
Abstract
Background:
In the United States, 5% of breastfeeding mothers report using cannabis. Frequent cannabis use results in higher delta-9-tetrahydrocannabinol (THC) in breast milk, and mode of cannabis use may also impact risk to the infant. The aim of this study was to understand how breastfeeding mothers use cannabis and factors related to frequency of its use.
Methods:
An anonymous online survey was conducted among mothers who used cannabis while breastfeeding. Frequency of cannabis use was ascertained along with modes of and reasons for cannabis use. Respondents were grouped by frequency of use: less-than-daily (n = 686), low-daily (1–3 times/day; n = 423), and high-daily (≥4 times/day; n = 218). Chi-square and analysis of variance tested between-group differences, and ordinal logistic regression examined factors associated with cannabis use frequency.
Results:
Smoking (88%) was the most common mode of cannabis consumption, followed by vaping (48%) and oral/edibles (36%). Smoking and vaping differed by cannabis use frequency. Only 54% used cannabis to get high, but was reported more among frequent users. In contrast, 89% of mothers used cannabis for mental or physical health symptoms, including anxiety, depression, gastrointestinal symptoms, chronic pain, and posttraumatic stress disorder. These symptoms differed by cannabis use frequency. Reporting more symptoms was associated with higher frequency of use. The odds of increasing cannabis use frequency was 2.7 for those reporting 1–2 health reasons, 5.6 for those reporting 3–4 health reasons, and 13.1 for reporting ≥5 health reasons.
Conclusions:
Strategies are needed to address maternal mental and physical health, which may be key to reducing cannabis use among breastfeeding mothers.
Introduction
In the United States, cannabis is classified federally as an illegal Schedule I drug 1 ; however, it has been legalized for recreational use in 17 states and for medical use in 26 states. 2 Because cannabis is now legal in many states, more people accept its use, including during pregnancy and breastfeeding. A recent study of cannabis use among perinatal women found that cannabis use was 1.5 to 2.2 times higher in states where cannabis was legal compared to those where it was illegal. 3 A recent study based on Pregnancy Risk Assessment Monitoring System (PRAMS) data from seven states found that 5.5% (n = 366) of postpartum women were using cannabis, 81% of whom were also breastfeeding. 4
Cannabis exposure during pregnancy and breastfeeding is concerning because its psychoactive component, delta-9-tetrahydrocannabinol (THC), is known to cross the placenta and transfer into breast milk, and it acts on the endogenous cannabinoid system. Negative impacts on fetal growth and early neonatal behaviors have been observed, 5 and long-term effects on neurodevelopment have been found.6,7
Cannabis exposure after 5–6 weeks gestation was related to a number of pathologies during adolescence, including sleep and cognitive difficulties. 8 However, a major challenge of studying prenatal cannabis exposure is to control for other aspects of social disadvantage that co-occur with cannabis use. Velez and colleagues 9 noted that there have been two longitudinal studies that controlled for social disadvantage and found delayed effects in learning and memory for adolescents exposed prenatally.
Prenatal exposure to cannabis is likely more potent than exposure during breastfeeding. Nevertheless, the American College of Obstetricians and Gynecologists, the American Academy of Pediatrics, and the U.S. Surgeon General recommend that mothers abstain from cannabis use while breastfeeding.10–12 The Academy of Breastfeeding Medicine recommends that breastfeeding mothers who use cannabis be counseled to reduce or eliminate use of cannabis and advised of possible long-term neurobehavioral effects. 13 Although the independent effect of THC exposure via breast milk is difficult to discern since infants are also often exposed prenatally, THC does enter breast milk and, therefore, poses a potential risk to the breastfed infants.7,14,15
Frequency of cannabis use is important because it is related to accumulation of THC in breast milk. More THC accumulates in breast milk of chronic than occasional users. 15 A study of 50 breastfeeding women who used cannabis found that THC levels were highly variable. 15 THC was detectable in 63% of the milk samples and was more likely to accumulate in breast milk among those who reported frequent cannabis use. The authors raised concerns that daily use would increase cannabinoid accumulation in infants. In another recent study of 20 chronic cannabis users, THC was measured in milk and plasma at both 2 weeks and 2 months postpartum. 16 Between these two time points, mothers increased their frequency of cannabis use, and the breast milk THC concentration increased by 30.1 ng/mL. Furthermore, THC was more concentrated in the milk than the plasma.
