
Abstract
Objective:
The aim of this study was to identify factors associated with requiring surgical treatment for mastitis or breast abscess in postpartum mothers.
Materials and Methods:
This was a retrospective cohort study using the Japan Medical Data Center Claims Database. Information on pairs of infants born between April 2012 and December 2016 and their mothers were extracted. Data regarding the baseline characteristics, medical history, medical practice, and prescription drugs of mothers and their infants were collected. Multivariable logistic regression analysis was used to examine factors associated with undergoing surgical treatment.
Results:
The data of 69,363 eligible mothers were analyzed. The proportion of mothers who were diagnosed with mastitis or breast abscess within 1 year after childbirth was 10.8% (7,516/69,363). There were 114 mothers who underwent surgical treatment within 1 year after childbirth. This was 0.2% of all mothers and 1.5% of those diagnosed with mastitis or breast abscess. Surgical treatment was significantly associated with mothers having their first child (adjusted odds ratio [AOR], 2.58; 95% confidence interval [CI], 1.63–4.07) compared to those with a second or later child; it was also significantly associated with the diagnosis of breast abscess (AOR, 10.38; 95% CI, 5.28–20.40).
Conclusions:
This was the first report of the prevalence of mastitis or breast abscess and the requirement for surgical treatment among postpartum mothers in Japan. A first diagnosis of breast abscess and having a first child were associated with requiring surgical treatment. Health care professionals providing postpartum care should be aware of these factors.
Introduction
Mastitis is an inflammatory condition of the breast with or without infection and is usually associated with lactation. 1 The reported prevalence of mastitis varies from 2.6% to 33% among lactating women, and mastitis commonly occurs during the 2nd and 3rd week of the postpartum period. 1 Delayed or inadequate treatment of mastitis can lead to the development of breast abscess. The proportion of breast abscesses in women with mastitis has been reported to range from 4.0% to 11%. 1 Breast abscesses may require surgical treatment such as incision, drainage, or needle aspiration.
Several studies have investigated risk factors for requiring surgical treatment after the diagnosis of mastitis or breast abscess. In a study performed in Sweden, some risk factors for women who delivered singletons were age older than 30 years, primiparity, and delivery at 41 weeks of gestation or later. 2 A case–control study of postpartum breast abscesses caused by Staphylococcus aureus requiring surgical treatment reported that employment outside home and maternal breastfeeding difficulties identified by a lactation consultant or a postpartum nurse were risk factors. 3
However, other important factors that might be associated with surgical treatment after the diagnosis of mastitis or breast abscess have not been clarified. Mothers' physical and psychological factors and infants' conditions associated with breastfeeding complications may also be associated with surgical treatment. Social demand for preventive care for severe mastitis has increased. Understanding the factors associated with severe cases could help improve the care and support required to prevent severe conditions.
The aim of this study was to identify factors associated with surgical treatment after the diagnosis of mastitis or breast abscess during the postpartum period.
Materials and Methods
Study setting
This was a retrospective cohort study using the Japan Medical Data Center Claims Database (JMDC Inc., Tokyo, Japan), 4 which contains anonymized claims data of corporate employees and their dependent family members obtained from Japanese union-managed health insurances. The data include insurance eligibility information and medical and pharmacy claims of ∼4 million beneficiaries in 2017. Family and personal identifiers, subscribers' sex and year and month of birth, relationship to the main insured person, diagnosis, medical services provided, drugs prescribed, and hospital admissions can be found in the database.
Diagnoses are recorded based on International Classification of Diseases, 10th revision (ICD-10) codes, and the Japanese classification codes. Prescription drugs are recorded according to the Anatomical Therapeutic Chemical (ATC) classification. Mothers and infants can be linked in the database using the family identifier and relationship information.
Case identification
First, infants born between April 2012 and December 2016 were identified and their mothers were linked using family identifiers. Families with no information on the mother were excluded. Families that had two or more possible mothers under the same insurance, families where infants were born when mothers were not enrolled in the insurance (e.g., in cases of remarriage), and families with mothers who lacked follow-up information until 1 year after childbirth were also excluded.
