
Abstract
Background:
New variants are evolving in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and receptor binding domain (RBD) mutations have been associated with a higher capacity to evade neutralizing antibodies (NAbs). We aimed at determining the impact of COVID-19 vaccine and infection on human milk antibody titers and activity against the RBD mutations from SARS-CoV-2 variants of concern.
Materials and Methods:
Milk samples were collected from 19 COVID-19 vaccinated women, 10 women who had a positive COVID-19 PCR test, and 13 unvaccinated women. The titers and NAbs of secretory IgA (SIgA)/IgA, secretory IgM (IgM)/IgM, and IgG against SARS-CoV-2 RBD with mutations N501Y or E484K were measured by using ELISA and a surrogate virus neutralization assay.
Results:
The titers of human milk IgG against N501Y were higher in the COVID-19 vaccine group than in the no-vaccine group but comparable with the COVID-19 PCR group. Other antibody titers did not differ between the three groups. The titers of SIgA/IgA were higher than those of SIgM/IgM and IgG in all three groups. The titers of SIgM/IgM and the inhibition of NAbs were higher against the mutation E484K than N501Y. Milk NAb did not differ between the three groups, but the inhibition of NAb against binding of the two mutant RBD proteins to their receptor was higher in the COVID-19 vaccine and PCR groups than in milk from prepandemic women.
Conclusions:
COVID-19 vaccination and exposure of mothers to SARS-CoV-2 influenced the titers and NAbs in breast milk against the variants of concern.
Introduction
Infants have a lower abundance of antibody-secreting cells than children and adults, which make them more susceptible to infectious diseases.1,2 This lack of antibody responses in newborns is primarily compensated by the transfer of maternal antibodies from human milk (primary secretory IgA [SIgA]) and from the placenta (IgG). 3 Moreover, the effectiveness of vaccines is reduced in infants younger than 2–6 months depending on the type of vaccine.4,5 Therefore, neutralizing antibodies (NAbs) against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from human milk is thought to provide passive immunity to infants against coronavirus disease 2019 (COVID-19) during the first 6 months of life. 6
Recent studies revealed that SARS-CoV-2-specific IgG but not IgA increased in maternal blood and human milk from COVID-19 messenger RNA (mRNA)-vaccinated mothers.7–10 This lack of IgA response is likely related to the intramuscular vaccination, which triggers a robust systemic response without a major mucosal response. In contrast, natural infection by SARS-CoV-2 induced a strong SIgA response at mucosal sites, including in human milk.11–15
SIgA plays a crucial role in mucosal immunity by neutralizing and preventing the virus from attaching to epithelial cells and thereby host infection. 16 After COVID-19 disease, purified IgA from serum or saliva was more potent in neutralizing SARS-CoV-2 than paired purified IgG. 17 It remains unclear whether the weaker mucosal response in COVID-19-vaccinated mothers compared with COVID-19-recovered mothers correlates with a similar decrease in NAbs in human milk.
New variants of SARS-CoV-2 are evolving and receptor binding domain (RBD) mutations have been associated with enhanced infectivity, greater transmissibility, and a higher capacity to evade NAbs. One recent study reported that the NAbs against the B.1.1.7 variant (United Kingdom) and particularly against the B.1.351 variant (South Africa) was reduced compared with the wild-type SARS-CoV-2 in milk from COVID-19-vaccinated mothers and infant cord blood. 8 The N501Y mutation may help the virus to spread more easily, whereas the E484K mutation has been suggested to reduce antibody responses and promote immune escape.18,19
The binding and neutralizing activity of antibodies produced after COVID-19 recovery or vaccination against these novel variants remain unexplored. Therefore, in this study, we determined the titers and neutralizing activities of SIgA/IgA, SIgM/IgM, and IgG antibodies in human milk fromCOVID-19-vaccinated women, -recovered women, and -unvaccinated women against the RBD SARS-CoV-2 harboring the mutation N501Y or E484K. We hypothesized that milk from women in the COVID-19 vaccine group would have higher IgG titers and lower IgA titers against the variant SARS-CoV-2 RBDs than milk from women in the COVID-19 recovered group, and that both groups had higher levels of NAbs than the unvaccinated/uninfected group.
