
Abstract
Objective:
Milk expression is the key step of milk production in mothers of preterm infants. Our hospital has started an electrical breast pump loaning program to improve human milk feeding rate in our patients. This study was aimed to assess the beneficial effect of the loaning program.
Materials and Methods:
This was an interrupted time-series study. In addition to general information, mothers in the intervention period received electrical breast pump before discharge. Maternal milk volume was recorded for 28 days, and 24-hour-feeding record and recall were used to determine breastfeeding rate at discharge and 6 months postpartum, respectively.
Results:
There were 40 mothers, 20 mothers in each group, who participated in this study. Maternal milk volume in the control group was 169.3 + 152.4, 329.5 + 241.6, 547.4 + 390.8, and 704.2 + 439.6 mL/day in first, second, third, and fourth week, respectively. Milk volume in the intervention group was 308.5 + 269.6, 454.1 + 281, 544.9 + 282.2, and 531.9 + 282.2 mL/day in first, second, third, and fourth week. Average frequency of milk expression was higher in the intervention group [5.15 (1) and 6.01 (1.49) times per day, p-value 0.04]. There were one (5%) and four (20%) infants in the control and intervention groups who were exclusively breastfed at discharge. At 6 months, eight (40%) infants from each group were still breastfed.
Conclusion:
Mothers in the pump loaning program had expressed milk more frequently. Even though maternal milk volume difference did not reach statistical significance, the intervention group had higher milk volume in the first 2 weeks postpartum. There was no difference in terms of feeding type both at discharge and 6 months postpartum.
Introduction
Preterm infants face many challenges during the early life period. Compared with term infants, preterm infants are at higher risk of mortality and morbidity. Some of these challenges result from immaturity itself, such as respiratory distress syndrome or necrotizing enterocolitis (NEC). Some are the consequences from a combination of immaturity and treatment complications such as bronchopulmonary dysplasia and retinopathy of prematurity, or cerebral palsy. 1 Moreover, long-term health and social outcomes such as IQ, deficit in executive function, and behavioral and emotional outcomes are challenges faced by preterm infants. 2
Human milk has been recognized as the best medicine in neonatology. It provides uncomparable nutritive factors, growth factors, and immunologic factors. Preterm infants who received a higher dose of human milk have a lower rate of late onset sepsis and NEC.3,4 The beneficial effects of human milk feeding in terms of hospitalization rate, mental development index, and psychomotor development index score continued beyond infancy. 5 However, the establishment and maintenance of a milk supply in mothers of these preterm infants are not simple. Based on the 10 steps for promoting and protecting breastfeeding for vulnerable infants, 6 mothers need to initiate milk expression within 6–12 hours after birth, 8–12 times per day with a hospital-grade electrical breast pump.
In Thailand, good quality electrical breast pumps are quite expensive and might not be affordable for some families. From a previous study of our hospital, 50–60% of mothers of sick neonates started milk expression within 4 hours after labor. Nearly 70% of neonates admitted in the neonatal unit received human milk for >50% of total feedings during the hospital stay. 7 Continuation of breastfeeding after discharge remains the major goal of supporting breastfeeding in all neonates, including sick neonates. However, in our hospital, only 34% of previously sick neonates continue exclusive breastfeeding at 6 months. 8
With the intention to improve the breastfeeding rate in our preterm infants, our hospital has set up an electrical breast pump loaning program for mothers of preterm infants <32 weeks or birth weight <1,500 g, to support the establishment and maintenance of milk supply in mothers of preterm infants. This research focused on the effect of the electrical breast pump loaning program on maternal milk volume and breastfeeding rate at hospital discharge and 6 months postpartum.
Materials and Methods
This study was an interrupted time-series study. It was done in a university hospital with level III NICU during November 2017–April 2019. Mothers (N = 40) of preterm infants <32 weeks of gestation or birth weight <1,500 g were enrolled if their child was admitted in the hospital within 72 hours of life. Exclusion criteria were contraindication to human milk feeding such as HIV infection or inborn error of metabolism. Mothers were terminated from the study if their child died or they decided to stop milk expression before 28 days after labor. In the study period, we did not have donor milk yet, so all human milk is mother's own milk.
