
Abstract
Aim:
Mother's own milk (MOM) is the preferred source of neonatal nutrition. Due to various challenges, mothers are often unable to provide exclusive MOM to neonates admitted in neonatal intensive care units (NICUs) and depend on pasteurized donor human milk (PDHM). The aim of this quality improvement (QI) initiative was to enable mothers to provide MOM and consequently decrease the “PDHM dependency.”
Methods:
Neonates <32 weeks of gestation (n = 120) were included. A multidisciplinary team was formed, and a detailed root cause analysis was done to understand the cause of PDHM dependency during the observation phase (November 1 to December 15, 2019). Various evidence-based practices were planned, tested, and implemented through Plan-Do-Study-Act cycles during the intervention phase (December 16, 2019 to January 31, 2020). These were further strengthened and adopted as a unit culture during the maintenance phase (February 1 to July 31, 2020). Results from the observation and intervention phases were compared.
Results:
Within 6 weeks of QI interventions, the average proportion of MOM significantly increased from 74.4% to 93.5% (p = 0.0003), and the proportion of PDHM significantly decreased from 20.5% to 4.6% (p = 0.005). The proportion of MOM remained at 82.5% during the maintenance phase. There was a significant decrease in the number of days to reach full feeds and regain birth weight.
Conclusions:
Provision of PDHM from our newly functional milk bank led to a reduced drive to express MOM in mothers of NICU babies. Our QI project focused on various strategies to improve MOM feeding and reduce PDHM dependence.
Introduction
The benefits of mother's own milk (MOM) and its advantages in preterm neonates are well known. Prevention of prematurity-related morbidities (e.g., necrotizing enterocolitis, bronchopulmonary dysplasia, and retinopathy of prematurity), better intestinal maturity, and improved neurodevelopmental outcomes are few advantages.1–4 However, initiation and maintenance of MOM are of global concern in neonatal intensive care units (NICUs). 5 The American Academy of Pediatrics recommends pasteurized donor human milk (PDHM) as the second-best option if MOM is not available. However, pasteurization, refrigeration, and freeze–dry cycles affect the nutritional and functional properties of milk and decrease protective factors, such as immunoglobulin, probiotics, and growth factors.6–9 The lactational stage of PDHM also contributes to nutrient limitations for infants. 10
The advantages of MOM are abundantly evident in literature for both short-term and long-term neonatal outcomes, and MOM should be a preferred choice over PDHM.
After establishment of a mother's milk bank in our center in August 2019, a reduced drive to express MOM was observed in the mothers of babies in NICUs. Various reasons were cited by the mothers such as ‘baby is already on human milk,’ ‘I'm tired,’ ‘I don't have milk,’ ‘I cannot come to the hospital for expression,’ and ‘expression is painful and tiring.’ There is also a lack of interest among nursing staff and resident physicians to encourage mothers for MOM due to an easy availability of PDHM, leading to what is defined as “PDHM dependency.”
There have been several studies on PDHM dependency; however, only a few have described methods to overcome it.11,12 This quality improvement (QI) project was initiated to address the issue of increased dependence of mothers and staff on PDHM.
Aim
To improve the contribution of MOM by more than 90% in the daily consumption of human milk among preterm babies admitted in the NICU, thereby decreasing the “PDHM dependency.”
Materials and Methods
The study was conducted at a tertiary-level IIIB NICU in India from November 1, 2019 to July 31, 2020 in three phases. These were the observation phase from November 1 to December 15, 2019 (6 weeks), followed by the intervention phase from December 16, 2019 to January 31, 2020 (6 weeks) and the maintenance phase from February 1 to July 31, 2020 (6 months). The maintenance period was atypical because of the impact of coronavirus disease 2019 (COVID-19)-related lockdown. Inborn preterm neonates (<32 weeks of gestation) and all out-born neonates of similar gestation who were admitted within 24 hours of delivery were included in the study. Neonates of critically ill mothers who were not able to feed and neonates with major congenital anomalies and gastrointestinal surgeries were excluded from the study.
A multidisciplinary team was formed, including a neonatologist, two neonatology residents, two neonatal nurses, one labor room nurse, and one lactation counselor. The Institutional Ethics Committee approved the study.