Materials and Methods
Study design and participants
A screening survey was completed by donors at the Mothers Milk Cooperative (Boulder City, NV) to identify donors that had been vaccinated against COVID-19 and/or had a SARS-CoV-2 infection confirmed by reverse transcription-PCR. The 10 participants with a positive COVID-19 PCR were asked to report when they were sick. The 19 participants vaccinated with COVID-19 vaccine were asked for the date of their doses and what vaccine they were given. The survey also identified 13 donors lacking COVID-19 vaccination and any previous positive COVID-19 PCR test based on the survey answers. The inclusion criteria were completing a health questionnaire, and a survey related to COVID-19.
Written consent to use their milk for research purposes was obtained from all participants. Donors were approved through Mothers Milk Cooperative. Milk collection was approved by the institutional review board (IRB00012424) of Medolac Laboratories. The exclusion criteria were donors who were smoking, taking medications, or other drugs. Human milk was collected and was previously described in our recent studies.14,15
Antibody titers
The area under the curve (AUC) of antibodies reactive to RBD-SARS-CoV-2 harboring the mutation N501Y or E484K was determined by using ELISAs as described in our recent studies,14,15 with some modifications (Supplementary Data S1). Microplates were coated with recombinant SARS-CoV-2 RBD protein with the mutation N501Y or E484K. Milk supernatant samples were diluted in serial twofold dilutions in blocking buffer. Interpolation of a standard curve was created by using four points (in duplicate) for each sample, and the AUC was calculated by using GraphPad Prism ( GraphPad Software, version 9, San Diego, CA).
Neutralizing antibodies
The neutralizing ability of human milk antibodies against the SARS-CoV-2 RBD with mutations E484K and N501Y was determined via a SARS-CoV-2 surrogate virus neutralization (sVNT) test as described by Tan et al., 20 with some modifications (Supplementary Data S1). Microplates were coated with human ACE2 protein. Biotinylated SARS-CoV-2 RBD(E484K) or RBD(N501Y) at 3 ng was preincubated with supernatant samples (diluted five times with blocking buffer) for 1 hour, before addition into the plate coated with hACE2 for 1 hour. After washing, the wells were incubated with 44 ng streptavidin-peroxidase polymer for 1 hour.
OD450 values were normalized to the OD450 of the well, where no biotinylated RBD was added (5 × milk diluted). A negative control (only blocking buffer) and a positive control (only biotinylated RBD with blocking buffer) were added in each plate to calculate the inhibition.
Statistical analysis
The neutralizing ability of the Kruskal–Wallis test followed by Dunn's multiple-comparison test was performed by using GraphPad Prism to compare the titers or neutralizing activity between groups. Mann–Whitney test was used to determine the effect of isotype and type of vaccine. Linear regression was performed to evaluate differences between the titers or NAbs and the maternal age, lactation time, and the elapsed time from infection or vaccine to sample collection. A heatmap of the correlation matrix (Pearson, r) was created between the measurements in each individual group and combined groups. The sample size was determined based on antibody titers detected in our previous study.14,15
Results
Maternal demographics
The demographic details of the three groups are presented in Table 1. The maternal age, postpartum time, and infant gender were comparable and not significantly different between the three groups (Supplementary Fig. S1 and Table 1). Of the women in the COVID-19 vaccine group, 63.1% received the Moderna mRNA vaccine, whereas 36.8% women had taken the Pfizer/BioNTech mRNA vaccine. The elapsed time from vaccination to milk collection was 37 ± 20 (7–75) days after the second dose. For the COVID-19 PCR group, the elapsed time from their positive PCR test to milk collection was 63 ± 40 (9–122) days. The COVID-19 vaccine group had a higher rate of influenza vaccination (94.7%) than the women in the COVID-19 PCR group (30%) and the COVID-19 no-vaccine group (61.5%).
Demographic Description of COVID-19-Vaccinated Women, -Recovered Women (Had a Positive COVID-19 Polymerase Chain Reaction Test), and -Unvaccinated Women
Women were diagnosed with a positive COVID-19 PCR test with a nasal swab. Viral symptoms reported were cough, fatigue, fever, sore throat, headaches, and loss of taste/smell.
Data are presented as mean ± SD (min and max).
N/A, not applicable.
