
Abstract
Background:
The World Health Organization recommends exclusive breastfeeding for ≥6 months, but many mothers are unable to meet this goal. A major reason why mothers undergo early, unplanned breastfeeding cessation is perceived inadequate of milk supply (PIMS). We hypothesized that defining genetic polymorphisms associated with PIMS could aid early identification of at-risk mothers, providing an opportunity for targeted lactation support.
Materials and Methods:
This prospective observational cohort study followed 221 breastfeeding mothers for 12 months, collecting medical, demographic, and breastfeeding characteristics. Eighteen mammary secretory genes were assessed for single-nucleotide polymorphisms in 88 women (45 with PIMS and 43 with perceived adequate milk supply [PAMS]), matched by age/race/parity. Hierarchical regressions were used to assess the ability of genotype to aid PIMS prediction.
Results:
Mothers with PIMS exclusively breastfed for a shorter period (7 ± 12 weeks; p = 0.001) and reported lower milk production (17.6 ± 13.3 oz/day; p = 0.001), and their infants displayed reduced weight-for-length Z-score gains (0.74 ± 1.4; p = 0.038) relative to mothers with PAMS (22 ± 19 weeks; 27.03 ± 12.2 oz/day; 1.4 ± 1.5). Maternal genotype for the rs2271714 variant within milk fat globule EGF and factor V/VIII domain containing gene (MFGE8) was associated with PIMS status (p = 0.009, adjusted p = 0.09, likelihood ratio = 9.33) and duration of exclusive breastfeeding (p = 0.009, adjusted p = 0.09, χ2 = 9.39). Addition of MFGE8 genotype to a model employing maternal characteristics (age, parity, previous breast-feeding duration, body mass index, education, and depression status) significantly increased predictive accuracy for PIMS status (p = 0.001; χ2 = 13.5; area under the curve = 0.813 versus 0.725).
Conclusions:
Genotyping one lactogenic gene aided identification of mothers at risk for PIMS. If validated in a larger cohort, such an approach could be used to identify mothers who may benefit from increased lactation support.
Introduction
Maternal breast milk is considered the optimal form of infant nutrition, providing health benefits to both mother and child. 1 The American Academy of Pediatrics and the American College of Obstetricians and Gynecologists recommend exclusive breastfeeding for the first 6 months, and continued breastfeeding through the first 12 months after delivery. 2 However, many women struggle to meet these recommendations. 3 Although 83% of new mothers initiate breastfeeding, only 57% are still breastfeeding at 6 months, and only 35% breastfeed until 12 months. 3
Socioeconomic and environmental factors account for a portion of breastfeeding cessation, but difficulties with milk supply are also a major contributing factor. A survey of 245 breastfeeding mothers revealed that the most common reasons for formula introduction were as follows: (1) mother's perception of father's attitude, (2) uncertainty regarding milk supply, and (3) return to work. 4 Similarly, a survey of 418 first-time mothers found that 92% were having problems breastfeeding 3 days after birth, with 40% reporting insufficient milk supply. 5 Among these women, 47% fed their newborn formula in the first 2 months, and 21% stopped breastfeeding entirely. 5
Maternal genetics contribute to the yield and composition of breast milk. 6 A study of breast milk samples from 772 mothers identified significant associations between maternal single-nucleotide polymorphisms (SNPs) in the fatty acid desaturase (FADS) gene cluster and breast milk fatty acid concentrations. 6 SNPs in FADS and fatty acid elongase (ELOVL) have also been associated with child cognitive outcomes (presumably due to the importance of fat intake on brain myelination). 7 Other studies have tied maternal genetics to the breast milk micronutrient profiles. For example, SNPs in serine-/arginine-rich SC35-like splicing factor (SLC30) have been associated with breast milk zinc content.8,9
Although extensive research has interrogated the mechanisms through which maternal genetics impact the macronutrient and micronutrient composition of breast milk, few studies have explored the relationship between maternal genotype and breast milk production. 10 Surprisingly, the majority of scientific literature regarding genetics of milk production focuses on bovine.11,12
Since “increasing the number of infants who are exclusively breastfed through six months” is one of five key goals for the Heath Resources and Services Administration's Maternal & Child Health Bureau, 13 defining the impact of human genetics on breast milk production is a crucial biologic question. The ability to use genetic profiles to prospectively identify women at risk for low milk volumes could facilitate early, targeted lactation support, preventing poor infant weight gain and early breastfeeding cessation.