During the observation phase, the multidisciplinary team collected baseline data, and a fish bone analysis was performed to understand the root cause of PDHM dependence (Fig. 1). After studying various causes related to persons, environment, materials, and procedures that led to the PDHM dependence in mothers and staff, a “Bundle” of best practices was charted as primary and secondary drivers (Fig. 2). The multidisciplinary team constantly counseled mothers on the importance of breast milk, differences between MOM and PDHM, and frequency of breast milk expression. Myths about the equivalence of MOM and PDHM were corrected.
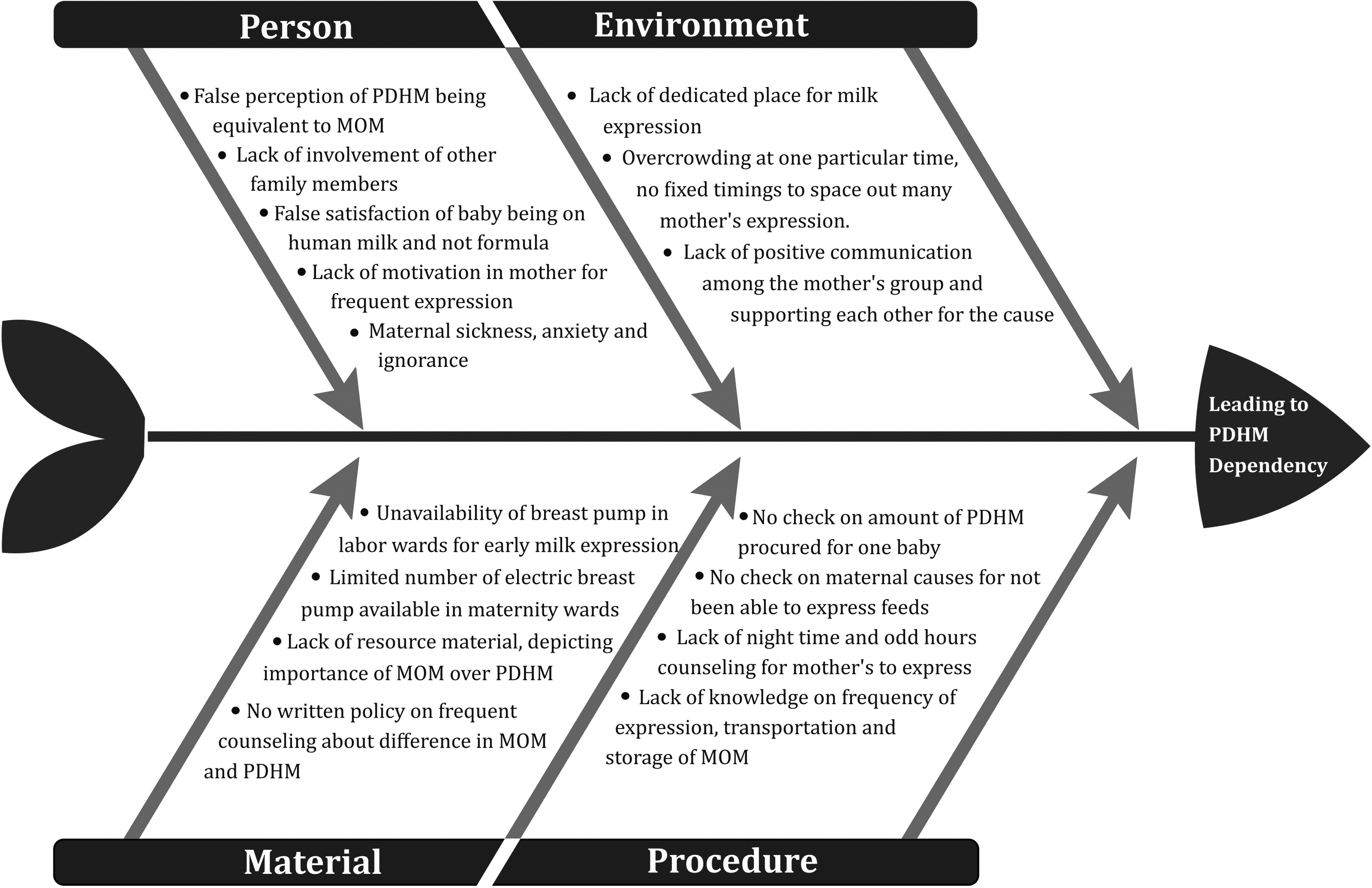
Fish bone analysis—detailed root cause analysis. FF, formula feed; MOM, mother's own milk; PDHM, pasteurized donor human milk.