Antibody titers
To determine whether the antibody response in milk against SARS-CoV-2 variants of concern differs between women vaccinated against COVID-19 (COVID-19 vaccine group), those who recovered from COVID-19 infection (COVID-19 PCR group), and women who were unvaccinated against COVID-19 and without a positive PCR test (No vaccine group), we determined the titers of IgG, SIgA/IgA, and SIgM/IgM against SARS-CoV-2 RBD variants with mutations N501Y and E484K. We found that the titer of RBD(N501Y)-reactive IgG in human milk samples was 8.8-fold higher in the COVID-19 vaccine group than in the no-vaccine group (p = 0.0011, Fig. 1a), whereas no significant differences in IgG titers were observed between the COVID-19 vaccine group and the COVID-19 PCR group or the COVID-19 PCR group and the no-vaccine group (Fig. 1a).

Effect of COVID-19 vaccine and infection on the antibody titers against SARS-CoV-2 RBD mutations. Violin plots show the AUC for
When analyzing the IgG titers against RDB(E484K), no similarly significant increase was observed in the COVID-19 vaccine group (Fig. 1d). Also, no significant differences in titers of RBD(N501Y)- or RBD(E484K)-reactive SIgA/IgA or SIgM/IgM were observed between milk samples from the three groups (Fig. 1b, c, e, f). Importantly, the antibody titers did not differ between Moderna and Pfizer/BioNTech vaccines (Supplementary Fig. S2a–c)
When comparing the reactivity against the SARS-CoV-2 RBD variants, we found that the titers of SIgM/IgM were 3.0-fold higher against E484K than N501Y in milk from all women (p = 0.0001, Fig. 2a) but did not differ for SIgA/IgA or IgG (Fig. 2b, c).

Effect of SARS-CoV-2 RBD mutations and isotypes on the titers and neutralizing activity of antibodies in human milk. Violin plots show the AUC of antibodies against SARS-CoV-2 RBD variants with mutation E484K or N501Y (n = 42 for women) for