The purpose of this study was to interrogate a panel of 18 genes that are highly expressed in mammary tissue and associated with secretory function (Table 1) 11 and identify maternal polymorphisms associated with inadequate milk production. Previous studies in mammals have described associations between polymorphisms in these genes and milk production characteristics, but to our knowledge, no study has examined these genes in breastfeeding women.
Candidate Genes Expressed in Mammary Tissue and Involved in Secretory Function
SNPs, single-nucleotide polymorphisms; UTR, untranslated region.
We posited that polymorphisms in a subset of the 18 genes would be associated with early, unplanned introduction of formula due to perceived inadequate milk supply (PIMS). Furthermore, we hypothesized that assessment of genotype (alongside medical and demographic factors previously associated with inadequate milk supply and/or early breastfeeding cessation) would accurately identify women at risk for PIMS. These hypotheses were tested through a prospective longitudinal cohort study of breastfeeding mothers.
Materials and Methods
Institutional Review Board approval
This study was reviewed and approved by the Penn State Institutional Review Board (STUDY00008657). All participants provided written informed consent.
Participants
This prospective longitudinal cohort study involved a convenience sample of 221 women, 19–42 years of age. Eligible participants included mothers of full-term, singleton infants (37–42 weeks gestation), who planned to breastfeed at least 6 months. Exclusion criteria included the following: maternal morbidities that could affect ability to breastfeed (e.g., cancer, drug addiction, and HIV), plan for infant adoption, presence of neonatal condition that could significantly affect a newborn's ability to feed (e.g., cleft lip/palate, metabolic disease, and prolonged neonatal intensive care unit admission >7 days), or plan to seek primary pediatric care outside our academic medical center. Participants were enrolled within 7 days of delivery at the newborn nursery or the outpatient pediatrics clinic. Enrollment began on October 18, 2018, and ceased on July 30, 2020.
Following enrollment, cheek swabs and medical/demographic information were collected from each mother, and mothers completed longitudinal follow-up surveys at 1, 4, 6, and 12 months after delivery. Participants were dichotomized into two groups (PIMS; or perceived adequate milk supply [PAMS]) as follows: as part of the infant feeding practices (IFP) survey, 14 mothers were asked, “Have you had to supplement your child's diet with formula?”
Participants who indicated formula had been introduced were asked, “Which of the following reasons best describes why you chose to introduce formula into your child's diet: a) Decreased or low breast milk production; b) My child showed signs of an allergy from breastfeeding; c) I chose to introduce formula for personal reasons (e.g., work, daycare, time restraints); and d) Other.” Mothers who indicated that formula was introduced due to decreased or low breast milk production were designated as PIMS (n = 52).
Seven of these mothers were ultimately excluded from the PIMS group because their infant displayed significant weight gain (change in weight-for-length Z-score >2.5) during the first month after delivery, indicating ample milk supply. Finally, the 45 women with PIMS were matched at the group level by age, race, and parity with 43 PAMS mothers who either maintained exclusive breastfeeding throughout the duration of the study or reported formula introduction for reasons other than “decreased or low breast milk production” (Fig. 1).

Consort diagram for participant enrollment, exclusion, and group determination. Research staff screened 2,487 mothers for eligibility, and approached eligible mothers for enrollment. There were 221 mothers who consented to participate (61.5%), of whom 192 completed the study (86.8%). Over the study period, 52 mothers reported introduction of formula due to decreased or low breast milk production, 70 mothers reported formula introduction for other reasons, and 80 reported exclusive breastfeeding. Among mothers who reported decreased or low breast milk production, seven were excluded from the PIMS group due to significant infant weight gain (weight-for-length Z-score change >2.5) between birth and 1 month postdelivery. The 45 mothers with PIMS were compared against 43 mothers with PAMS selected to match age, race, and parity at the group level. PAMS, perceived adequate milk supply; PIMS, perceived inadequate milk supply.
Measures
Participant characteristics were collected through electronic surveys administered by research staff at enrollment. When possible, survey responses were confirmed through review of the electronic medical record.