Then we identified episodes of the first perinatal mastitis or breast abscess within 1 year after childbirth using the Japanese codes corresponding to “inflammatory disorders of the breast” or “infections of the breast associated with childbirth,” as listed in the Supplementary Table S1. Those with mastitis or breast abscess before childbirth, whose diagnostic records continued to appear after childbirth, were not included. Women who were diagnosed with breast tumors within 1 year after the diagnosis of mastitis or breast abscess were also excluded.
Variables
The outcome of the study was surgical treatment (puncture or needle biopsy, incision, or aspiration) for mastitis or breast abscess within 1 year after childbirth.
Demographic characteristics of mothers included age at childbirth and dependent family status. Mothers were categorized into having mastitis or breast abscess according to the first diagnosis. When both diagnoses were recorded, mothers were categorized as having breast abscess. We identified medical history of urinary tract infection, throat infection, skin infection, and vaginal candidiasis between childbirth and diagnosis of mastitis or breast abscess (ICD-10 codes N39, J02, L08, and B37.3, respectively), which could increase the risk of infectious mastitis. 5 Use of anxiolytics, psychotropics, or antidepressants between 10 months before childbirth and diagnosis of mastitis or breast abscess were identified (ATC code N05). Antibiotics prescribed on the same day of the diagnosis of mastitis or breast abscess were also identified.
Demographic characteristics of infants included sex, age in months when the mother was diagnosed with mastitis or breast abscess, and birth order. We identified malformations, infectious diseases, low birth weight, and preterm birth using diagnosis codes recorded between childbirth and diagnosis of mastitis or breast abscess. Categories of disease and their respective codes are provided in Supplementary Table S2. We also identified phototherapy, admission to pediatrics department, and admission to neonatal intensive care unit between childbirth and diagnosis of mastitis or breast abscess.
Statistical analysis
We compared the characteristics between those with surgical treatment and those without using the Chi-squared test or the Fisher's exact tests, as appropriate, for categorical variables. A multivariable logistic regression analysis was performed to identify factors associated with the need for surgical treatment. Variables with p < 0.10 in the bivariate analysis and mother's age, which were associated in a previous study, 2 were used in the multivariable regression analysis. Two-tailed p < 0.05 was considered statistically significant. All analyses were performed using SPSS version 25.0 for Windows (IBM Corp., Armonk, NY).
Ethical considerations
Approval for this study was obtained from the Research Ethics Committee of the Graduate School of Medicine, The University of Tokyo [approval number 10862-(1)]. Given the de-identified nature of data, the requirement for informed consent was waived.
Results
Characteristics of the study population
Figure 1 shows participant selection. Among the 69,363 mother/infant pairs, 7,516 (10.8%) diagnosed with mastitis or breast abscess within 1 year after childbirth, fulfilling the inclusion criteria, were analyzed. Of the 7,516 mothers, there were 87 mothers (1.2%) with breast abscess as the first diagnosis. The median duration between childbirth and the diagnosis of mastitis or breast abscess was 2 months (interquartile range [IQR], 1–6 months). Of the 69,363 mothers, 114 (0.2%) underwent surgical treatment of mastitis or breast abscess within 1 year after childbirth. The proportion of mothers who underwent surgical treatment after the diagnosis of mastitis or breast abscess was 1.5%. The median duration between the diagnosis of mastitis or breast abscess and surgical treatment was 15 days (IQR, 4–85 days).