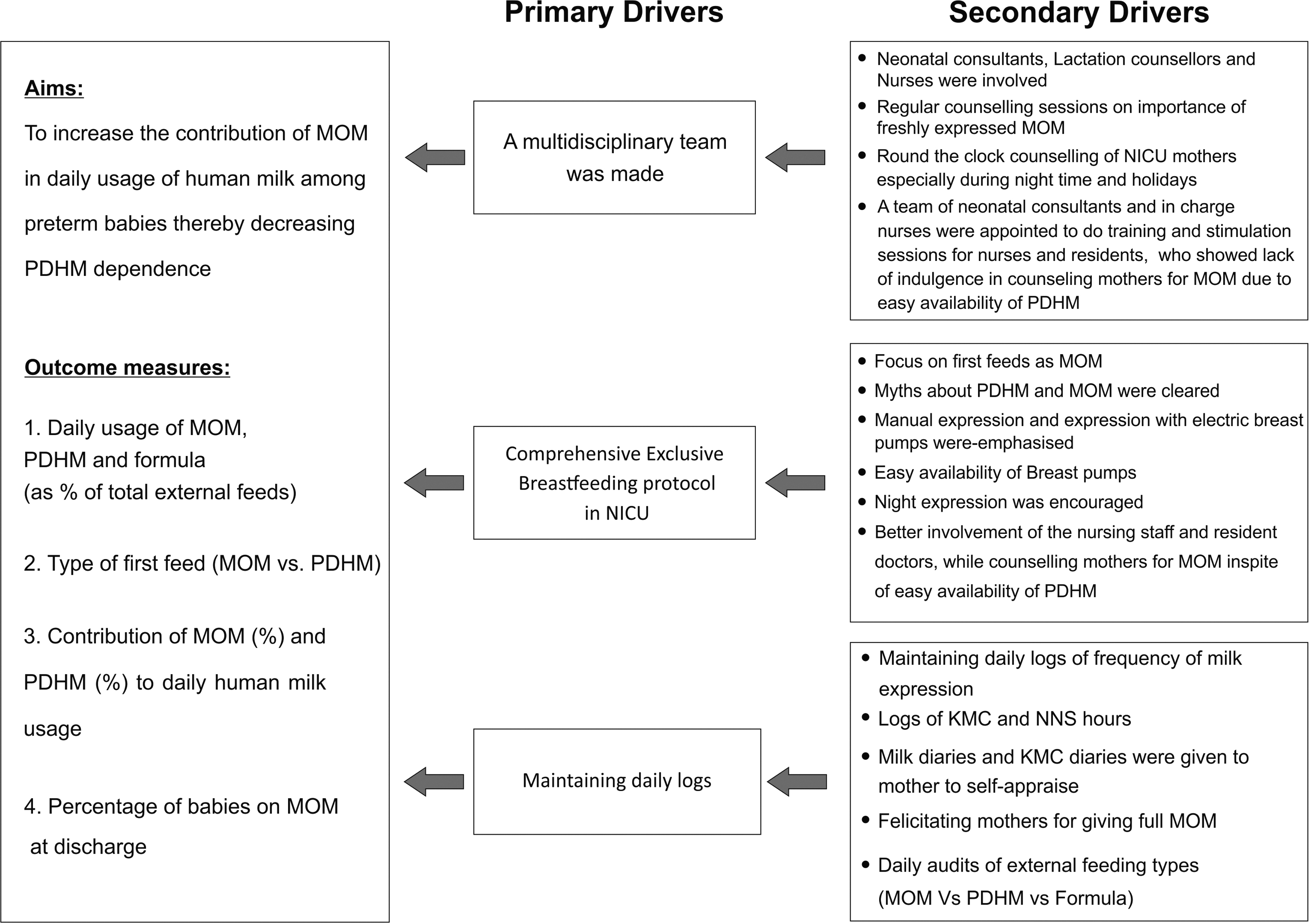
Driver diagram. KMC, Kangaroo Mother Care; NICU, neonatal intensive care unit; NNS, non-nutritive sucking.