For all participants, the following medical and demographic characteristics were collected: age (years), race (White, Black, Asian, biracial, and other), ethnicity (Hispanic or non-Hispanic), marital status (married, single, unmarried and living together, divorced, or separated), health insurance (Medicaid, private, and other), parity (nulliparous, primiparous, and multiparous), duration of previous breastfeeding (>4, 2–4, 1–2 months, never breastfed), maternal prepregnancy body mass index (BMI; kg/m2), educational level (postgraduate degree, college degree, incomplete college degree, high school degree, and incomplete high school degree), tobacco status (never smoked, past smoker, and current smoker), and maternal depression (presence/absence of depression).
Mothers' self-reported current medications and supplements were compared against a database of medications known to impact breast milk production 15 (i.e., levothyroxine, levetiracetam, doxylamine, albuterol, and cetirizine). Presence of milk-suppressing medications was determined. Of note, no women reported the use of galactagogue supplements.
Infant feeding characteristics were collected through electronic administration of the modified IFP, completed by mothers 1, 4, 6, and 12 months after delivery. Results of longitudinal IFP survey responses were used to estimate the following: (1) duration of exclusive breastfeeding (defined as the period of time for which an infant received breast milk as their sole milk source) and (2) volume of milk produced in a 24-hour period, at both 1 and 4 months (defined by maternal report of estimated feeding volumes). Milk production (oz/day) was approximated based on maternal report of pumping volumes (oz/pumping session) and IFP (feeds/day). For mothers who did not use a breast pump, missing data regarding milk production volumes (n = 26/190 data points; 13.6%) were imputed using median reported milk volumes for the entire cohort at each respective time point (1 and 4 months).
For mothers who reported breastfeeding cessation (or failed to provide a breast milk sample due to PIMS) at 1 or 4 months (n = 25), a milk production volume of 0 oz/day was assigned. Given that self-reported milk production can vary widely in accuracy, 16 an upper threshold of milk production (48.1 oz/day) was applied in nine cases, based on the study by Kent et al. 17 Infant weight (kg) and length (cm) were abstracted from the medical record at birth and 1 month postdelivery. For each infant, weight-for-length Z-score was determined at each time point using standardized curves from the World Health Organization, and the change in Z-score from birth to 1 month was calculated.
Sample collection and processing
A maternal saliva sample was collected at enrollment by applying a DNA stabilizing swab to the buccal surface for 10–20 seconds as per manufacturer's instructions (DNA Genotek, Ottowa, Canada). Samples were stored at −80°C. DNA was extracted using an Illumina DNA Prep Kit (Illumina, San Diego, CA), and libraries were prepared by polymerase chain reaction with a custom Ampliseq Panel (Illumina) as per manufacturer's instructions. The panel provided 99.54% coverage across all 18 coding targets with 25 base-pair exon padding (Table 1).
SNP analysis
The processed libraries were assessed for size distribution and concentration using the BioAnalyzer High Sensitivity DNA Kit (Agilent Technologies). Pooled libraries were diluted to 2 nM in EB buffer (Qiagen) and then denatured using the Illumina protocol. The denatured libraries were diluted to 10 pM by prechilled hybridization buffer and loaded onto an Illumina MiSeq v3 flow cell (Illumina) for 150 cycles using a single-read protocol according to the manufacturer's instructions. De-multiplexed sequencing reads were generated using Illumina BaseSpace.
Alignment of amplicon reads against the human reference genome (hg19) and the variant calling was performed using the DNA amplicon analysis module in the Local Run Manager software (Illumina). VCFtools 18 was used to filter the VCF file for missing data (called below 50% across all individuals), genotype depth (<3 reads), locus quality score (a minimum quality score of 30), and minor allele frequency (minor allele count <3). Individuals with more than 50% missing data (n = 1) were excluded from down-stream analysis. Major and minor alleles were assigned using default parameters of Germline Variant Caller from the Illumina DNA amplicon analysis module (Illumina) based upon dbSNP allele status within the global population.