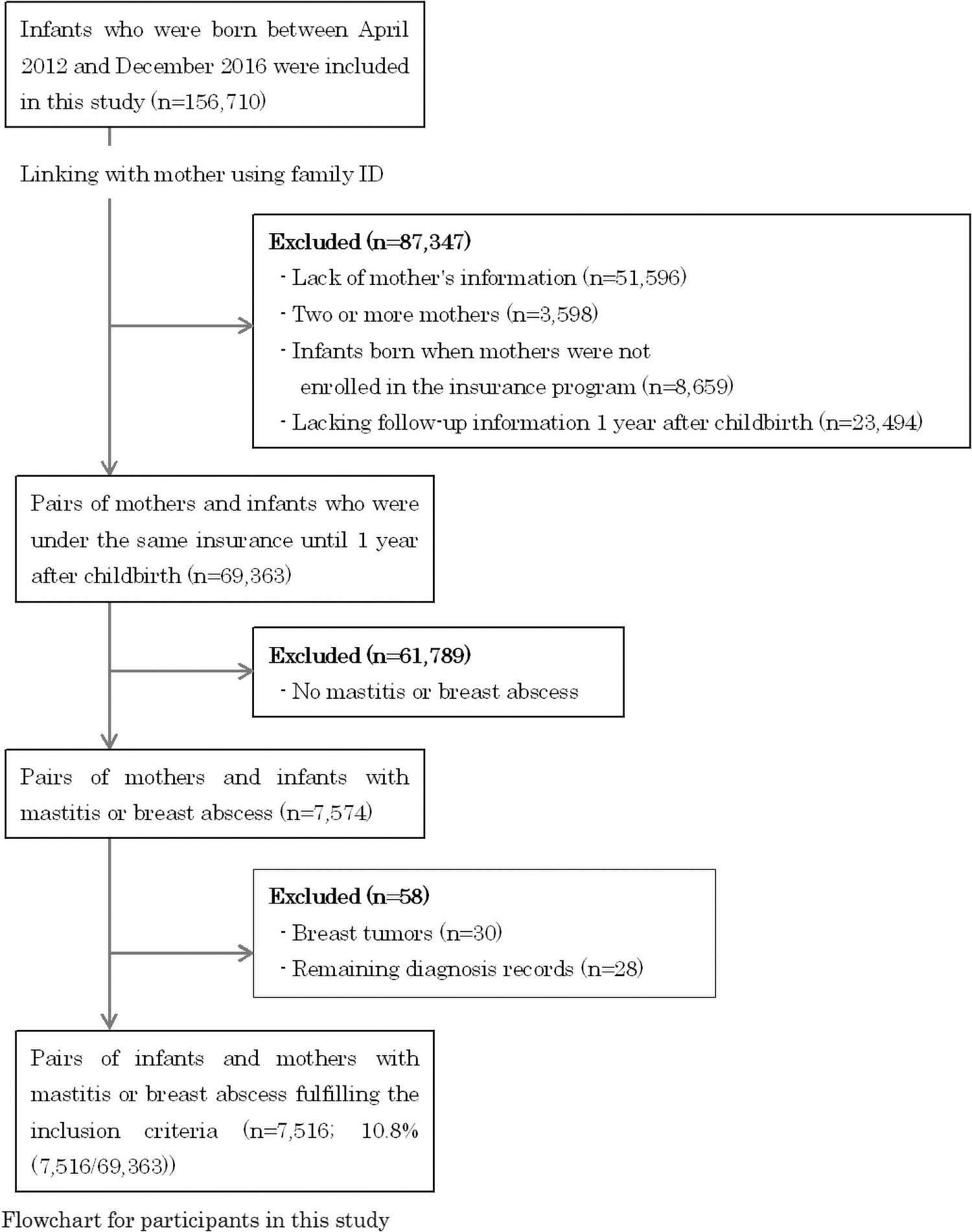
Flowchart for participants in this study.
Participants' characteristics and comparisons using bivariate analyses between mothers with and without surgical treatment are shown in Table 1. The mother's age at childbirth was 30 years or older in 5,156 participants (68.6%). Proportion of participants receiving different types of antibiotics on the day of diagnosis were as follows: cephalosporin only, 48.1%; broad-spectrum penicillin only, 2.8%; other antibiotics, 3.8%; and no antibiotics, 45.4%. In the bivariate analyses, the first diagnosis of mastitis or breast abscess, birth order, and the infant's age were significantly associated with surgical treatment.