These sessions involved senior neonatologists, neonatology residents, bedside nurses, and lactation counselors, and were conducted every day during the NICU stay (even on holidays and at nights). A comprehensive unit protocol emphasizing exclusive feeding of MOM was developed, and frequent milk expressions and night expressions were encouraged.
Family members, including the husband and grandparents on both sides, were made part of these frequent counseling sessions to extend support to the lactating preterm mother. Breast pumps (manual and hospital-grade electrical breast pumps) were made easily available. Kangaroo Mother Care (KMC) and non-nutritive sucking (NNS) were supported and encouraged. Daily logs of milk expression, milk diaries, and KMC diaries recorded the frequency and quantity of milk expression. KMC hours were recorded.
The most important step was the weekly log of the percentage of MOM versus PDHM versus formula feed (FF), which helped mothers in self-appraisal and also gave an early signal to catch up with exclusive MOM over PDHM. These regular feedbacks helped mothers in understanding the need better. A mothers' club was formed where experienced mothers from the NICU were involved in counseling the existing preterm mothers on the importance and maintenance of breastfeeding and encouraging them. The nursing staff and resident doctors who showed lack of interest in counseling mothers for MOM due to easy availability of PDHM were also motivated for better and regular involvement. These interventions together helped in changing the unit strategies and achieving outcomes.
Various practice modifications were planned through Plan-Do-Study-Act (PDSA) cycle (Fig. 3) during the intervention phase. These changes were implemented, and new evidence-based practices were tested every week and implemented through PDSA cycles (Fig. 4). Daily logs were maintained, data were averaged for every week, and run charts were displayed (Fig. 5) to provide regular