associations were observed between 1-month CRP and IL-6 (or their changes from 1 to 3 months), and the odds of FF by 3 months.
Relationship of Human Milk Bioactives and Their Changes from 1 to 3 Months Postpartum with Formula Initiation at 3 and 6 Months
Association between milk bioactive concentrations at 1 and 3 months postpartum and changes in concentrations from 1 to 3 months and odds of formula initiation at 3 and 6 months.
Bold values indicate significance at p < 0.05.
Milk component values have been standardized to distribution of (0,1).
Adjusted for study center, education, age, parity, race, batch, maternal prepregnancy BMI, OGCT result, delivery mode, and mean HEI-2015 score.
Models include only participants fully breastfeeding at 3 months.
BMI, body mass index; CI, confidence interval; CL, confidence level; CRP, C reactive protein; HEI-2015, healthy eating index; HM, human milk; IL-6, interleukin 6; OGCT, oral glucose challenge test; OR, odds ratio.
At 6 months, increases in milk insulin concentration from 1 to 3 months postpartum were associated with higher odds of FF (OR 2.08 [95% CI: 1.03–4.17]; p = 0.041). No other 3-month milk component concentrations or changes from 1 to 3 months were associated with FF by 6 months postpartum.
Milk bioactive concentrations, milk output, and incident FF
Adjustment for 1 month maternal milk output from a single breast expression and changes in output from 1 to 3 months postpartum did not have a significant effect on the ability of glucose to predict initiation of FF by 3 months postpartum in adjusted models (Table 3). Leptin and changes in its concentration from 1 to 3 months and changes in insulin concentration from 1 to 3 months were slightly weaker after adjusting for milk output. The odds of initiating FF, however, remained within 10% of the original OR.
Relationship of Human Milk Bioactive Components and Milk Output and Their Changes from 1 to 3 Months Postpartum with Formula Initiation at 3 and 6 Months
Association between milk component concentration, milk output at 1 and 3 months postpartum, and changes in concentration from 1 to 3 months and odds of formula initiation at 3 and 6 months.
Bold values indicate significance at p < 0.05.
Milk bioactive concentrations have been standardized to distribution of (mean of 0 and standard deviation of 1).
Adjusted for study center, batch, and maternal education, age, parity, race, prepregnancy BMI, OGCT result, delivery mode, and mean HEI-2015 diet quality score.
Models include only participants fully breastfeeding at 3 months.
Milk output is a single complete breast expression sample in mL.
Change in output from 1 to 3 months postpartum in mL.
BMI, body mass index; CI, confidence interval; CL, confidence level; HEI-2015, healthy eating index; HM, human milk; OGCT, oral glucose challenge test; OR, odds ratio.
At 6 months postpartum, after adjustment for 3 month milk output and the change in output from 1 to 3 months postpartum, the increase in insulin from 1 to 3 months was no longer predictive of incident FF (OR 2.00 [95% CI: 0.98–4.08], p = 0.06) in the adjusted model. The resulting OR was slightly smaller but within 10% of the original OR.
Discussion
In this study, we examined for the first time whether concentrations of human milk bioactives were associated with incident initiation of formula over 6 months of follow-up, in a cohort of healthy women, all of whom were FBF for at least 1 month. Our study provides a unique look at possible milk-based biomarkers that may be used to predict initiation of formula.
Prenatal surveys revealed no difference in confidence or beliefs about breastfeeding between FF and FBF participants at 3 and 6 months postpartum. This replicates prior findings that social and psychological determinants do not completely account for breastfeeding outcomes. 30 Because the aim of the parent study is to understand milk bioactive concentrations and their changes in relationship to breastfeeding and infant outcomes, our cohort was designed to include only women who were highly likely to sustain breastfeeding. This design, although clearly not representative of all breastfeeding women in the population, allowed us to focus on the potential physiological differences between women who met their goals for full breastfeeding and those who did not, at a time point when they were all still FBF.