Characteristics of Both the Mothers Diagnosed with Mastitis or Breast Abscess and Infants (n = 7,516)
Mastitis or breast abscess (%) in the column, surgical treatment or no surgical treatment (%) in the row of these groups.
Chi-square test.
Fisher's exact test.
Mother's infection, including urinary tract infection, throat infection, skin infection, or vaginal candidiasis.
Other antibiotics, including penem, fluoroquinolone, macrolide, tetracycline, antibiotics for external use, or multiple prescription.
Malformation including oral, cardiovascular, or digestive malformations.
Infant's infection, including Streptococcal sepsis, viral conjunctivitis, diarrhea, gastroenteritis, varicella, hand-foot-and-mouth disease, infectious erythema, exanthema subitum, virus infection, cytomegalovirus infection, pertussis, rubella, herpangina, measles, mumps, respiratory syncytial virus infection, or oral thrush.
NICU, neonatal intensive care unit.
Factors associated with requiring surgical treatment
Table 2 shows the results of multivariable logistic regression analysis. Diagnosis of breast abscess first (adjusted odds ratio [AOR], 10.38; 95% confidence interval [CI], 5.28–20.40) and having a first child (AOR, 2.58; 95% CI, 1.63–4.07) were significantly associated with surgical treatment.
Multivariable Logistic Regression Analysis of Factors Associated with Surgical Treatment (n = 7,516)
AOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
Discussion
This is the first study to report the proportion of mothers who underwent surgical treatment for breast abscess in Japan. Using paired data of mothers and infants from a large-scale claims database, we identified that 7,516 (10.8%) among the 69,363 mothers were diagnosed with mastitis or breast abscess within 1 year after childbirth, and subsequently, 114 (0.2%) required surgical treatment for breast abscess. Factors associated with surgical treatment were initial diagnosis of breast abscess and having a first child.
This study showed that one-tenth of mothers suffered from mastitis or breast abscess, and they were at risk for developing breast abscesses requiring surgical treatment. A previous database study performed in Sweden examined data of all 1,454,068 singleton births from 1987 to 2000 and identified 1,401 (0.1%) that required surgical treatment for breast abscess. 2 The proportion in the Swedish study was similar to that in our study. Health professionals should identify women at high risk for mastitis or breast abscess and provide appropriate preventive care for them.
In this study, mothers with a first child were more likely to require surgical treatment after the diagnosis of mastitis or breast abscess than mothers with a second or later child. A previous study showed that first-time mothers had a 3.6-fold increased risk of breast abscess compared with women with multiparity. 2 As a previous study reported, inexperience in breastfeeding of first-time mothers may increase the risk of mastitis. 6
Mothers who were diagnosed with breast abscess at the first visit were more likely to require surgical treatment compared with mothers with the initial diagnosis of mastitis. This finding suggests that delayed or inadequate care of mastitis could lead to severe outcomes. In Japan, mothers and infants generally receive examinations at hospitals or by visits of health care professionals during the 1st month after birth. Women are less likely to have the next regular opportunity to consult health care professionals after 1 month postpartum health checkups.
Considering the median duration between childbirth and the diagnosis of mastitis or breast abscess was 2 months, and the rather high incidence of mastitis or breast abscess imply the importance of continuous and seamless support for lactating mothers throughout the perinatal period, including accurate assessment of the condition of mothers with breastfeeding troubles and appropriate referral to medical treatment. Especially, up to 6 months of the postpartum period is of importance, as mastitis occurring after then would not be so severe with the start of baby food.
Drugs prescribed to mothers for mental illness between the antenatal period and the diagnosis of mastitis or breast abscess were not associated with surgical treatment in this study. Mothers with mental illness receiving psychoactive drugs may have required additional support from and close monitoring by their health care professionals. This could have led to early detection and proper treatment in this group of patients. To our knowledge, no previous studies reported the association between mastitis or breast abscess and mental illness. Further research is needed to examine the relationship between mothers with mental illness and the development of mastitis or breast abscess.