feedback. The neonatal resident in the unit collected data on a daily basis. Daily intake of MOM, PDHM, and FF as respective proportions of total milk consumption and proportion of any human milk in total milk consumption were charted. The secondary outcome measures included hours of life when first feed was started, type of first feed, weight at the time of discharge, Z-score for weight, growth velocity, duration of hospital stay, time to regain birth weight, and percentage of babies on MOM at discharge. During the maintenance phase, test ideas were strengthened and adopted into the system. Data collection, monitoring, sensitization of the team members, and regular feedback to the mothers became a daily practice. Best practices like KMC and NNS and involvement of other family members were scaled up.
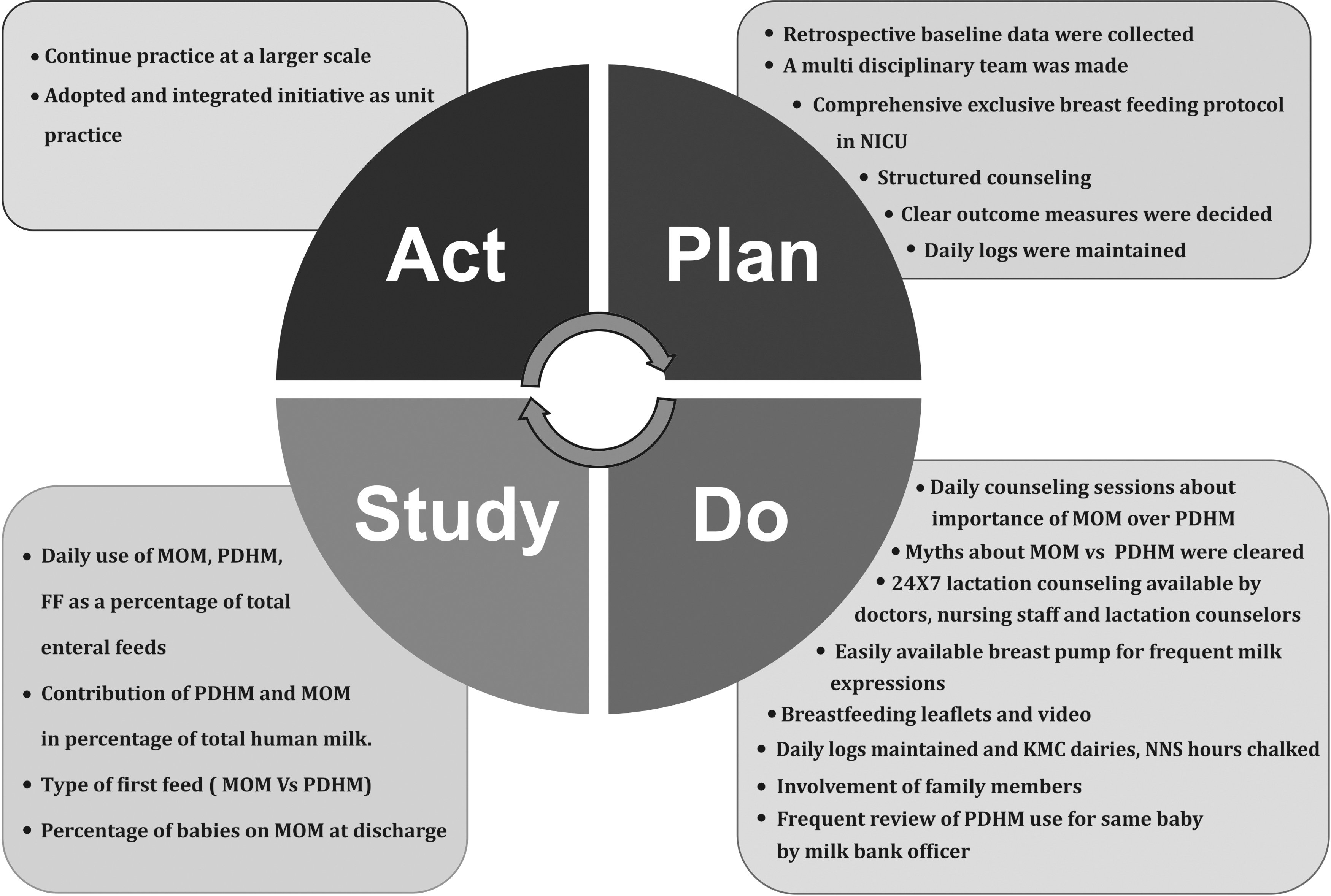
PDSA cycle. PDSA, Plan-Do-Study-Act.

Implementation of PDSA cycle.
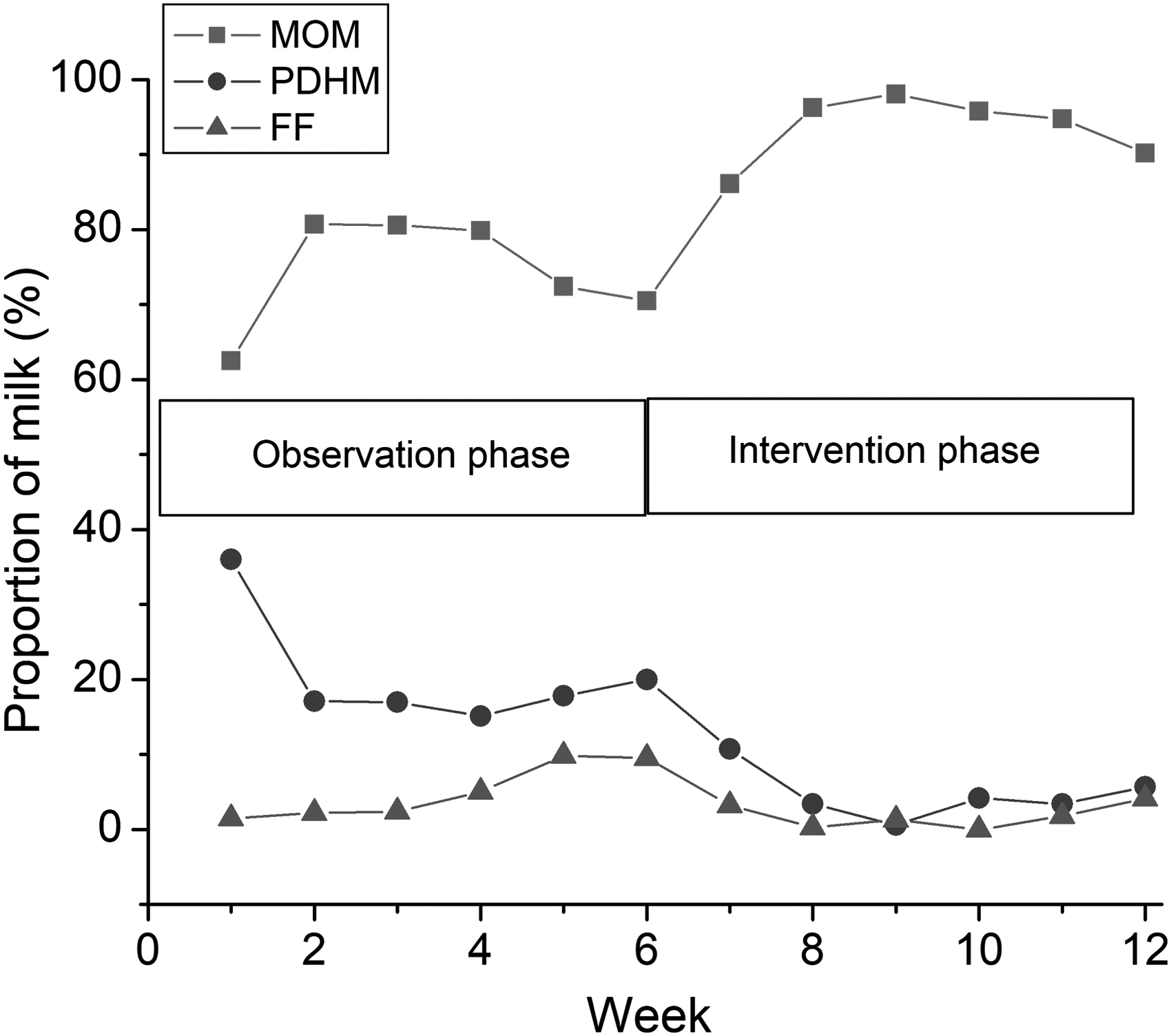
Run chart.
The statistical analysis was performed using software Origin v2019b (Origin Lab Corporation, Northampton, MA). The normality of the distribution of continuous data was assessed by Shapiro–Wilk test. Data with normal distribution were described in mean ± standard deviation and data with non-normal distribution in median and interquartile range (IQR) and compared between observation and intervention phases by t test and Mann–Whitney test, respectively. Categorical data were described in proportions and compared between observation and intervention phases by chi-square test or Fisher's exact test. Since the data on the maintenance phase were affected by COVID-19, they were not included in the analysis. A p-value of <0.05 was considered statistically significant.
Results