The study period was divided into two periods. During the early postpartum period, before maternal discharge, all mothers were advised to use hospital-grade pumps combined with hand expression to initiate lactation six to eight times per day. Before discharge, mothers in the first period were informed about the importance of human milk to preterm infants, and also how to express and collect milk for preterm babies. Mothers in this period were free to choose to express milk by hand or her own electrical breast pump. In the second period, mothers were similarly informed about the importance of human milk feeding, as with mothers in the first period. However, in the second period, mothers were offered a high-quality electrical breast pump with a double pump collecting system (Spectra S1® and Pump-in-Style Medela®) to use after discharge. All pumps in the loaning project were donated. Most were second hand but all pumps had been checked and were working before giving them to the mothers. Every pump was cleaned by our staff, all pump accessories such as breast shield, tubing, and connector were replaced with new accessories.
Instructions regarding how to express milk either by hand or by electrical pump were given by a lactation nurse. After discharge, mothers were given a milk record chart to record milk volume production and frequency of milk expression every day. Telephone visits were done every 2 months until mothers stopped milk expression or 6 months postpartum. Data collection included baseline mother and infant characteristics, timing of first milk expression after labor, frequency of milk expression, and volume of milk production for each week. In the intervention group, mothers were asked to report any nipple pain in each week and the satisfaction of using the electrical pump. The infant's clinical outcomes such as death, NEC, hospital-acquired infection, time to full enteral feeding, length of hospital stay, and feeding type at discharge and 6 months postpartum were also recorded. This protocol was approved by the ethics committee of Thammasat University MTU-EC-PE-1-065/61.
Outcome measures
Milk volume production
Mothers were given 20 mL syringes to record milk volume obtained each time of expression.
Feeding type at discharge
We used 24-hour milk intake record from the patient chart. Infants were categorized into four groups:
Exclusive human milk feeding: Infants received only human milk. Mainly human milk feeding: Infants received human milk for more than half of the total feed. Mainly formula feeding: Infants received human milk for less than half of the total feeds. Exclusive formula feeding: Infants who had not received any human milk.
Feeding type at 6 months postpartum
We used a telephone follow-up for 24-hour recall of feeding type. Infants were categorized into four groups as per feeding type at discharge.
Statistical analysis
The sample size calculation was primarily based on milk volume production (from Slusher et al. 9 ). At least 20 mothers, 10 in each group, were required to achieve power of 90%, and an α level of 0.05. Information sheets were given to all participants and written informed consent was obtained from all. Independent data were analyzed using Student's t-test and Wilcoxon rank-sum test. Maternal milk volume production each week was analyzed using repeated measure analysis.
Result
There were 40 mothers who participated in the study. Thirty women (70%) were primigravida. Nearly half of the infants were male (N = 19, 47.5%). The time of the first milk expression ranged from 3 to 120 hours after birth [median (IQR); 4.15 (3.65, 6)]. There was one woman in the control group who initiated milk expression at the 120th hour due to maternal illness. In the control group, there were eight mothers (40%) who used a small personal electrical pump of varying brands, whereas all mothers in the intervention group were loaned high-quality electrical pumps from our loan program. All mothers had completed follow-up until 6 months or cessation of milk expression of breastfeeding. There was no difference in mothers' and infants' baseline characteristics, as given in Table 1. The frequency of milk expression was significantly higher in the intervention group [6.01 (1.49) versus 5.14 (1.00), p-value = 0.040]. Median (IQR) of maternal milk production at day of life 14th was 240 mL (135, 550) in the control group and 403 mL (237.5, 649) in the intervention group (p-value = 0.11).
Patient Characteristics and Clinical Outcomes
Data are described in median (IQR), Wilcoxon rank-sum test was used.
NEC, necrotizing enterocolitis.
Maternal milk volume production in each week is shown in Figure 1. The average of daily milk volume production of mothers in the control group was 169.3 ± 152.4, 329.5 ± 241.6, 547.4 ± 390.8, and 704.2 ± 439.6 mL in first, second, third, and fourth weeks, respectively. For the intervention group, the average daily milk production was 308.5 ± 269.6, 454.1 ± 281, 544.9 ± 282.2, and 531.9 ± 282.2 mL, respectively. As shown in Figure 1, mothers in the intervention group had slightly higher milk volume production in the second week, however, no statistical difference was detected.