Cannabis use postpartum includes other concerns, including second-hand smoke exposure, a risk factor for Sudden Infant Death Syndrome (SIDS). 17 High levels of indoor air particles have been measured in households where cannabis is smoked. 18 Furthermore, tobacco use is prevalent among cannabis users; PRAMS data indicate that 27% of women using cannabis while breastfeeding also smoke tobacco. 19
In terms of risk to infants when breastfeeding mothers use cannabis, two factors are particularly salient: frequency of use, which is related to the amount of THC in breast milk, and mode of consumption, which determines whether there will be second-hand smoke exposure. Because little is known about mode of consumption and frequency of cannabis use while breastfeeding, the present study examined frequency of cannabis use and mode of cannabis consumption in a large sample of mothers who used cannabis while breastfeeding.
Methods
Survey development
An online survey was developed to obtain information about how and why mothers use cannabis during pregnancy and breastfeeding. The survey was developed by researchers with expertise in psychology, lactation, obstetrics/gynecology, and pharmacology. The initial survey questions were developed based on factors that were related to substance use, in general, and cannabis use in particular.
First, a review of the literature was completed to identify important variables to include. An initial survey draft was reviewed by members of an online community that supported pregnant and breastfeeding mothers who used cannabis. Based on their feedback, another survey draft was completed. Since this was a new area of study, many of the questions were developed and piloted for the present study. The survey was then pretested by ∼300 individuals who used cannabis while pregnant or breastfeeding and provided written feedback. They suggested small wording changes and suggested using the word “cannabis” rather than “marijuana” as this term would be more acceptable to the mothers completing the survey. The final edits were made through two rounds of suggestions by the Institutional Review Board (IRB). The IRB specifically insisted that we not ask participants their state of residence since cannabis was not legal across the United States and they feared possible consequences for the women who participated.
This survey obtained information on maternal age, parity, and youngest child's age as continuous variables. Education, race/ethnicity, household income, alcohol and tobacco use, and other demographics (Table 1) were obtained as categorical variables. Frequency of cannabis use was assessed with two questions (described in the Analyses section). Modes of cannabis use were assessed using a multiple-choice question in which multiple selections could be made, and a space to write in other methods was provided. Reasons for cannabis use were also assessed through a multiple-choice question; participants could select all options that applied and write in additional reasons.
Demographics for Total Sample and Subgroups by Cannabis Use Frequency While Breastfeeding
Cannabis use frequency subgroups are as follows: “Less-than-daily user” used cannabis ≤6 times per week; “Low-daily user” used cannabis 1–3 times daily; “High-daily user” used cannabis ≥4 times daily.
Bolded p-values indicate those that are statistically significant.
p Value of analysis of variance between means of cannabis use frequency subgroup.
p Value of Pearson's chi-square for differences between cannabis use frequency subgroups.
p Value of nonparametric test for trend.
NICU, neonatal intensive care unit.
To participate in the survey, mothers had to be at least 18 years old and used cannabis while pregnant or breastfeeding. The survey was available through the InfantRisk Center website and distributed through their social media platforms where this information could be shared and distributed further. In addition, specific support groups for mothers who use cannabis shared the survey through their own social media pages. The survey was open from May 2018 through August 2019.
This study was approved by the IRB at Texas Tech University Health Sciences Center.
Analyses
Analyses for this article were limited to those who reported using cannabis while breastfeeding. Out of the 2,165 surveys that were submitted, 1,679 met the inclusion criteria (Fig. 1). An additional 163 were excluded due to excessive missing data, and 189 provided insufficient information about frequency of cannabis use, resulting in a final sample size of N = 1,327 (Fig. 1).

Study sample flow chart.
Respondents were grouped by frequency of cannabis use. The questions used to create the groups were: (1) “In an average week, how often did or do you use cannabis while breastfeeding?” and (2) “In an average day, how often did or do you use cannabis while breastfeeding?” Based on responses to these two questions, respondents were categorized as less-than-daily use (cannabis use six times per week or less; n = 686), low-daily use (cannabis use one to three times per day; n = 423), and high-daily use (cannabis use four or more times per day; n = 218).