When comparing the antibody reactivity to SARS-CoV-2 RBD variants with mutations N501Y and E484K, and its association with each antibody isotype, we found that the titers of SIgA/IgA were higher than the titers of SIgM/IgM and IgG in all three groups, whereas the SIgM/IgM and IgG titers were comparable within each of the three groups (Fig. 2d, f). This observation was not surprising, as SIgA is the dominant antibody in human milk. The COVID-19 vaccine group had the highest proportion of IgG against both N501Y and E484K compared with the COVID-19 PCR and no-vaccine groups (Fig. 3a
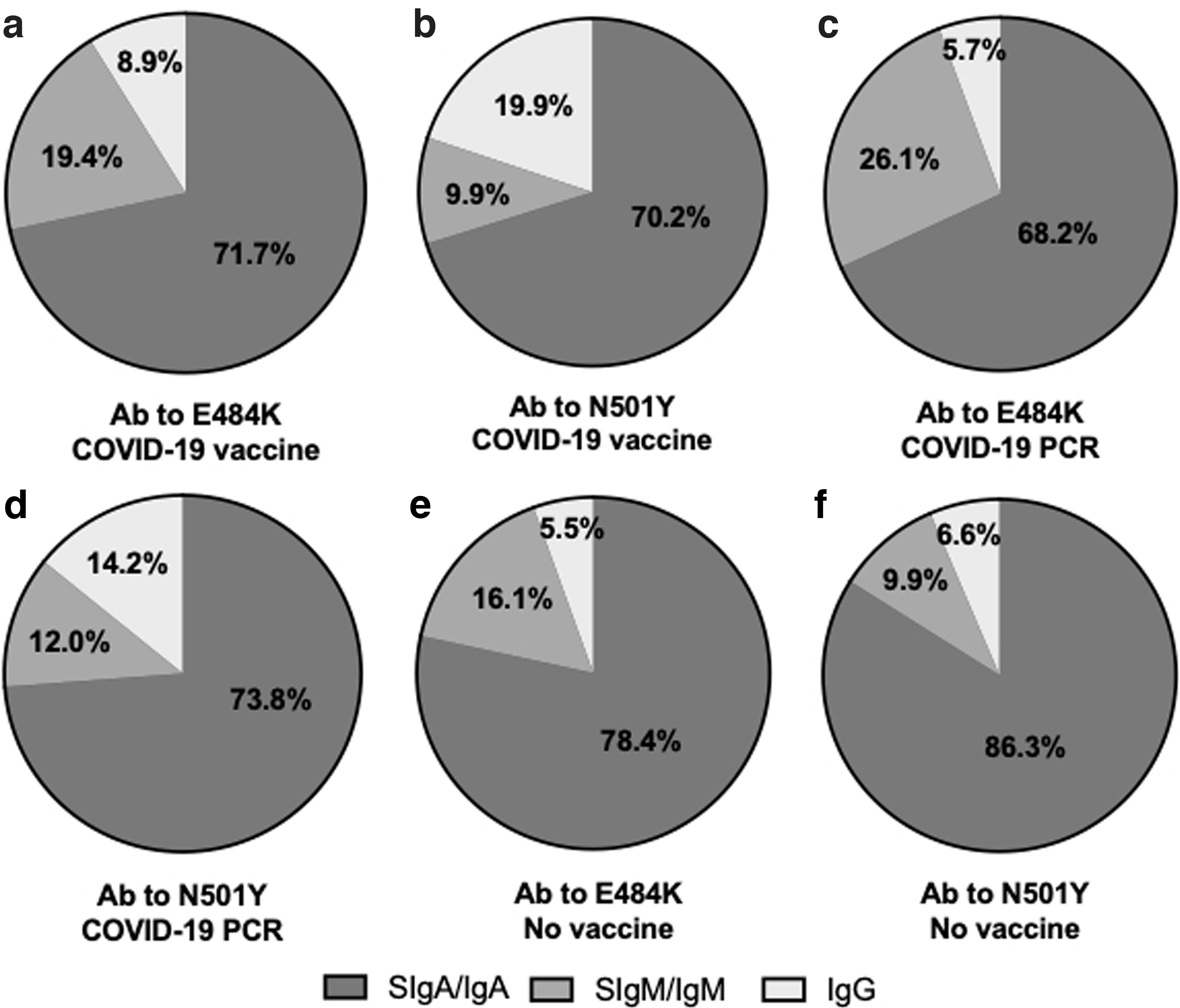
The proportion of isotypes SIgA/IgA, SIgM/IgM, and IgG against SARS-CoV-2 RBD variants with mutations E484K or N501K in human milk.
Correlation between the antibody isotypes titers within each group
As we observed some global differences in antibody isotype titers to be reactive against the two variants and as the proportion of the various isotypes differed between groups, we next wanted to determine the specific effect of COVID-19 vaccination and previous COVID-19 infection on the antibody isotype titers. Thus, the titers of the distinct antibody isotypes in the milk samples were correlated within each group and these correlations were then compared between the three groups (Fig. 4a

Matrix heatmaps show correlations between antibody titers (isotypes SIgA/IgA, SIgM/IgM, and IgG) and NAbs against the SARS-CoV-2 RBD variants with mutations E484K and N501K in human milk. Titers and NAbs from
First, N501K-reactive SIgA/IgA was positively correlated with E484K-reactive SIgA/IgA in the COVID-19 vaccine group (p = 0.011, Fig. 4a) and tended to be correlated also in the COVID-19 PCR group (p = 0.095, Fig. 4b), whereas no correlation was observed in the no-vaccine group (Fig. 4c), suggesting that both vaccination and infection promotes SIgA secretion in the milk against both variants.
Second, N501K-reactive SIgA/IgA was negatively correlated with E484K-reactive SIgM/IgM in the COVID-19 vaccine (p = 0.012, Fig. 4a) and in the COVID-19 PCR (p = 0.013, Fig. 4) groups and a similar trend was detected in the no-vaccine group (p = 0.10, Fig. 4). Third, N501Y-reactive IgG was positively correlated with E484K-reactive IgG (p = 0.003) in the COVID-19 vaccine group, a correlation that was not observed in either the COVID-19 PCR or the no-vaccine groups, suggesting a role of vaccination in IgG secretion in the milk.