Statistical analysis
Medical and demographic characteristics were compared between PIMS and PAMS groups using a Welch's t test or a chi-square test. A chi-square test was used to compare genotype frequency between PIMS and PAMS groups for each missense SNP detected. A Kruskal-Wallis analysis of variance (KW-ANOVA) was used to compare duration of exclusive breastfeeding between genotypes for each missense SNP. KW-ANOVA was also used to determine if mean milk production (oz/day) differed between genotypes for each missense SNP (at both 1 and 4 months). Benjamini Hochberg multiple testing correction was applied to all p-values, and Cohen's d, likelihood ratios, or χ 2 values were reported, as appropriate. Finally, hierarchical logistic regression was used to assess the potential of maternal SNP testing to enhance prediction of PIMS.
An initial model employing maternal traits (age, parity, and previous breastfeeding duration), was compared against a second model, which added modifiable maternal characteristics (medication use, education level, depression status, and prepregnancy BMI), and a third model, which combined maternal traits and medical characteristics with genotype status (for a single missense SNP displaying relationships with PIMS/PAMS status and duration of exclusive breastfeeding).
The ability of each model to account for between-groups variance (measured by McFadden's R-squared) was reported, and significant gains across additive models (p < 0.05) were determined. Discriminative accuracy of the most predictive model (for anticipating PIMS) was visualized on a receiver operator characteristic curve. Tenfold cross-validated area under the curve (AUC), sensitivity, and specificity were reported.
Results
Participants
Participating mothers were on average 29 (±4) years of age, with a mean BMI of 27 (±6) kg/m2 (Table 2). The majority of mothers were white (66/88; 75%), married (73/88; 77%), were multiparous (41/88; 47%), never used tobacco (71/88; 81%), and had obtained a college or postgraduate degree (61/88; 69%). Relatively few had a history of depression (15/88; 17%), none lacked medical insurance (0/88; 0%), and approximately half had never previously breastfed (40/88; 45%). Self-reported depression was more common (χ 2 = 6.03; p = 0.014) among mothers with PIMS (12/45; 27%), compared to those with PAMS (3/43; 7%). There were no significant differences between mothers with PIMS (n = 45) and mothers with PAMS (n = 43) in age, race, ethnicity, marital status, parity, tobacco use, education, insurance status, or previous breastfeeding experience.
Participant Medical and Demographic Characteristics
p < 0.05. p-Values were determined by Welch's t test (non-normally distributed) or Student's t test (normally distributed).
BMI, body mass index; SD, standard deviation.
Milk production and infant weight trajectory
Mothers with PIMS had shorter duration of exclusive breastfeeding (7 ± 12 weeks) than mothers with PAMS (22 ± 19; p = 0.001; Cohen's d = 1.015; Fig. 2A). One month after delivery, mothers with PIMS reported lower volumes of milk production (17.6 ± 13.3 oz/day) than mothers with PAMS (27.0 ± 12.2 oz/day; p = 0.001; Cohen's d = 0.734; Fig. 2B). Four months after delivery, mothers with PIMS continued to report lower volumes of milk production (16.0 ± 14.1 oz/day) than mothers with PAMS (27.3 ± 14.9 oz/day; p < 0.001; Cohen's d = 0.848; Fig. 2C). Infants born to mothers with PIMS had a smaller average increase in weight-for-length Z-score between birth and 1 month (0.74 ± 1.4) than infants born to mothers with PAMS (1.4 ± 1.5; p = 0.038; Cohen's d = 0.388; Fig. 2D).