Infants' factors, which included malformations and infections, were not significantly associated with surgical treatment. A previous study showed tongue-tie as a potential cause of inadequate latching on the mother's breast. 7 In addition, oral thrush in infants was reported to be associated with nipple pain or breast pain. 8 However, these findings have not been confirmed till date. In this study, few infants with malformations or infections were observed, possibly leading to statistically insignificant results. Breastfeeding is a collaboration between a mother and an infant. Further studies are needed to determine factors of infants that affect breastfeeding and lead to mastitis or breast abscess.
The social demand for preventive care for severe mastitis has increased in Japan. The Japanese Midwives Association published the standards of care for mastitis in 2013, 9 which was updated in 2015 10 and 2020, 11 with the aim for uniformity and a guarantee of the quality of breast care. In 2018, the Ministry of Health, Labour, and Welfare created a medical service fee for mastitis aggravation preventive care and guidance. 12 Introduction of the fee was an important milestone, in which midwifery care for mastitis was covered by health insurance for the first time in Japan. The fee is expected to improve the access to breast treatment in maternity homes or outpatient care for postpartum women who have breast problems.
This study is the first report of prevalence and risk factors associated with surgical treatment after diagnosis of mastitis or breast abscess in Japan. These results may be used as baseline data for evaluating an impact of health insurance system on the trends of mastitis, breast abscess, and subsequent surgical treatment in the future.
This study has several strengths. This study showed the proportion in a large group of corporate employees or their dependent family members under Japanese health insurance system. Moreover, in previous studies of mastitis, most symptoms were identified from telephone interviews or self-reported questionnaires. 13 The definition of mastitis was also different across studies. In this study, diagnostic information derived from medical records avoided the mother's subjectivity and recall bias.
Some limitations of this study should be acknowledged. First, this study used a health insurance claims database, and data regarding the diagnosis were obtained using claims records. Diagnostic criteria could have varied depending on physicians. Second, data were excluded from the analyses if a mother and an infant were not enrolled in the same insurance. For example, when a father and an infant were in the same insurance and the mother had another type of insurance, data were not collected. Third, data regarding symptoms or treatment that are not covered by insurance were not included. For example, as of 2017, breast care by midwives was not covered by health insurance.
A medical service fee for mastitis aggravation preventive care and guidance was created in 2018. 12 Finally, information regarding breastfeeding practices was not available. Further studies are needed to examine the effect of mothers' breastfeeding practice and midwives' support.
Conclusions
Among the 69,363 mothers, 7,516 (10.8%) were diagnosed with mastitis or breast abscess within 1 year after childbirth and 114 (0.2%) required surgical treatment for breast abscess. Factors associated with receiving surgical treatment after the diagnosis of mastitis or breast abscess included the following: a first diagnosis of breast abscess and having a first child. The social demand for preventive care for severe mastitis has increased. The prevalence found in this study can be used as baseline data for mastitis in Japan. In addition, health care professionals providing postpartum care should be aware of the risk factors identified in this study.
Footnotes
Authors' Contributions
Conception of the work, C.S.; design of the work, C.S., M.H., E.S., K.Y., N.H., Hay.Y., K.M., Hid.Y., and H.M.; acquisition of data, Hid.Y. and H.M.; analysis of data, C.S., Hay.Y., and K.M.; interpretation of data, C.S., Hay.Y., K.M., Hid.Y., and H.M.; drafting the work, C.S.; revising the work critically for important intellectual content, M.H., E.S., K.Y., H.N., Hay.Y., K.M., Hid.Y., and H.M.; final approval of the version to be published, all authors; and agreement to be accountable, all authors.
Disclosure Statement
The authors declare that they have no conflict of interest that might bias the outcomes of this article.
Funding Information
This work was supported by grants from the Ministry of Health, Labour and Welfare, Japan (21AA2007), and the Ministry of Education, Culture, Sports, Science and Technology, Japan (20H03907 and 21H03159).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.