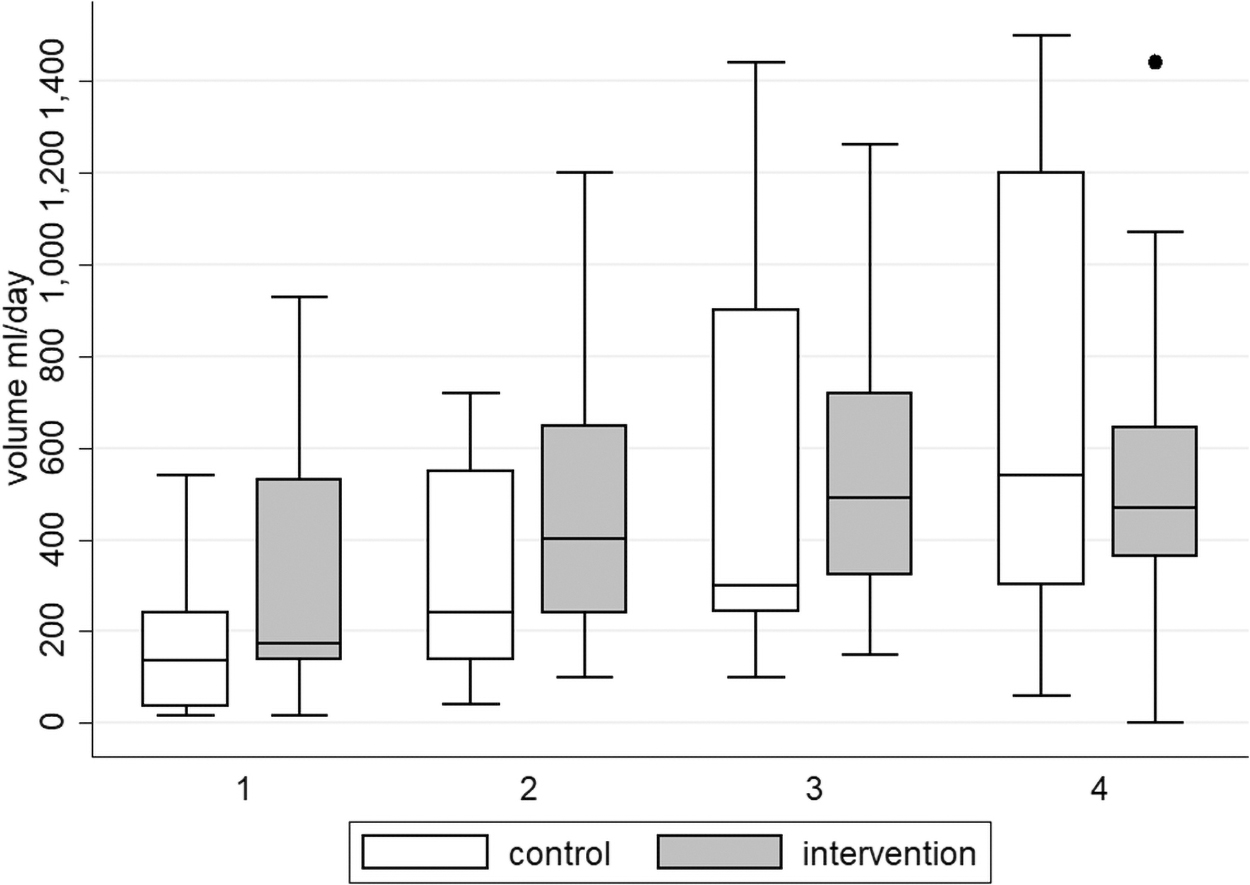
Maternal milk volume production in each week. Box plots show the median and interquartile range (IQR; 25th to 75th percentiles) of average maternal milk volume production (mL/day) in each week during the first 4 weeks postpartum. Whisker bars represent 1.5 IQR beyond each box.