Age of respondents' children varied considerably; thus, we created categories for youngest child's age: 0 to <6, 6 to <12, and ≥12 months. Given insufficient numbers in different racial/ethnic groups, groups were combined which resulted in three final groups: (1) white/non-Hispanic, (2) Hispanic, and (3) black, indigenous, and people of color.
One-way analysis of variance was tested for differences in continuous demographic variables (maternal age, youngest child's age, parity) by frequency of cannabis use. Pearson chi-square tests were used to test for differences in categorical variables by cannabis use frequency. Given low numbers in some cells, the nonparametric test for trend was used for income.
Ordinal logistic regression was used to examine factors associated with the three levels of frequency of cannabis use. After bivariate analyses of the independent variables, we included those with p < 0.1 in the model (number of health reasons [0, 1–2, 3–4, ≥5], p < 0.001; education [≤high school education, some college, ≥bachelor's degree], p < 0.001; marital status [married, single, other], p < 0.001; cannabis use to get high [yes/no], p < 0.001; alcohol use [yes/no] p < 0.001; tobacco smoking [yes/no] p < 0.001; household income [<25,000, $26,000–$50,000, $51,000–$75,000, and $76,000 or more]). Tests of parallel lines were conducted to ensure that all assumptions were met for the model and odds ratios are reported.
Results
The majority of survey respondents lived in the United States (91%) and Canada (6%), and the remaining 3% lived in several other countries across the globe. The mean age of respondents was 30 years, and 44% had children <12 months old at the time of the survey. Seventy-nine percent were White, and 53% had some posthigh school education, but less than a bachelor's degree. More than half were married, and over half had household incomes between $26,000 and $75,000 (Table 1).
Frequency of use differed by education, household income, and marital status. There were no differences based on maternal age, parity, youngest child's age, or race or ethnicity. A relatively low proportion (23.8%) of this sample ever used formula, but this increased with increasing cannabis use frequency (p = 0.001) (Table 1).
Seventy-six percent of participants who used cannabis while breastfeeding also used cannabis while pregnant, and nearly all (97.7%) of the high-daily users used cannabis while pregnant compared to only 67.3% of the less-than-daily users. Alcohol use was more prevalent among the less-than-daily cannabis users, but tobacco use was more prevalent among the high-daily cannabis users (Table 1).
How cannabis was consumed