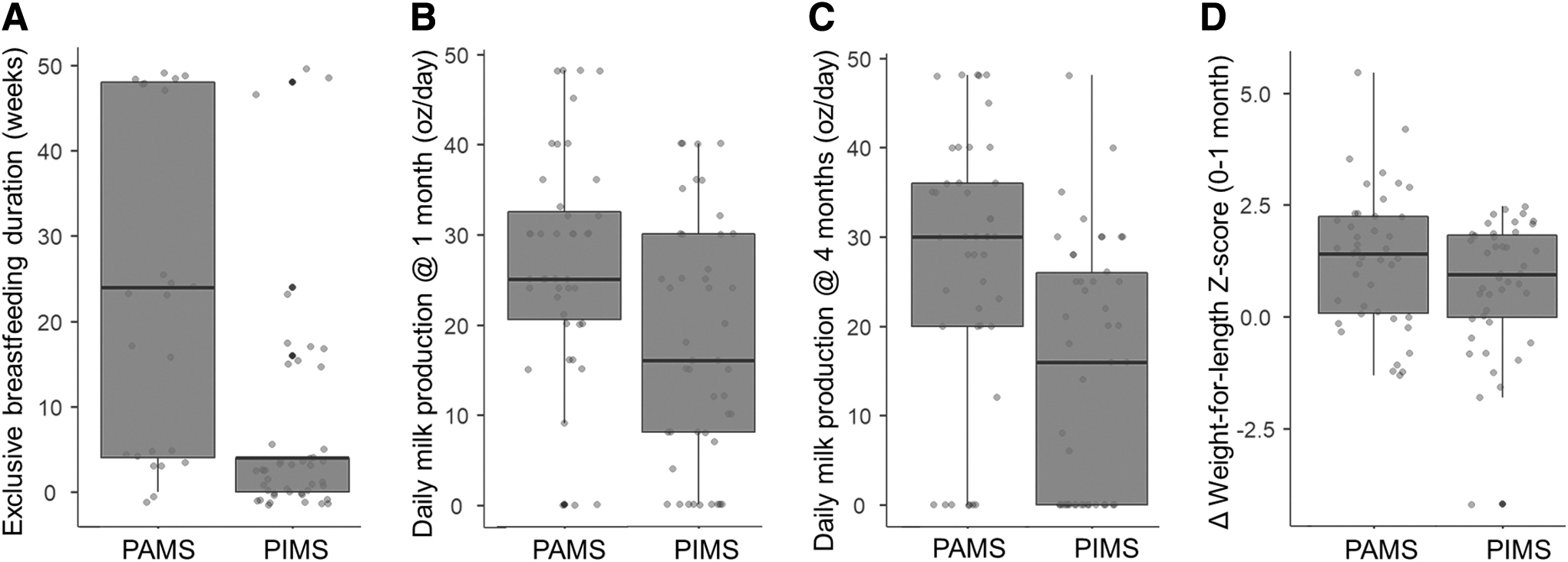
Mothers with PIMS displayed shorter duration of exclusive breastfeeding, lower volumes of daily milk production, and infants with reduced weight gain. The whisker box plots depict the milk production characteristics for mothers with PIMS and mothers with PAMS. Duration of exclusive breastfeeding
Frequency of SNPs
Among the 18 candidate genes, 72 SNPs were identified (Table 1). There were 10 missense SNPs, 9 synonymous SNPs, 52 intron SNPs, and 1 SNP within the 3′ untranslated region (Supplementary Table S1). The gene with the largest number of SNPs was ATPase plasma membrane calcium transporting 2 (ATP2B2; 19/72 SNPs; 26%). No SNP was identified in 8 of the 18 candidate genes. All downstream analyses were focused on the 10 missense SNPs.
Relationship of SNPs with perceived milk supply, duration of exclusive breastfeeding, and volume of milk production
The rs2271714 variant within the milk fat globule EGF and factor V/VIII domain containing gene (MFGE8) displayed a nominal association with PIMS status (p = 0.009, adjusted p = 0.09, χ 2 = 8.14, likelihood ratio = 9.33; Fig. 3A). Homozygosity for the major allele was observed in 93% of mothers with PAMS (40/43) compared with 76% of mothers with PIMS (34/45) (Supplementary Table S1). The rs2271714 variant within MFGE8 was also associated with duration of exclusive breastfeeding (p = 0.009, adjusted p = 0.09, χ 2 = 9.39). Homozygosity for the major allele at rs2271714 was associated with a longer duration of exclusive breastfeeding (13.8 ± 16 weeks), compared with the heterozygous variant (4.7 ± 14 weeks; Fig. 3B). None of the 10 missense SNPs was associated with volume of milk production at 1 or 4 months postdelivery.