The between-groups test from longitudinal analysis using a conditional model after controlling for frequency of breast milk expression indicated that there was no difference in milk volume production change in the intervention and control groups (p-value = 0.169), as well as between mothers who use pump or hand expression (p-value = 0.93), as shown in Figures 2 and 3.
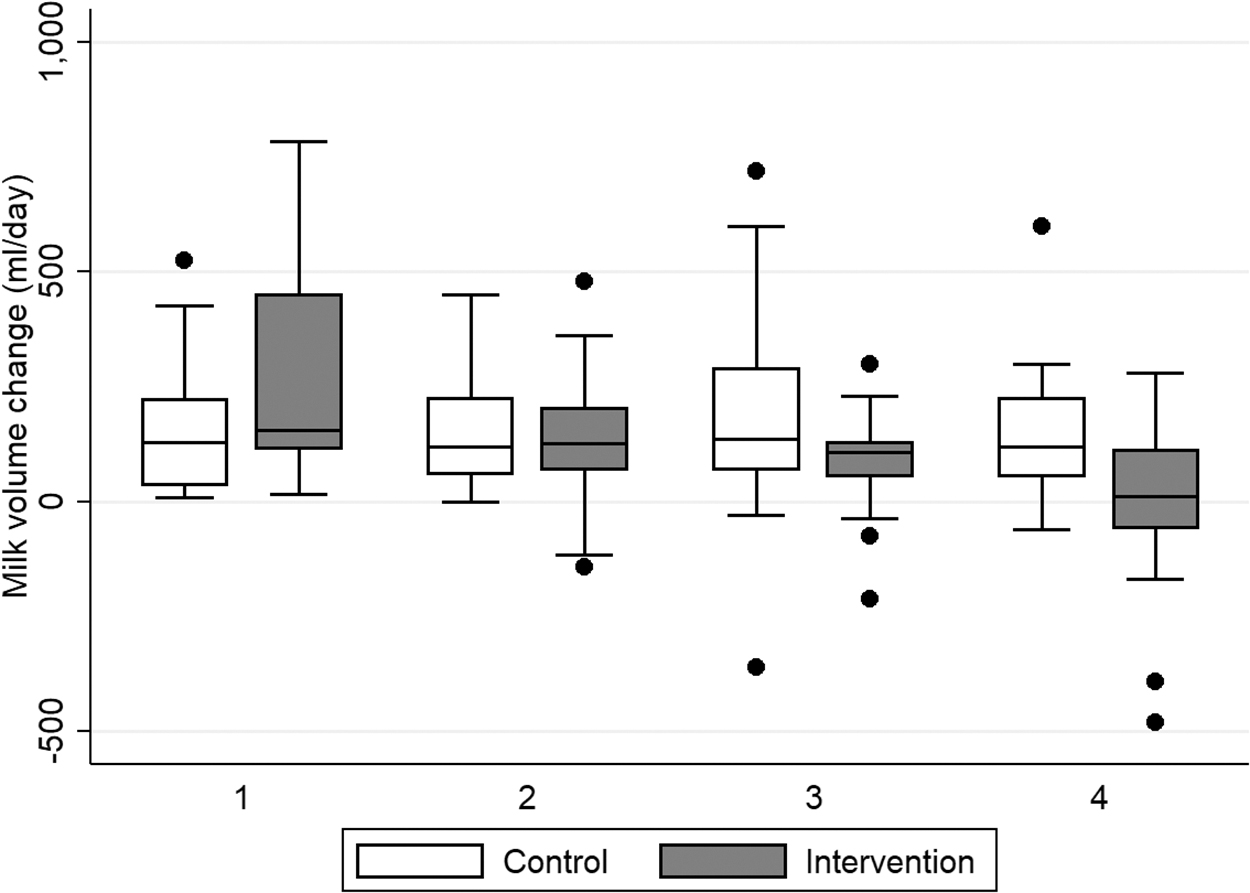
Maternal milk volume change in each week classified by the intervention group. Box plots show the median and interquartile range (IQR; 25th to 75th percentiles) of maternal milk volume change (mL/day) after adjusting for frequency of milk expression in each week during the first 4 weeks postpartum. Whisker bars represent 1.5 IQR beyond each box.