Most participants consumed cannabis through more than one method, including smoking (88%), vaping (47%), and oral/edibles (35%). Oral tincture and topical methods were also reported (Fig. 2). Smoking (p < 0.001) and vaping (p = 0.001) differed by cannabis use frequency and were more often used by the most frequent users.
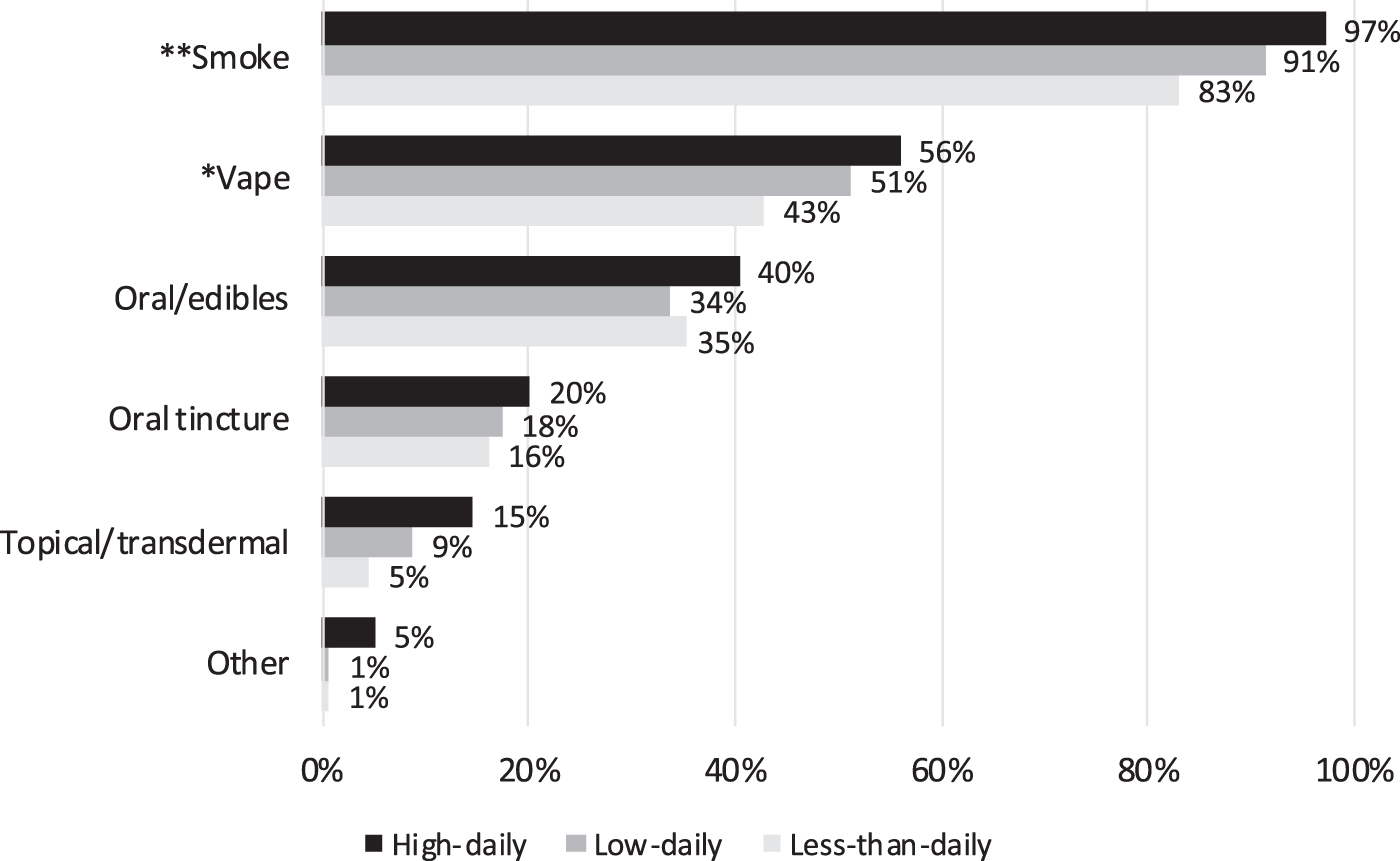
Mode of cannabis consumption stratified by frequency of cannabis use. More than one mode could be selected.
Reasons for cannabis use
Among the total sample, only 54% reported using cannabis to “get high,” but this differed by cannabis use frequency. More high-daily users (67%) were using it to get high than low-daily (52%) or less-than-daily (50%) users (p < 0.001).
A strikingly high proportion (89%) of respondents used cannabis to address at least one health problem. In fact, two, three, or four health-related reasons for using cannabis were reported by 19%, 26%, and 19% of the total sample, respectively. Two participants reported eight health-related reasons.
Among the health-related reasons, the most highly reported were anxiety (87%) and depression (70%). Gastrointestinal symptoms and disease (54%; included appetite, nausea, irritable bowel syndrome, and to a lesser extent inflammatory bowel disease), chronic pain (46%), and posttraumatic stress disorder (PTSD) (34%) were also common reasons. For each of the top five health-related reasons, significant differences (p < 0.001) were observed by cannabis use frequency. Women who used cannabis more frequently were more likely to report using it to address health symptoms (Fig. 3).

The top five health-related reasons for cannabis use stratified by frequency of cannabis use. GI symptoms/disease included nausea, vomiting, increasing appetite, irritable bowel syndrome, and to a lesser extent inflammatory bowel disease.
Less common, yet medically important, reasons for cannabis use included acute pain (6%), sleep disorders (6%), autoimmune or inflammatory disorders (3%), other psychiatric disorders (2%), and seizures or epilepsy (1%). Notably, in a later question about nonhealth-related reasons, 77% of the total sample reported using cannabis to aid with sleep.
Predictors of cannabis use frequency
Ordinal logistic regression indicated that number of health reasons, education, tobacco smoking, alcohol use, and “getting high” were all significant predictors of cannabis use frequency. Marital status and household income, while significant in bivariate analyses, were not significant in the model (Table 2). When household income was removed, education became a more significant predictor; when marital status was removed, there was virtually no change in the remaining variables (data not shown).
Predictors of Frequency of Cannabis Use While Breastfeeding
Bolded values are significant with p < 0.05.
aOR = aOR from ordinal logistic regression model.
aOR, adjusted odds ratio; CI, confidence interval.