Leptin is an appetite-regulating hormone31–33 elevated in the serum and milk of women with elevated BMI. 20 Previous studies reveal that maternal serum leptin and milk leptin are positively correlated (r = 0.42–0.55).34,35 In our study, higher 1-month concentration and greater increases in milk leptin from 1 to 3 months were associated with increased odds of FF by 3 months. The mechanisms by which higher milk leptin might disrupt full breastfeeding are not clear, but leptin has been shown to inhibit muscle contractions in vitro. 36 Myoepithelial cells of the mammary gland express leptin-specific receptors and in obese mice, elevated plasma leptin inhibited the effect of oxytocin on myoepithelial contracting, slowing milk ejection. 37 Researchers also hypothesized that elevated levels of leptin may cause prolactin resistance, thereby impairing lactation, as has been reported in a rodent model of obesity. 37 It has been reported that serum leptin is inversely associated with serum prolactin and with 24-hour milk expression in lactating women. 38 Leptin is also observed to reduce infant appetite in animal models, 39 and thereby could reduce infant demand and milk volume.
Cannon et al. found that leptin dose and infant feeding volume were positively associated (p < 0.001), and larger feeding volumes (>105 g) were associated with decreased leptin concentrations in milk postfeeding (mean decrease of 0.02 ng/mL in skimmed milk; p = 0.009). 40 This may suggest that mothers with smaller total milk output had higher concentrations of leptin in their milk. Thus, the positive association of milk leptin with initiation of FF found in this study is in alignment with mechanistic work suggesting that elevated leptin depresses milk supply, perhaps through effects on lactation (prolactin and oxytocin release or action) or reduced infant demand. It is possible, however, that elevated leptin serves as a marker of lactation difficulty and does not directly depress lactation. More work is needed to elucidate the complex relationship of adipokines with mammary gland development and function in humans.
In our study, larger increases in milk insulin from 1 to 3 months were associated with increased odds of FF by 3 and 6 months postpartum. Maternal obesity, GDM, and insulin resistance are associated with elevated milk insulin levels,41,42 and with breastfeeding difficulties, including DOL 43 and early breastfeeding cessation, 44 although this is not always observed. 45 None of the participants in our study had type I or II diabetes or met the criteria for GDM, but it is possible that even slight impairments in glucose tolerance (indicated by higher levels of milk insulin) may impact lactation. Verd et al. showed that mothers who had mildly impaired glucose tolerance during pregnancy had increased odds of early exclusive breastfeeding cessation (OR 1.65 [95% CI: 1.11–2.45]; p = 0.01). 46 Of note, in this study of normoglycemic women, the milk insulin—FF associations were independent of maternal OGCT results.
Nommsen-Rivers' review of the literature discusses the important mechanistic role for insulin in milk synthesis and secretion, hypothesizing that low milk supply, one of the most often-cited reasons for weaning, may stem from impaired insulin action. 15 The review also highlights the role of insulin in the expression of genes (Stat5a and Elf5 47 ) involved in milk protein synthesis and presents animal models showing that inhibiting insulin receptor gene expression in the mammary gland (mimicking insulin impairment) leads to significant downregulation of many genes involved in milk synthesis. 48 In sum, there is both an epidemiological and molecular basis for the novel observation that greater milk insulin and its degree of increase from 1 to 3 months increase the odds that mothers will initiate FF.
Milk glucose at 1 month and smaller decreases in milk glucose concentration from 1 to 3 months were associated with lower odds of FF by 3 months postpartum among the women in our study. Glucose is a precursor for lactose, the primary sugar in human milk, and consequently, the mammary gland requires an adequate supply of glucose to produce milk. 49 Although some glucose is taken up for the production of lactose, another portion is secreted from the mammary epithelial cells into the milk through apical transporters. 50
Neville et al. confirmed the equilibration of glucose across the apical membrane of mammary cells in vivo by measuring the infusion of glucose labeled with stable isotopes into lactating women. 51 They found that milk glucose concentrations were proportional to the rate of milk secretion, such that glucose concentrations in the mammary cells decreased as milk synthesis decreased. Thus, our finding that higher milk glucose is associated with lower odds of FF appears to be consistent with what is known about the regulation of milk secretion, in that if higher milk glucose concentration reflects greater milk secretion and supply, then it should also predict longer FBF.