Heterozygosity for the rs2271714 variant within MFGE8 is more common in mothers with PIMS, and is associated with shorter duration of exclusive breastfeeding. The whisker box plots depict the genotype frequencies (11, 12, and 22) for the rs2271714 variant within the MFGE8
Predictive utility of maternal genotype and medical/demographic factors
A logistic regression model employing maternal traits (age, parity, and previous breastfeeding duration) did not significantly account for the variance between PIMS and PAMS groups (p = 0.59; χ 2 = 7.4; R2 = 0.060). Neither age (p = 0.52; χ 2 = 0.47), parity (p = 0.44; χ 2 = 3.70), or previous breastfeeding duration (p = 0.38; χ 2 = 4.18) were individually significant. Addition of modifiable maternal characteristics (BMI, education level, and depression status) did not significantly improve the model (p = 0.16; χ 2 = 7.3), accounting for an additional 6.42% of the variance between groups (p = 0.362; χ 2 = 15.24; R2 = 0.125). In this model, only depression status displayed significance (p = 0.006; χ 2 = 7.62).
Addition of a single SNP (rs2271714, MFGE8) to maternal traits and modifiable maternal characteristics resulted in a model that accounted for a significant amount of additional variance (11.06%) between PIMS and PAMS groups (p = 0.001; χ 2 = 13.5), and accurately differentiated PIMS status (p = 0.026; χ 2 = 28.74; R2 = 0.2356). Predictive utility of each model was compared on a receiver operator characteristic curve (Fig. 4). The predictive model utilizing rs2271714 (MFGE8), maternal traits, and maternal modifiable characteristics displayed greater accuracy (AUC = 0.813, sensitivity = 0.78, and specificity = 0.70) than a model using maternal traits and maternal modifiable characteristics (AUC = 0.725, sensitivity = 0.69, and specificity = 0.65), or maternal traits alone (AUC = 0.637, sensitivity = 0.64, and specificity = 0.54).

A logistic regression model employing maternal genotype for MFGE8 enhances detection of mothers at risk for PIMS. The receiver operating characteristic curves display sensitivity and specificity for hierarchical models employing maternal traits (age, parity, and previous breastfeeding duration)
Discussion
In this study, we survey part of the genetic landscape in 45 women with PIMS. The results show that missense mutations in lactogenic genes are relatively uncommon. An SNP in the MFGE8 gene (rs2271714) may be associated with the risk of PIMS. Within our cohort, a polymorphism at this locus was associated with a sevenfold increase in PIMS risk, and heterozygotes displayed significantly shorter durations of exclusive breastfeeding (4.7 weeks). When assessed in combination with maternal characteristics, detection of the rs2271714 variant significantly improved ability to predict PIMS. Although PIMS is a subjective measure of milk supply, in this cohort, PIMS was associated with shorter duration of exclusive breastfeeding, lower volumes of daily milk production at 1 and 4 months postdelivery, and reduced infant weight-for-length z-score trajectory.
Clinical implications
Identifying risk for PIMS at the outset of breastfeeding could provide opportunities for early, targeted lactation support and aid efforts to achieve exclusive breastfeeding through 6 months. Current assessment for PIMS risk is largely guided by parental reports of infant satiety or perceived breast milk production. 19 Although several predictive tools have been developed for clinical use, these rely solely on maternal characteristics. Furthermore, few assessments specifically differentiate PIMS from other causes of early breastfeeding cessation (such as maternal choice), few demonstrate predictive validity, and many are too lengthy for clinical utility.20–22
PIMS and early breastfeeding cessation have been associated with a variety of maternal factors, including age, parity, educational attainment, previous breastfeeding duration, medications, BMI, and depression status.15,23–27 In this study, predictive models relying solely on maternal characteristics were poor predictors of PIMS status. Maternal depression was the only factor that significantly differentiated PIMS participants from PAMS participants. However, the physiologic impact of maternal depression on maternal milk supply remains unclear. 28 In fact, the body of literature concerning the effect of maternal factors on breastfeeding cessation is somewhat conflicting.21,22
Adding a single genetic variant associated with PIMS status to a model that included maternal factors markedly increased predictive accuracy. If validated in a larger external cohort, such a tool could be used to identify mothers at risk for PIMS in the newborn nursery, and provide targeted, sustained lactation support directed at waning milk supply. Such support might include early introduction of galactagogues, increased caution concerning use of medications with antigalactic activity, and continuous education at regularly scheduled lactation visits. Since PIMS may also affect breastfeeding duration in subsequent children,24,25 the implementation of preventative measures could yield sustained benefits in multiparous women.