Number of health reasons reported was the strongest predictor of cannabis use frequency (Table 2). Mothers reporting one to two health reasons for cannabis use had an approximate twofold increased odds of more frequent cannabis use than those who reported none. For mothers who reported three to five health problems, the odds of higher cannabis use was 5.6 and for those reporting five or more health reasons it was 13.1.
Discussion
Health reasons were by far the strongest predictor of frequent cannabis use among mothers who used cannabis while breastfeeding, and the number of health problems increased the likelihood of frequent use by 2 to 13 times compared to those who reported no health reasons. Importantly, three of the top five reported health reasons were related to mental health: anxiety, depression, and PTSD. Use of cannabis for psychopathologies has been reported by others in general populations20,21 and among pregnant women. 22 In fact, in a study of PRAMS data, ∼80% of mothers who used cannabis reported using it to “relieve stress/anxiety,” which notably included depression, PTSD, and bipolar disorder. 22
Our findings indicate that more mothers used cannabis while breastfeeding to address a specific health problem (89%) than to get high (54%). Understanding why mothers use cannabis may help health care providers develop appropriate strategies for addressing symptoms for which cannabis is used.
In some cases, nonpharmacologic treatments, such as cognitive-behavioral therapy, mindfulness, yoga, or exercise, may be indicated to address mental or physical health problems. 23 In other cases, prescription medications may be indicated, although acceptability may be an issue as cannabis is often considered a “natural alternative” to medications. In one study, women overwhelmingly believed that “natural” products were safer than prescription medications while breastfeeding. 24 This may help explain findings of Bartlett et al. 25 that pregnant women who used cannabis continued to use it despite believing that it transferred to the fetus during pregnancy and to the infant while breastfeeding. More and larger studies are needed to understand the risks of maternal medication use and cannabis use while breastfeeding to provide stronger evidence-based guidance to mothers.
Anxiety was the most frequently reported reason for cannabis use. Mothers are faced with many stressors, including caring for their infant, house work, food preparation, and breastfeeding. In addition, many also face challenges of domestic violence, trauma, substance use, and smoking cessation. Most health care providers are not equipped to provide assistive services for all of these issues, but knowing what is available in the community can facilitate mothers receiving the support they need. Health care providers and International Board Certified Lactation Consultants (IBCLCs) develop strong relationships with their patients and may be well poised to assist breastfeeding mothers with accessing services, including referral to treatment for cannabis use disorder. 26
Smoking was the most common mode of cannabis use in our sample. Second-hand smoke exposure increases infants' risk of SIDS. 13 A systematic review reported the population attributable fraction of second-hand smoke for SIDS to be between 6.7% and 43.6%. 27 Interestingly, Posis et al. 18 found that family homes in which cannabis was smoked indoors had indoor air particle concentrations at levels similar to homes in which tobacco was smoked, indicating that second-hand smoke from cannabis could also have potential SIDS risk. The impact of second-hand smoke from cannabis is also evident as children in homes where cannabis was smoked have been significantly more likely to experience adverse health events when controlling for confounders. 18
To decrease the risks of second-hand smoke, similar strategies that are recommended to mothers who smoke tobacco would be applicable: (1) do not smoke around the baby, (2) always smoke outside, (3) cover clothing and hair while smoking, and (4) wash face and chest before breastfeeding to remove smoke residual. Vaping, the second most reported mode of consumption, may result in fewer chemicals than smoked cannabis; however, it, too, is not without risks. Many vaping devices use highly processed products with high-potency forms of cannabis, and acute lung injury has been reported in some instances. 28
Other issues related to cannabis use among breastfeeding mothers include infant sleep location and maternal impairment. If mothers are using cannabis, they should not sleep with their babies, particularly if they are intoxicated.29,30 Safe-sleep strategies could include the baby in a basket or the baby near the bed in a bassinet or co-sleeper. All babies under 6 months should sleep in the parents' room to reduce the risk of SIDS 31 but not bed-share if mothers or their partners are using cannabis. In addition, when mothers are high, someone else who can safely care for the infant should be present. This is basic safety planning that needs to be frankly discussed with mothers. A particular concern is possible impaired driving while high.
