
Abstract
Background:
Previous research has noted an association between breastfeeding and a reduced risk of postpartum depression (PPD). This article provides a systematic review and meta-analysis on the possible association of the type and degree of breastfeeding and PPD.
Methods:
A systematic literature search in English was conducted by using PubMed, Google Scholar, Scopus, Web of Science, and Cochrane Library Databases from their start dates until January 2021. Outcome estimates were pooled by odds ratios (ORs) or standardized mean differences.
Result:
Women who did not exclusively breastfeed had 89% higher odds of PPD (OR = 1.89, 95% confidence interval [CI]: 1.50–2.39). Included studies used different cutoff points for the diagnosis of PPD. Therefore, PPD in nonexclusive breastfeeding mothers was more in studies using the cutoff point 9/10 (OR 1.97, 95% CI 1.46–2.64) as symptoms of depression than those using the cutoff point 12 (OR 1.78, 95% CI 1.21–2.61). Some studies reported PPD based on means and the others reported it based on OR. Accordingly, nonexclusive breastfeeding mothers had higher odds of PPD in studies calculating the effect size based on means (OR 1.62, 95% CI 1.19–2.19) and OR (OR 2.36, 95% CI 1.65–3.39) than in other studies.
Conclusion:
This review showed that exclusive breastfeeding is associated with a reduced risk for PPD.
Introduction
Postpartum depression (PPD) is the most common psychiatric complication of childbirth that develops in 10–20% of women and it can have devastating consequences for women, their kids, and families. 1 Criteria for diagnosing depression include the presence of at least five symptoms of depressed mood, decreased interest or enjoyment in activities, weight loss or gain without a specific program, lack of sleep or oversleeping, feeling tired, feeling worthless, decreased concentration, and suicidal thoughts. 2 Hormonal, biochemical, psychological, social, and environmental factors are involved in the progression of depression.3,4 Unfortunately, PPD is generally under-recognized and undertreated. 5
PPD causes a poor relationship between the mother and the baby, unfavorable feelings about the baby, and, ultimately, a poor attachment bond between the mother and the baby.6,7 It is mentioned in the literature that the lactogenic hormones, including oxytocin and prolactin, are involved in PPD. 8
Oxytocin has undeniable effects on decreasing maternal anxiety and the establishment of an emotional relationship between mother and infant and mothers’ eye and skin contact with the baby. 9 Further, lower oxytocin levels in pregnancy can impair emotional adaptation to motherhood, which is a primary risk factor for PPD development and, subsequently, affects the quality of maternal behavior. 10 Released oxytocin in response to breastfeeding causes milk ejection, and it induces physiological changes. 11 These changes promote psychological adaptation to prepare women for motherhood. 12
As a result, breastfeeding behaviors can significantly change mothers’ physiological and psychological states. Some studies have indicated the association between breastfeeding and PPD.13–15 For instance, Dennis (2007), in a population-based study on 594 postpartum participants, indicated that mothers with an Edinburgh Postnatal Depression Score >12 at 1 week postpartum were significantly more likely to discontinue breastfeeding at 4 and 8 weeks. 14 In another study, Khalifa et al. showed that exclusive breastfeeding was associated with an 80% decrease in odds of PPD. 16 Considering several studies on the association between breastfeeding and PPD, and given that a systematic review attempts to collate all empirical evidence that fits pre-specified eligibility criteria to answer a specific research question, 17 this study aimed at assessing the association between the type of breastfeeding and PPD.
Materials and Methods
This systematic review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO ID: 251079) before performing the review and is publicly available. It was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. 18 The PRISMA checklist was used to ensure the inclusion of relevant data.