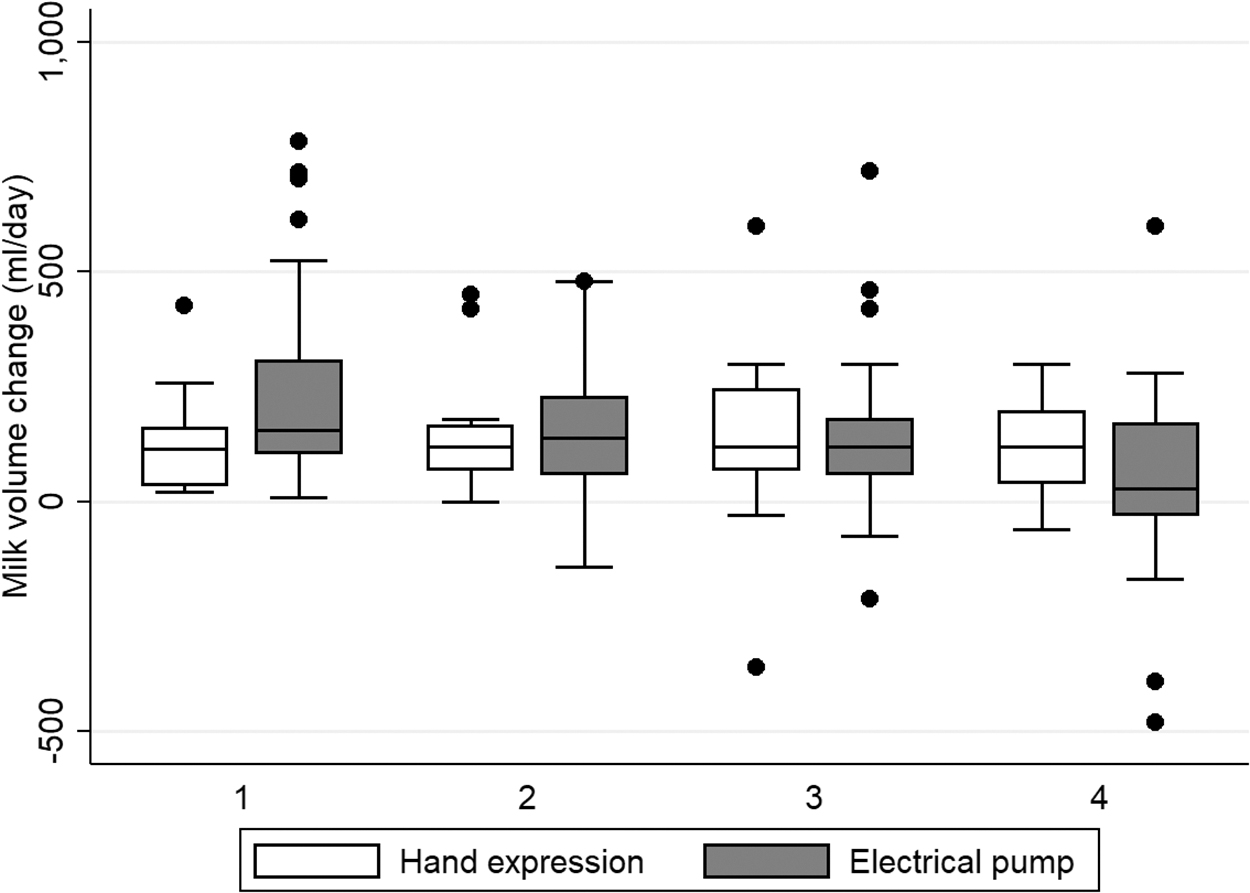
Maternal milk volume change in each week classified by type of expression. Box plots show the median and interquartile range (IQR; 25th to 75th percentiles) of maternal milk volume change (mL/day) after adjusting for frequency of milk expression in each week during the first 4 weeks postpartum. Whisker bars represent 1.5 IQR beyond each box.