In addition, N501Y-reactive IgG was also positively correlated with N501Y-reactive SIgM/IgM (p = 0.004, Fig. 4a) in milk from the COVID-19 vaccine group, whereas no such correlation was observed in the two other groups. However, this correlation was not as clear for IgG reactive to E484K in the COVID-19 vaccine group, but instead a strong positive correlation between E484K-reactive IgG and E484K-reactive SIgM/IgM was observed in the COVID PCR group (p = 0.022, Fig. 4b). Combined, the pattern of correlations observed in the COVID-19 vaccine group displayed some overlapping patterns with that observed in the COVID-19 PCR group (Fig. 4d), whereas these patterns were mostly different from those in the no-vaccine group.
Neutralizing antibodies
We next assessed the functionality of the milk antibodies by determining their ability to inhibit the binding of the SARS-CoV-2 RBD variants with mutation E484K and N501Y to their receptor, human angiotensin-converting enzyme 2 (hACE), in a SARS-CoV-2 sVNT test. The NAb activity was measured as % inhibition of RBD binding to hACE2 at five times dilutions of milk samples. To interpret our neutralization data more accurately, we also included milk samples collected before the pandemic in the analysis. The inhibition was generally high and comparable within the three groups for NAb against E484K and N501Y (Fig. 2g
However, the % inhibition of antibodies against E484K in milk samples from the COVID-19 vaccine group (p = 0.009) and the COVID-19 PCR group (p = 0.015) was significantly higher than the inhibition observed in the prepandemic group and tended to be higher also for the no-vaccine group (p = 0.095, Fig. 2g). When comparing NAb against N501Y, the COVID-19 vaccine (p = 0.005), the COVID-19 PCR (p = 0.003), and the no-vaccine (p = 0.025) groups, all had a significantly higher % inhibition than the prepandemic group (Fig. 2h). The % inhibition of NAb in human milk from all women (COVID-19 vaccine, COVID-19 PCR, and no-vaccine groups combined) was significantly more pronounced against E484K than against N501Y (p < 0.0001, Fig. 2i).
Correlation between titers and NAbs
To better understand whether the titers of the distinct antibody isotypes in the milk samples were associated with the ability of the milk to neutralize RBD binding to its receptor, antibody titers and neutralizing activity were correlated. NAb against N501Y tended to be positively correlated with NAb against E484K in the COVID-19 vaccine group (p = 0.095, Fig. 4a), and it significantly correlated in the COVID-19 PCR group (p = 0.025, Fig. 4b), whereas no correlation was detected in the no-vaccine group (Fig. 4c). NAb against N501Y was correlated with SIgM titers against E484K (p = 0.025, Fig. 4b), and it tended to correlate with IgG titers against E484K (p = 0.071) in the COVID-19 PCR group. The correlations between NAb and isotype titer were absent in the COVID-19 vaccine group, and they were mostly negatively correlated in the no-vaccine group.
Variation of antibodies between women
A strong variation of antibody titers between mothers was observed in the three groups, and high titers against one RBD variant was not necessarily correlated with high titers also against the other. In addition, high titers of one Ig isotype were not directly correlated with high titers of the two other isotypes (Fig. 5a–c).

Heatmaps of the titers and NAbs against the SARS-CoV-2 RBD variants with mutations E484K or N501K in human milk.
The elapsed time from COVID-19 vaccination to milk collection varied from 7 to 75 days. However, no correlation was observed between the elapsed time from COVID-19 vaccination to milk collection and any of the antibody titers in this group. In this group, SIgA/IgA titers were positively correlated with the elapsed time from infection to milk collection (Supplementary Fig. S3a), whereas no correlation was detected for SIgM/IgM and IgG. NAbs were not influenced by the elapsed time from infection or vaccine to milk collection.
Maternal factors
The titer of IgG reactive to both N501Y and E484K was positively correlated with the maternal age in all groups (Supplementary Fig. S3d). NAbs were not changed by the maternal age. Influenza vaccine and infant gender did not influence the antibody titers and NAbs.