During the study period, a total of 155 neonates <32 weeks were admitted and 120 neonates were included in the study as per inclusion criteria. Among these 120 babies, 21 neonates were part of the observation phase, 24 babies were in the intervention phase, and 75 babies were in the maintenance phase. During the observation phase (Supplementary Table S1), average use of formula was 5.1%, and any human milk consumption was 94.9%. The proportion of MOM used was only 74.4%, and PDHM was 20.5%. Over a period of next 6 weeks (intervention phase: Supplementary Table S2), proportion of MOM increased significantly to 93.5% (p = 0.0003), and PDHM proportion decreased significantly to 4.6% (p = 0.005) of the total human milk consumption.
There was no statistically significant difference between any human milk (94.9% versus 98.3%; p = 0.09) and proportion of formula used (5.1% versus 1.1%; p = 0.09) in the observation and intervention groups, respectively. During the maintenance phase, average intake of any human milk continued to be 90.35%, with proportion of MOM, PDHM, and formula being 82.70%, 7.65%, and 9.65%, respectively.
Table 1 shows the demographic profile of neonates and it was comparable between the observation and intervention phases in terms of birth weight, gestation, and discharge weight. Hours of life when the first feed was started significantly (p = 0.002) improved from a median of 11 hours (IQR, 6–19 hours) to 5 hours (IQR, 3–7 hours). Proportion of MOM:PDHM also significantly (p = 0.02) improved from 61.9% to 92.3%.
Demographic Profile
This table compares the demographic profile of babies between observation and intervention phases.
IQR, interquartile range; MOM, mother's own milk; PDHM, pasteurized donor human milk; SD, standard deviation.
Table 2 shows the secondary outcome measures. The Z-score of discharge weight, growth velocity, duration of hospital stay, and percentage of babies on MOM at the time of discharge were comparable in both the groups. The mean days to regain birth weight was significantly (p = 0.02) lower in the intervention phase (11.9 ± 4.9 versus 15.5 ± 5.5).
Secondary Outcomes
This table compares the secondary outcomes between observation and intervention phases.