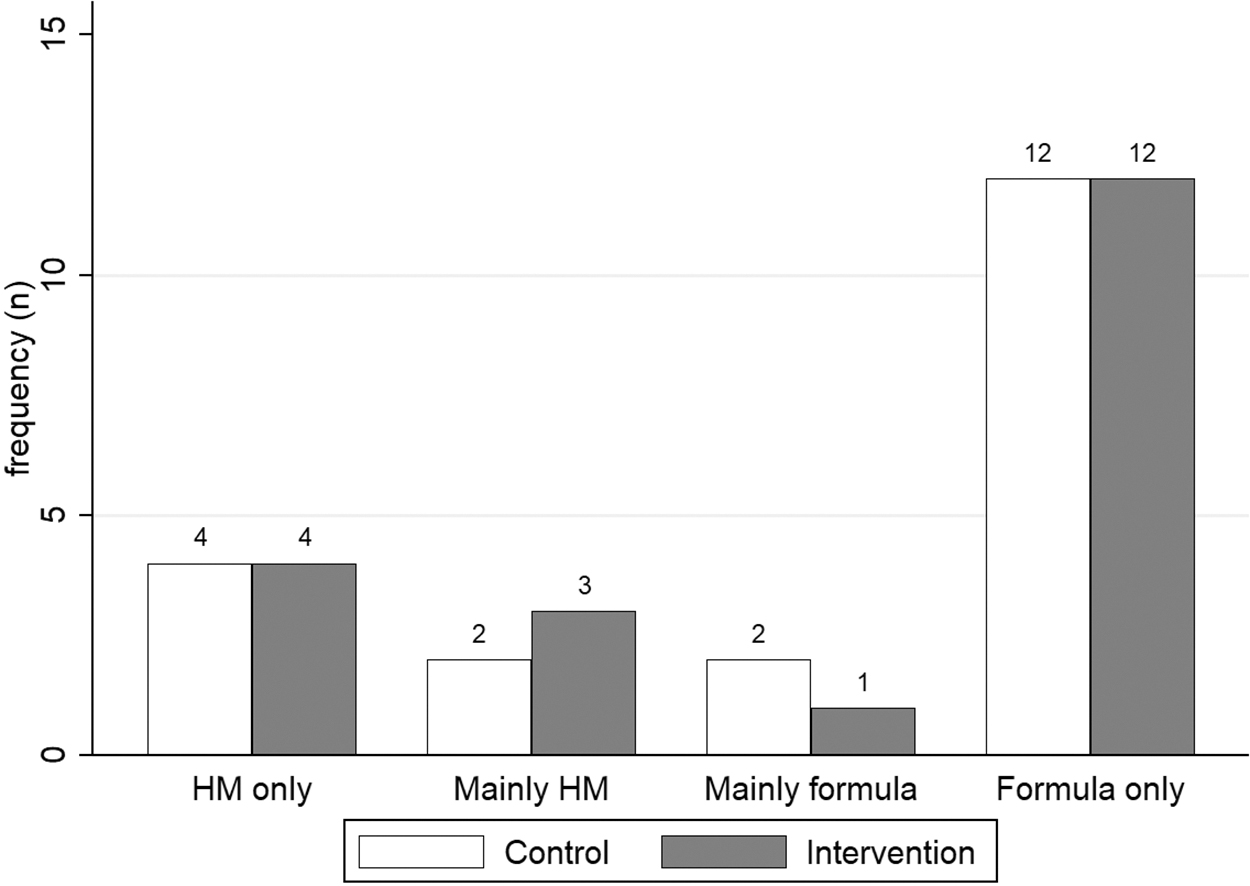
The proportion of infants who received any human milk feeding was not different at discharge and sixth month postpartum. At discharge, there were 8 infants (40%) in the control group who received more human milk than formula than 14 (70%) infants in the intervention group (p-value = 0.111). Regarding the feeding type at the sixth month, there were six (30%) and seven (35%) infants in the control and intervention groups who received mainly human milk, respectively (p-value = 1.0). Mean (SD) of breastfeeding duration was 3.96 (1.99) months and 3.58 (2.05) months in the control and intervention groups, respectively, (p-value = 0.496) Figures 4 and 5.