Discussion
In this study, we measured the antibody titers of immunoglobulin isotypes as well as the ability of antibody to neutralize novel SARS-CoV-2 Spike protein variants to its receptor in milk from women vaccinated against COVID-19, with prior infection with COVID-19 or in milk from women who had not been vaccinated and had no history or positive PCR test for COVID-19. We used the N501Y mutation that has been identified in variants B.1.1.7, B.1.351, and Brazil P.1 and is thought to make the virus spread more efficiently. 21 We also investigated antibody activity against the E484K mutation that was detected in these same variants and is thought to help the virus escape antibodies. 22
Antibody titers and NAbs against the SARS-CoV-2 RBD with mutations E484K and N501Y were quantified in milk from COVID-19-vaccinated, -infected, and unvaccinated/uninfected women. We were able to show, for the first time, that the IgG titer against N501Y was significantly higher in the COVID-19 vaccine group than in the no-vaccine group but did not differ for IgG against E484K, although a few milk samples had titers higher than in both the other groups. These results suggest that the COVID-19 vaccine increased human milk IgG that recognizes the mutation N501Y. This observation agrees with recent studies demonstrating that IgG titers specific to SARS-CoV-2 RBD were higher in milk collected after COVID-19 vaccination than in pre-vaccine milk.7,8,23
Comparing the Ig isotypes, SIgA/IgA titers against the E484K and N501Y RBD variants in milk were higher than SIgM/IgM and IgG in women from the COVID-19 vaccine, COVID-19 PCR/infection, and no-vaccine group. However, SIgA/IgA and SIgM/IgM titers against RBD E484K and N501Y did not differ between the three groups. This is in contrast to Gray et al., 7 who reported that human milk titers of IgA and IgM specific to the spike protein were higher in postvaccine (2–6 weeks after the second dose of Moderna or Pfizer vaccines) than in prevaccine milk. The lack of difference in antibody titers for SIgA/IgA and SIgM/IgM between COVID-19 vaccine, COVID-19 PCR/infection, and the no-vaccine group could be related to longer elapsed time from vaccination to milk collection in several mothers.
SARS-CoV-2 spike-protein specific SIgA/IgA levels were reduced after 20–30 days after the COVID-19 vaccine in human milk from 5 women 24 and 32 women after 43 days postvaccination. 25 Another explanation could be that the unvaccinated/uninfected women in the no-vaccine group may have experienced asymptomatic COVID-19 infection, resulting in some level of immune response with production of Ig isotypes against the SARS-CoV-2 RBD region. We recently demonstrated that the COVID-19 infection group had higher titers of SIgA/IgA, SIgM/IgM, and IgG specific to SARS-CoV-2 RBD than in pre-pandemic groups. 14
Also, the mutations of SARS-CoV-2 RBD used here could also explain the absence of significant differences for the Ig isotype titers between the three groups, potentially due to a reduced ability of antibodies to bind on RBD E484K and N501Y. Collier et al. 8 found that serum antibody titers from vaccinated lactating and pregnant women were reduced against the B.1.1.7 variant (United Kingdom) and strongly decreased against B.1.351 variant (South Africa).
We further found that the SIgM/IgM titer was higher against E484K than N501Y but that titers did not differ for SIgA/IgA and IgG between the groups. Interestingly, the inhibition of NAb against E484K was also higher than that of NAb against N501Y. These results suggest that human milk IgM recognized the mutation E484K more readily than N501Y from SARS-CoV-2 RBD. However, the increased IgM titers against the E484K RBD could not directly explain the neutralizing activity, as NAb inhibition did not correlate with the SIgM/IgM titers against this RBD variant, suggesting that a subportion of antibody rather than the total IgM antibodies were responsible for neutralization and protection.
In the COVID-19 vaccine group, we found positive correlations between N501Y SIgA/IgA and E484K SIgA/IgA titers and between N501Y IgG and E484K IgG titers, indicating that antibodies produced after vaccination in response to the wild-type spike protein are reactive to both mutant spike protein variants. These correlations were absent in the COVID-19 PCR/infection and no-vaccine groups. The lack of correlation between titers in the COVID-19 PCR/infection group may well be related to differences in severity and disease progression, and different amounts/dosage of the virus over time between women in this group that could be associated with variable immune responses were raised to the whole virus.
In contrast, the COVID-19 PCR/infection group displayed positively correlated NAb for N501Y and E484K, which was not detected in the other groups, although a trend toward a correlation was observed in the COVID-19 vaccine group. These results suggest differences in the antibody response and recognition between COVID-19-vaccinated women, COVID-19-recovered women, and unvaccinated women. Differential human milk IgG- and IgA-antibody responses specific to SARS-CoV-2 have been identified in maternal infection and vaccination. 8 The factors influencing the variation of NAbs in human milk are still not understood.