Search strategy
Studies on relationships between breastfeeding and postnatal depression were found by using precise and comprehensive search methods. Also, published English-language articles and abstracts were identified in Google Scholar, Scopus, Web of Science, Pub Med, and Cochrane Library Databases from their start dates until January 2021. In addition, some mesh and non-mesh keywords and their combinations were used during the literature search as follows:
“Post Natal Depression,” “Post-Natal Depression,” “Post-Partum Depression,” Post-Partum Depression,” “Postnatal Depression,” “Puerperal Depression,” “Postpartum,” “Breast Feeding,” “Breast Milk Expression,” “Breast Feeding,” “Exclusive Breastfeeding,” “Breastfeeding,” “Feeding,” “Exclusive Breast Feeding,” “Lactation,” “Human Milk,” and “Breast Milk.”
The search was carried out by using quotation marks to find exact terms, parentheses to build a search with a combination of terms, and asterisks to search all words derived from each of the mentioned keywords.
EndNote software (reference manager software, version X9.3.3) was used to export all retrieved articles. Duplicate articles were deleted, and the remaining articles underwent an initial evaluation. Two reviewers (M.Z. and M.M.) separately read the titles and abstracts of the articles to find those relevant to the subject. A third reviewer (R.A.) was consulted in case of uncertainty or disagreements between the two reviewers. This review was performed with no restriction for publication time or language.
The process demonstrated in Figure 1 explains how the final number of articles included in the review and articles at each stage were reached after following various steps.

PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Inclusion and exclusion criteria
The inclusion criteria were defined with an adaptation of the PICOS approach 19 as follows: (1) studies assessing the effects of exclusive breastfeeding on depression outcome compared with nonexclusive or no breastfeeding, (2) studies using the EPDS questionnaire to assess depression, (3) studies with point estimates comparing the effects of exclusive breastfeeding with nonexclusive or no breastfeeding on the depression outcome (odds ratio [OR], risk ratio, or data to allow calculation of these values), and (4) studies with sample sizes >25 (for statistic calculations). Studies were excluded if they (1) did not assess breastfeeding, (2) were not published in English, and (3) were not available in full-text version or had insufficient data in their abstracts. Finally, nine full-text articles were read for eligibility screening (Fig. 1).
Data extraction and study quality assessment
For data extraction, one of the authors (R.A.) extracted the detailed characteristics of each of the articles by using a pre-prepared list and recorded the information as follows: sample size, age (mean or range), publication year, country, first author's last name, duration (week), exclusive breastfeeding and nonexclusive or no breastfeeding group sample, and point estimates comparing breastfeeding with non-breastfeeding on the depression outcome (Table 1).
Baseline Features of Studies Included in Systematic Review and the Meta-Analysis of Breastfeeding on Postpartum Depression
CI, confidence interval; EPDS, edinburgh postnatal depression scale; OR, odds ratio; SD, standard deviation.
A standard international checklist, that is, the Strengthening the Reporting of Observational Studies in Epidemiology checklist, was used for assessing the quality of the studies. 20
Statistical analysis
Point estimates and 95% confidence intervals (CIs) of all the included studies were calculated to determine the breastfeeding effect on postnatal depression. The primary effect size for meta-analyses was considered OR. Therefore, any effect size other than ORs was transformed to ORs whenever possible. In addition, standardized mean differences were changed to OR by using the following formula:
21
Forest plots were used to express the results of each study and the heterogeneity among the studies. For pooling the effect of breastfeeding on postnatal depression, it was assumed that the included studies were random samples from the populations under study, and a random-effect model was employed. The heterogeneity among the studies was examined by using 25%, 50%, and 75% values corresponding to low, moderate, and high degrees of heterogeneity, respectively. 22
The source of heterogeneity was explored by using subgroup analysis based on the EPDS cutoff point for assessing depression (9–10 versus ≥12) and the effect size (mean versus OR). Statistical analyses were implemented by using Stata version 16.0 (Stata Corp. 2019. Stata Statistical Software: Release 16; Stata Corp LLC, College Station, TX). p < 0.05 was indicative of the level of statistical significance.
Bias and sensitivity test
The across-study bias (publication bias) was examined by using funnel plots. In addition, the statistical significance was assessed by Egger's regression asymmetry test. Finally, to test the robustness of a pooled estimate, each study's effect was evaluated on the pooled effect by excluding single studies sequentially. A study was deemed not to influence the pooled estimate if the estimate without it was within the 95% confidence limits of the overall effect.