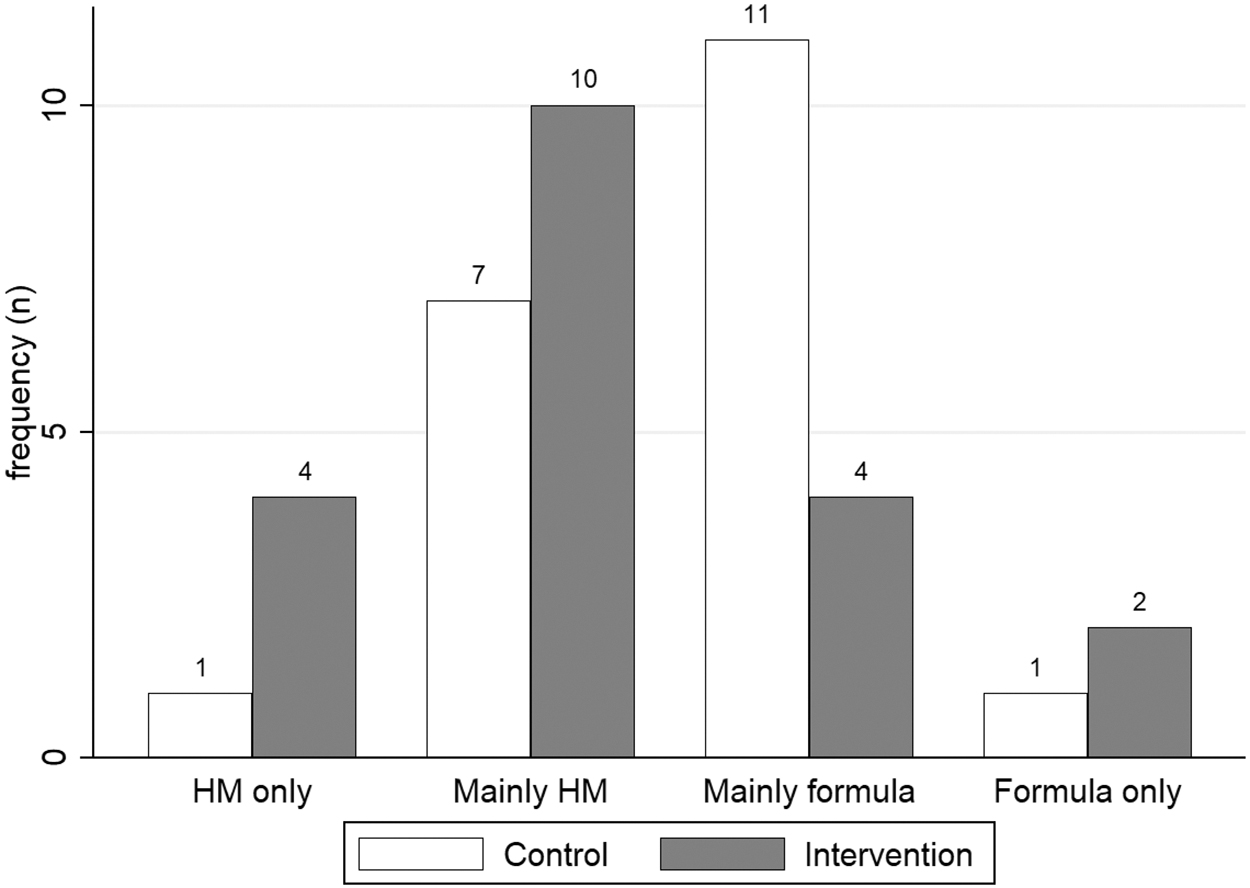
Infant feeding type at discharge. Bar graphs show number of infants categorized by feeding type at discharge.
Infant feeding type at sixth month. Bar graphs show number of infants categorized by feeding type at sixth month.
For clinical outcomes, the rate of late-onset sepsis, NEC, length of hospital stay, and hospital costs were similar in both groups. Very few mothers in the intervention group reported nipple pain in the first week and no mothers reported nipple pain in the third or fourth week. Most of them were satisfied with the electrical pump. Unfortunately, we had no data for maternal nipple pain and satisfactory milk expression in the control group.