When investigating NAb further, we found that human milk NAbs against N501Y and E484K were higher in the COVID-19 vaccine and the COVID-19 PCR/infection group than in the pre-pandemic control. We also observed that the unvaccinated women had higher human milk NAb against N501Y than in the pre-pandemic group, again suggesting the potential that they have been asymptomatically exposed to the virus. The presence of a low level of NAb in milk from pre-pandemic donors could be due to the polyreactive properties of SIgA and SIgM to bind to different epitopes.12,13,26,27 This result suggests that most lactating women could secrete human milk antibodies against the new SARS-CoV-2 variants of concern.
This study also illustrates the importance of not only measuring the total antibody titers but also determining the functionality of antibodies in terms of potential protective immunity. In this study, no specific correlation was observed between the neutralization activity of the milk samples and a specific isotype titer of antibodies, suggesting that titers alone do not predict protective immunity. This concept is well established for other viral pathogens and is an important tool to develop novel vaccines and improve our current vaccines. 28 Although a similar standardized surrogate assay is not yet established for COVID-19, various neutralization assays have been used to assess protection against the current vaccines, including the Moderna and Pfizer/BioNTech vaccines, and NAb is highly predictive of protection. 29
We used the SARS-CoV-2 sVNT test in this study, as it can detect NAbs without the need for any live virus or cells. This test mimics the virus–host interaction in an ELISA plate well. Tan et al. 20 demonstrated that the RBD-ACE2 interaction (sVNT) can be neutralized by specific NAbs in serum, in the same process as the conventional virus neutralization (cVNT) or the pseudovirus-based virus neutralization (pVNT). The % inhibition of NAb from 60 COVID-19 sera measured with sVNT was comparable to those determined with cVNT and pVNT. 20
Our results show that total antibody of various isotypes does not correlate with neutralizing activity of the same antibody. This suggests that only a minor portion of antibodies produced are really neutralizing or protective and that looking at titers alone does not tell the whole story. Therefore, that specific isotype Ig-titers do not correlate with neutralization fits well with that concept and further studies are needed to better define assays that specifically identify those antibodies that confer immune protection.
The limitation of the cohort study had a small sample size and was not a randomized clinical trial. Thus, any differences in the findings among the groups cannot be assumed to be causal.
Conclusion
Our study reveals that COVID-19 vaccine and previous infection by SARS-CoV-2 could influence the human milk antibodies against SARS-CoV-2 RBD with mutations E484K and N501Y present in current variants of the virus circulating throughout the world, but other maternal factors also changed their titers and neutralizing capacities. COVID-19 vaccine can increase IgG titer against some SARS-CoV-2 variants of concern in human milk compared with COVID-19 infection and unvaccinated women, but it does not change IgA or IgM titers. Human milk NAbs against SARS-CoV-2 variants from COVID-19 vaccine, SARS-CoV-2 disease, and women exposed to COVID-19 pandemic have a higher inhibition capacity than pre-pandemic women.
A future study is needed with a greater sample size to investigate the NAbs in human milk longitudinally in individual women (pre-, and post-vaccination, pre- and post-COVID-19 illness, and pre- and post-exposure period with neither vaccination nor obvious infection) to evaluate their association with the specific vaccine received, the specific virus the woman is infected with, and the “circulating” virus(es) within the communities and the periods.
Footnotes
Authors' Contributions
V.D.M. conceptualized and designed the study, carried out ELISA analyses with S.L., and the statistical analysis, drafted the article, and approved the final article as submitted. V.D.M. has primary responsibility for the final content. S.H. recruited donors and collected the completed survey. A.P.H. provided suggestions for analyses and critically revised the article. E.M. and S.F. acquired funding for this study. All authors revised the article and approved the final article as submitted.
Acknowledgments
The authors thank all study participants for their valuable contributions.
Disclosure Statement
V.D.M., S.H., S.L., S.F., and E.M. were employees at Medolac Laboratories. A.P.H. has no conflict of interest to disclose.
Funding Information
The authors (V.D.M., S.H., S.L., S.F., and E.M.) disclosed receipt of the financial support from Medolac Laboratories A Public Benefit Corporation for the conduct of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.