Results
Out of the 1,514 studies from the literature review, nine were eligible to be included in the systematic review and meta-analysis according to the inclusion criteria,14,16,23–29 as shown in Figure 1.
Our meta-analysis included 2,408 participants in a duration from 1 week to 14 months after childbirth. The studies were published between 2006 and 2019.
Findings on the association between the type of breastfeeding and PPD are reported in Figure 2. The summary estimate from the nine studies for non-breastfeeding versus breastfeeding on PPD was 1.89 (95% CI, 1.50–2.39; p < 0.001). Women who did not exclusively breastfeed had 89% higher odds of PPD than those with exclusive breastfeeding. Thus, there was zero heterogeneity. However, studies with poor estimates could mask the presence of real heterogeneity, resulting in a heterogeneity estimate of zero. Therefore, it would be a mistake to interpret an estimate of zero as meaning that effect sizes are consistent unless it is justified by CIs that exclude large values. 21 The CI was between 0% and 68% and, thus, there was moderate heterogeneity.

Forest plot diagram of systematic reviews and meta-analysis studies showing the effect of non-breastfeeding versus ever breastfeeding on postpartum depression.
The pooled estimates by potential risk factors are presented in Figure 3. We found that PPD was almost twice (OR 1.97, 95% CI 1.46–2.64) and 78% (OR 1.78, 95% CI 1.21–2.61) greater in nonexclusive breastfeeding mothers than in their exclusive breastfeeding counterparts in studies using the cutoff point 9/10 and 12 as symptoms of depression, respectively (Fig. 3A). Moreover, in studies with the effect size calculated based on means, PPD was 62% (OR 1.62, 95% CI 1.19–2.19) greater in nonexclusive breastfeeding mothers than in those with exclusive breastfeeding. Also, PPD was 2.36 times (OR 2.36, 95% CI 1.65–3.39) greater in nonexclusive breastfeeding mothers than in exclusive breastfeeding mothers in studies, with the effect size calculated based on OR (Fig. 3B).

Subgroup analysis for the effect of type of breastfeeding on PPD based on
The funnel plots showed no publication bias (Fig. 4), which was also confirmed by Egger's test (the bias coefficients b = 1.53; z = 1.62, p = 0.106), revealing that publication bias might not have a significant influence on the overall prevalence estimate.
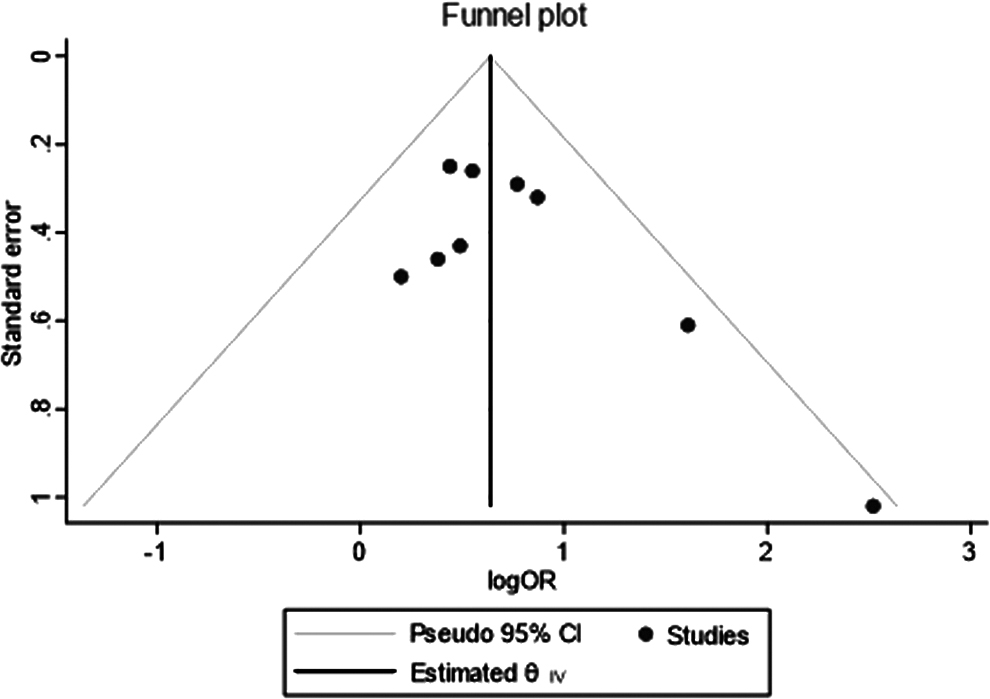
The funnel plot.