Discussion
To provide mother's own milk to very preterm infants, initiation and maintenance of milk supply are the keystones of the process. Based on “Ten steps for promoting and protecting breastfeeding for vulnerable infants,” milk initiation should begin within 4 hours after labor, at least 8–12 times per day. 6 The methods of milk expression have been discussed widely. Most studies revealed a higher milk volume obtained from large electrical pumps compared with hand expression.9,10 Issues other than milk volume were inconsistent regarding maternal satisfaction and quality of milk. 11 Hospital-grade breast pumps seem to be the preferred method of expression to maintain milk supply until discharge. This study was designed to assess the beneficial effects of the electrical breast pump loaning program, not the difference between hand expression and electrical pump. Although there were some mothers who used their own breast pump, all pumps in the control group were not hospital-grade breast pumps. Therefore, we analyzed the data based on group assignment. Our study failed to demonstrate any significant beneficial effect of loaning high-quality breast pumps to improve milk production and rate of human milk feeding through hospital discharge, but maternal milk volume was slightly higher in the second week in the intervention group. In repeated measure analysis after adjusting for frequency of expression, we were unable to demonstrate any difference in the control and intervention groups. Findings were similar in mothers who used an electrical pump compared with mothers who used hand expression (Figs. 2 and 3). Most mothers in both groups expressed milk less than eight times a day, which might not be adequate for maintaining lactation in mothers of vulnerable infants. This might be the reason that our mother's milk production was not different. Based on the physiology of lactation, stage II lactogenesis depends on prolactin level and prolactin was released in response to nipple stimulation. Once lactation was established, the maintenance of the milk supply relied on milk removal through the regulation of feedback inhibitory of lactation (FIL) and intramammary pressure. 12 Inadequate milk removal or long intervals of milk expression resulted in inadequate stimulation of prolactin secretion, increased intramammary pressure and inadequate removal of FIL led to decreased milk production.
Predictors of adequate milk supply until discharge are dual pumping system, milk volume >500 mL at 10th day after labor, 13 timing of milk expression initiation, and pumping frequency. 14 In this study, most mothers had initiated pumping within 6 hours after birth, which is acceptable. However, milk volume production at 14th day was <500 mL in both groups. As mentioned previously, milk volume production in the second week is the critical milestone for successful maintenance of milk supply in vulnerable infants. In our study, most mothers produced milk <500 mL/day at 14th day, and most of them continued human milk feeding until discharge. There was a slightly higher percentage of infants who received mainly human milk at discharge in the intervention group, but it did not reach statistical significance. However, compared with our previous study, 8 the rate of infants who were predominantly fed with human milk improved from 56.3% to 70% in the intervention group.
There were few limitations in this study. First, our sample size was based on the difference of milk volume from hand expression and electrical breast pump, therefore, it might not be sufficient to detect any clinical difference such as NEC or hospital stay. Second, because of financial issues, we used two brands of donated pumps. For future study, we would recommend firsthand hospital-grade breast pumps instead of donated pump. Also, the control group should limit only hand expression or manual pumps only. Last, based on discharge feeding type, if the sample size increases, the effect of the pump loaning program might be more evident.
From our previous study, the rate of breastfeeding for >6 months remained stable. 8 Even though exclusive breastfeeding until 6 months is the major goal for infant feeding policy, in Thailand there are obstacles to continue breastfeeding to 6 months postpartum such as short maternity leave, and separation of mother–infant dyads. Therefore, the pump loaning program alone was not powerful enough by itself to increase breastfeeding rates at 6 months.
Conclusion
An electrical breast pump loaning program alone cannot improve maternal milk supply without adequate frequency of milk expression. Therefore, we suggest a breast pump loaning program should be bundled with other strategies to improve the frequency of expression.
Footnotes
Acknowledgments
The authors thank Dr. Prapasri Kulalert, Department of Clinical Epidemiology, and Ms. Sam Ormond, from the Clinical Research Center, Faculty of Medicine, Thammasat University, for research analysis and English editorial assistance, respectively.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Faculty of Medicine, Thammasat University.