Among mothers who use cannabis while breastfeeding, strategies could be implemented to decrease their infants' exposure to THC in the breast milk by timing their cannabis use to immediately follow rather than precede breastfeeding sessions. This strategy would likely be most helpful for mothers who are occasional users, where THC levels drop within 4 hours of consumption. 14
It is unclear how chronic high levels of cannabis use affect THC concentrations in breast milk. This is an area that should be explored. Regardless, among all women who are using cannabis while breastfeeding, it seems prudent to counsel women (1) to discontinue or minimize their frequency of cannabis use and (2) to time their cannabis use to avoid infant exposure to the highest THC levels through breast milk. When ceasing use of cannabis is unlikely, waiting at least 4 hours after cannabis use to breastfeed may substantially reduce cannabis exposure of the infant through breast milk. 14
Strengths/Limitations
Our study is one of the first that reports reasons for cannabis use among a large sample size of breastfeeding mothers who used cannabis, a sample of cannabis users approximately four times the size of samples reported in PRAMS data. 4 In addition, our survey explored more detailed aspects about reasons for cannabis use, allowing for close examination of health-related reasons.
Notable limitations exist in this study. First, the sampling strategy, which enlisted the assistance of organizations of mothers who used cannabis, may limit our ability to generalize results to all mothers who use cannabis. Our findings might also differ if we included mothers under age 18 or if the survey had been available in other languages, such as Spanish. In addition, we recognize that the income categories are not all inclusive, but represent the categories provided as options in the survey.
Unfortunately, information on breastfeeding duration was not collected and, thus, could not be reported. Data from PRAMS indicated that breastfeeding durations varied among mothers who used cannabis and believed it was unsafe compared to those who believed it was safe. 4 Future studies should examine breastfeeding duration among mothers who use cannabis. Finally, a challenge with studying mothers who use cannabis is that it is illegal on a federal level and in many states; thus, our IRB did not allow us to collect information on state of residence. Frequency of cannabis use may have differed based on state of residence because of legality and access issues. The illegal status of cannabis may also have caused some mothers not to participate.
A large proportion of our sample was non-Hispanic White, and there were notably no differences in cannabis use frequency by race/ethnicity. Data from national surveys4,19 have also found non-Hispanic White women to make up the highest proportion of cannabis users during pregnancy and postpartum; however, their proportions were ∼65% compared to our 79%. While we believe this to be a limitation in our data, the higher percentage of White women in our sample is consistent with previous surveys that have studied cannabis use in perinatal women. The two PRAMS studies may have pulled a slightly higher percentage of racial/ethnic minority women than our sample because they focused more on general health questions.4,19 Our study was specific to cannabis use. We believe that racial/ethnic minority women may have been more reluctant to identify themselves as using cannabis because of historical mistrust of medical research and possible fear of child removal, which is disproportionally more common among minority versus White families.
Future studies should examine how high, chronic cannabis use affects transfer of THC into breast milk. Hospital and medical practices should also examine how policies may be supportive of the mothers rather than punitive. Finally, mothers' perceptions of the safety of cannabis versus medications should be explored.
Conclusions
Despite recommendations, at least 1 in 20 mothers is using cannabis while breastfeeding. Health reasons may be a particularly important driving factor for increasing frequency of cannabis use. Maternal health problems, particularly related to anxiety and other mental health issues, should be addressed among mothers who use cannabis. Future studies should examine approaches to reduce cannabis use through safe and alternative treatments for chronic pain and mental health conditions among breastfeeding mothers. Further harm-reduction strategies should also be implemented to reduce infant exposure to cannabis and its potential detrimental consequences.
Footnotes
Acknowledgments
The authors acknowledge Allison McBrayer, MD who assisted development of the data collection instrument, and Heather Thompson, PhD, MS from Elephant Circle who served as a key informant and provided assistance with survey testing. We also acknowledge Dr. Duke Appiah, Department of Public Health, Texas Tech University Health Sciences Center, who provided guidance on statistical analyses.
Authors' Contributions
C.D.G. conceptualized the study, performed the analyses, and drafted the article. K.K.T., C.Y., and T.B. conceptualized the study, created data collection instruments, provided feedback on analyses, and reviewed and revised the article. T.W.H. conceptualized the study, provided feedback on analyses, and critically reviewed the article for important intellectual content.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.