Biological connections
Although the name “milk fat globule EGF and factor V/VIII domain containing gene” implies a strong relationship with breast milk production, few studies have investigated the lactogenic role of MFGE8.29–31 The major protein product of MFGE8, lactadherin, is a glycoprotein involved in apoptotic phagocytosis, angiogenesis, and exosomal signal transduction. 32 Due to its role in apoptosis and angiogenesis, it has been linked with several inflammatory conditions in humans.
Studies in goats have identified four novel variants in MFGE8, and showed that three of these missense mutations were associated with decreased milk fat yield. 29 In mice, alternative splicing of the MFGE8 protein product into short and long variants resulted from skipping one exon that encoded a proline-/threonine-rich domain. 30 Interestingly, the long variant of MFGE8 was expressed predominantly in the mammary gland, and levels increased in late gestation and persisted throughout lactation.
Mice with mutations in MFGE8 have disrupted clearance of epithelial cells during mammary gland involution, and absence of the MFGE8 protein product leads to irregular remodeling of the mammary gland. 31 However, to our knowledge, no study has examined MFGE genotype in lactating women. The rs2271714 variant, which displayed an association with PIMS status and exclusive breastfeeding duration, typically results in a substitution of adenosine for guanosine at chr15:88906772. The clinical significance of this substitution has not been previously reported; however, it could potentially cause a Leu>Val change in the lactadherin preprotein isoform a, disrupting alternative splicing patterns that occur during lactation. Further investigation into the functional significance of this variant is necessary.
Strengths and limitations
This study is the first to examine the role of 18 lactogenic genes in unexplained milk insufficiency in humans. The prospective longitudinal design defines breast milk production at multiple time points and avoids artificial posthoc comparisons between case–control groups that may have underlying medical/demographic differences predisposing them to PIMS.
However, as with all prospective longitudinal studies, dropouts (40/221; 18%) may have contributed to attrition bias in the final cohort, and imputation of missing data (26/190 data points; 13.6%) may have contributed to ascertainment bias. Our regression model controls for several important maternal factors thought to impact milk supply (e.g., age, previous breastfeeding duration, BMI, education level, and depression); however, other important factors, such as milk removal frequency, were not collected. We acknowledge that the definition of PIMS is implicitly subjective and imprecise.
Although we have attempted to verify its relevance through maternal estimates of breast milk production (which differed between PIMS and PAMS groups), these estimates were not collected in the first month after delivery, may have missed mothers with very early inadequate milk production, and are inferior to validated approaches utilizing 24-hour infant weights or hourly pumping protocols. However, the difference in infant weight trajectory between PIMS and PAMS groups lends additional credence to the assumption that mothers with PIMS did experience lower milk production. Exclusion of seven mothers whose infants experienced below average weight gain could bias the findings. We note that one of these women was homozygous for the minor allele at rs2271714 and six were homozygous for the major allele.
Although this study is exploratory, and small in size, a posthoc power analysis using joint analysis for genome-wide association 33 determined that the study's sample size (n = 43) provided >80% power for detecting associations between genotype and PIMS status, based upon an additive disease model, a 15% prevalence rate of PIMS, and observed allele frequencies for rs2271714 (MFGE8). A power calculation using the Wald's test determined that the sample size also provided 80% power to detect an odds ratio >2.35 among binary covariates on logistic regression, given the observed case–control ratio.34,35 Thus, the study was adequately powered to assess the discriminative ability of lactogenic genotypes.
Conclusions
PIMS is a major source of early breastfeeding cessation and formula introduction, but it is difficult to identify women at risk for lactation difficulties. In this study, we describe a variant within MFGE8, which could potentially aid identification of mothers at risk for PIMS. Such information might be used to provide early, targeted lactation support, including galactagogue supplementation, or early scheduling of “nurse and pump” routines. This finding will require prospective validation in a larger cohort.
Footnotes
Acknowledgments
The authors thank Jessica Beiler for assistance with protocol development, and Amy Shelley, Amyee McMonagle, Makaila Ranges, Kerry Deitrick, Erica Miller, Jennifer Stokes, and Patricia Carper for assistance with recruitment and data collection.
Disclosure Statement
The authors have no related conflicts of interest to declare.
Funding Information
This study was funded by grants from the Gerber Foundation to S.D.H. and the Center for Research on Women and Newborns (CROWN) Foundation to S.D.H.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.