CRP is an acute phase protein and IL-6 is a cytokine that are present in higher quantities in the presence of inflammation and metabolic conditions.52,53 We hypothesized that milk CRP and IL-6 would be positively associated with FF but did not discern any relationships. However, milk concentrations of IL-6 may not be reflective of maternal serum levels, and breast milk receptors have a low affinity for IL-6.54–56 Thus, it is possible that these cytokines, although involved in other processes such as the development of infant immunity, 57 are not reflective of mammary gland function.
We found that the relationships between milk bioactives and FF were not significantly altered by adjusting for maternal milk output from a single feeding and thus, concluded that the observed associations are independent of the total volume expressed for one feeding. However, it is plausible that this single feeding volume is not representative of total daily milk output. Further studies examining these relationships and total output are needed.
Strengths of our study include its prospective cohort design in which assessment of the milk bioactives was conducted when all women were FBF, and the ability to adjust for numerous maternal demographics and clinical characteristics that could serve as potential confounders. Tight control of milk collection timing and use of a standardized protocol increased rigor of the study. Finally, we provided a novel examination of associations between milk bioactives and breastfeeding outcomes at two postpartum periods among healthy women.
Study limitations include inexact measurements of breastfeeding duration as infant feeding status was only assessed at 1, 3, and 6 months postpartum and, therefore, duration could only be defined as 1–3 months, 3–6, and ≥6 months. This imprecision may have reduced our ability to detect relationships at the later time point (3 months milk concentrations predicting 6 months FBF). In addition, our study cohort, which consisted of mostly non-Hispanic white highly educated middle to upper class women with a high rate of breastfeeding exclusivity, was not representative of the general population or FBF trends in the United States. 58
Conclusion
In summary, concentrations of milk bioactives early in lactation provide a window into mammary gland function and may help identify women at risk of not meeting their breastfeeding goals.
Footnotes
Acknowledgments
We would like to acknowledge and thank all the women and health care providers who contributed to the MILk study. We also acknowledge the valuable assistance of Neely Miller and Kristin Sandness and the resources of the Center for Neurobehavioral Development, Rebecca Hollister from the Center for Pediatric Obesity at the University of Minnesota, the Clinical and Translational Research Services support team at the Clinical and Translational Science Institute at the University of Minnesota (supported by grant no. UL1TR002494 from the National Institutes of Health's National Center for Advancing Translational Sciences), laboratory resources from the University of Oklahoma Health Sciences Center, and Elisabeth Seburg at the HealthPartners Institute.
We also acknowledge use of the following resources: Diet*Calc Analysis Program, Version 1.5.0. National Cancer Institute, Epidemiology and Genomics Research Program. October 2012. Diet History Questionnaire, Version 2.0. National Institutes of Health, Epidemiology and Genomics Research Program, National Cancer Institute. 2010. DHQ Nutrient Database. ![]() . National Cancer Institute, Epidemiology and Genomics Research Program. Study data were collected and managed using REDCap electronic data capture tools hosted at the University of Minnesota. REDCap (Research Electronic Data Capture) is a secure web-based software platform designed to support data capture for research studies.59,60
. National Cancer Institute, Epidemiology and Genomics Research Program. Study data were collected and managed using REDCap electronic data capture tools hosted at the University of Minnesota. REDCap (Research Electronic Data Capture) is a secure web-based software platform designed to support data capture for research studies.59,60
Authors' Contributions
E.W.D. and D.A.F. designed the research; L.F. and K.D. conducted the research; E.M.N. analyzed the data and drafted the original article; K.J., H.K., and J.H. assisted with data analysis; L.K., D.R.J., L.H., E.O.K., S.P., and D.A.F. critically reviewed the article; E.W.D. had primary responsibility for final content. All authors read and approved the final article.
Disclosure Statement
D.R.J., D.A.F., L.H., E.O.K., and E.W.D. report grant funding from the National Institute of Child Health and Human Development (NICHD) during the conduct of this study. National Institute of Dental and Craniofacial Research (NIDCR). E.M.N. reports funding on a grant from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). No other conflicts of interest or financial disclosures were reported.
Funding Information
This study used data from MILk study. The MILk study is supported by an NIH/NICHD grant (R01HD080444). K.E.J. received support from NIDCR (T90DE0227232). E.M.N. was supported by the NIH/NIDDK grant (T32DK083250).