Discussion
The donor human milk has expeditiously become the second-best choice of feeding in very low–birth weight babies (VLBW <1500 g), if MOM was not available. There is evidence in literature that PDHM decreases the risk of necrotizing enterocolitis either when used alone or when used along with MOM, compared with FF.13–15 This practice change from formula to PDHM has masked the abundant benefits of exclusive MOM feeding. In fact, both milks (MOM and PDHM) are measured as “any human milk feeds” in most of the NICUs, ignoring the proportion of exclusive MOM received by the baby. In our unit, we noticed an increased consumption of PDHM after the establishment of milk bank similar to what was observed in literature.6,11 In a few cases, the effect of introduction of donor milk in NICUs has been associated with less use of MOM. 16
While a few studies have raised the concern of PDHM dependency, 12 to date, there is no study that has reported on a QI initiative to address this.
We identified the problem and performed a detailed root-cause analysis. Based on this, we developed evidence-based, locally acceptable, and relevant strategies to focus on exclusive MOM feeds and decrease use of PDHM. Various evidence-based practices to promote and sustain MOM were considered such as antenatal and postnatal counseling, provision of lactation support, educating the mother for milk expression,17,18 and early and frequent pumping of milk. 19 The role of KMC, NNS, and nursing education was reemphasized in the unit.20,21 Lactation counseling was available around the clock, and frequent telephonic reminders or messages were sent to mothers about milk expression even after discharge, similar to the practices reported in the study by Pineda et al. 21
Various PDSA cycles were conducted and tested over a period of 6 weeks. The contribution of MOM to total human milk significantly increased and was consistent during the maintenance phase.
The secondary outcomes such as MOM as type of first feed, hours of life when the first feed was started, days to regain birth weight, and percentage of babies on MOM at discharge were better when compared with our previously published QI to improve MOM. 5 During the maintenance phase, there was a decreasing trend in the usage of any human milk (MOM and PDHM), and increased use of formula was observed. This was probably due to lockdown restrictions during COVID-19 pandemic, and mothers could not visit the hospital frequently.
Human milk donations also decreased during this period, and many parents did not want to opt for MOM if they tested positive for the virus or were in contact with positive cases. There was a lack of clear guidelines in the early period of the pandemic about transmission of disease through milk, KMC, and NNS policies and protocols to visit the NICUs. Postlockdown, we educated the mothers and other family members about lack of evidence on vertical transmission and transmission of virus through breast milk and reinculcated best practices in the unit following safety protocols.
The strengths of the study were early identification of the problem of PDHM dependence, adopting and strengthening practices by closely observing results of QI over the next 6 months, and making the entire process a regular practice in the unit.
Second, no additional monetary support was required, and the existing staff and residents took additional responsibility to promote exclusive MOM feeds to the neonates. The nursing staff and lactation counselors underwent intensive training sessions and participated with better competence (Supplementary Table S3). They were in close communication with parents attending to concerns of KMC, NNS, and frequent milk expressions. Third, this is one of the very few studies that has demonstrated increased dependence on PDHM due to easy availability and how systemic implementation of QI can decrease the PDHM dependence in the unit. We acknowledge that the sample size and the PDSA cycle duration were small and short, respectively, but these findings can inform similar NICUs of the best practices to decrease the “PDHM dependence.”
Although the team worked rigorously during the whole phase and regular counseling and involvement of the mothers became a routine practice in the unit, some challenges were encountered during the pandemic with a significant decrease in the availability of nursing and other support staff, and the anxiety of mothers affected milk production during the initial few weeks of the maintenance phase that subsequently improved.
Conclusion
The donor human milk has become the second-best choice in neonatal units where MOM is not available and PDHM is easily available. Both types of milk are commonly used as “human milk feeding.” However, PDHM cannot be a replacement for MOM, and it is important to observe and improve the proportion of MOM received by neonates. Our study shows that investing resources in addressing lactation barriers with evidence-based practices helps in improving continuous supply of exclusive MOM, in spite of easy availability of PDHM. There is a need for more such QI initiatives in future to address this issue.
Footnotes
Acknowledgment
The authors would like to thank Dr. Kurt O Gilliland PhD, Cell Biology and Physiology, University of North Carolina, Chapel Hill, NC for the article review.
Disclosure Statement
None of the authors has any proprietary interests or conflicts of interest related to this submission.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.