Sensitivity tests
The sensitivity tests indicated that all single-study omitted estimates lay within the 95% CI of the respective overall effect. This suggested that no single study substantially influenced the pooled effect. The stability of such results validated the rationality and reliability of our analysis.
Discussion
To our knowledge, this is the first systematic review and meta-analysis of the association between the type of breastfeeding and PPD. The present meta-analysis results indicated the higher odds of PPD in nonexclusive breastfeeding women compared with exclusive breastfeeding women. Moreover, those with nonexclusive breastfeeding had an 89% increased risk of developing PPD.
The mechanism underpinning these findings may be attributed to the role of the two most important hormones, that is, prolactin and oxytocin, associated with lactation. Prolactin is an essential hormone for breastfeeding that is involved in initiating and inducing maternal behavior. 30 In addition, the maternal serum level of oxytocin predicts mother–infant attachment by reducing anxiety and regulating responses to stressful stimuli during pregnancy and the postpartum period.31,32
A lower level of oxytocin was also measured in mothers with depression compared with the other mothers. 33 The result of a study demonstrated a reverse dose-dependent relationship between breastfeeding frequency and stress level. 34 Another explanation for this finding is that most women experience feelings of joy and pleasure during the breastfeeding process. 35
These findings are also consistent with those of previous studies that indicate an association between breastfeeding process problems and maternal mood.33,36 The findings are also similar to those of previous research, suggesting that mothers suffering from PPD were significantly more likely to experience less confidence in their breastfeeding ability. 37 Similarly, the findings are in line with those of a previous systematic review reporting that the exclusivity of breastfeeding was less likely to occur in mothers with postpartum depressive symptoms. 38 Therefore, the interaction between breastfeeding and PPD appears bidirectional.
Despite the lack of heterogeneity among the studies, further analysis was made to find a possible source of true heterogeneity. Due to the difference in diagnostic cutting points of the PPD scale, a subgroup analysis was performed to assess the impact of this variable on the outcome. The analysis demonstrated that PPD was more significant in mothers with nonexclusive breastfeeding than in exclusive breastfeeding mothers in studies using the cutoff point 9/10 and 12. This showed that even mild depression is associated with exclusive breastfeeding.
Generally, according to the findings of this study and other studies on the psychological consequences of exclusive breastfeeding, the World Health Organization's recommendation about exclusive breastfeeding in at least the first 6 months should be emphasized. 39 However, it is notable that the prevalence of exclusive breastfeeding remains low worldwide and it does not meet the WHO Global Nutrition Target. 40
Several limitations must be considered when interpreting these findings. First, a small number of studies was included in this analysis. In addition, this meta-analysis was based on cross-sectional studies; therefore, we cannot confirm the causality of the observed association.
A major strength of this meta-analysis was the absence of publication bias, as demonstrated by funnel plot symmetry, which indicates the high generalizability of results.
However, further studies are still required regarding the psychological consequences of breastfeeding. Further, according to the results of this study about the relationship between exclusive breastfeeding and maternal depression, further studies using longitudinal or experimental designs will determine this causal relationship.
Conclusions
Generally, these findings suggested that exclusive breastfeeding is associated with a reduced risk for PPD. Therefore, since PPD can disrupt parenting behaviors and result in long-term negative consequences on maternal and child health, establishing health services and politics that promote exclusive breastfeeding may help reduce the incidence of this disorder.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.