
Abstract
Background and Objectives:
Breastfeeding women are generally excluded from clinical trials with new vaccines. The objective of the study was to explore whether the BNT162b2 mRNA and mRNA-1273 COVID-19 vaccines are safe for breastfeeding mothers and their breastfed infants.
Methods:
A convenience sample prospective cohort single institution study was performed on breastfeeding health care professionals, who were exposed to second dose of SARS-CoV2 vaccine at the beginning of the study period. They and their breastfed children's symptoms were followed up through online questionnaires for 14 days.
Results:
Of the 95 finally included participants, only 1 was lost to follow-up on day 7. Mean age of the mothers was 35.9 ± 3.9 years and that of their infants was 14.6 ± 12.1 months. At least one adverse event was reported by 85% (95% confidence interval [CI]: 76–91.5%) of the mothers. The most frequent was injection site pain in 81% of cases. Moreover, 31% (95% CI: 22–41%) observed some event in their breastfed children. Most frequently, 19% (95% CI: 13–30%) of the children were irritable. During the 14 days of follow-up, 36% of the children (95% CI: 27–46%) were diagnosed with respiratory infection.
Conclusions:
Most mothers' reactions were mild and transitory, generally limited to the first 3 days after vaccination. Many children's events were associated with concomitant infectious processes and we did not detect a notable peak on any particular day of follow-up. Neither mothers nor their infants developed serious adverse events nor were they diagnosed with COVID-19 within the study period.
Introduction
On December 31, 2019, the Wuhan Municipal Health and Sanitation Commission reported an outbreak of pneumonia of unknown etiology but of common origin, with some of the cases being severe. As early as January 12, 2020, the genetic sequence 1 of the causative virus, a member of the Coronaviridae family, was released under the name SARS-CoV-2. Since then, the clinical pattern in SARS-CoV-2 infections, termed COVID-19, turned out to be variable, with disease-related mortality rates exceeding 12% in some countries. To date, the SARS-CoV-2 pandemic poses an extraordinary challenge to global health. As of yet, >400 million cases have been notified worldwide, causing the death of >5 million people. 2
This has led to large-scale investments in funding for treatment and vaccine research. As a result, less than a year after virus genome sequence publication, emergency use authorization for a candidate vaccine was requested from the United States Food and Drug Administration (FDA). Four vaccines against COVID-19 are currently marketed in Europe, three of which were approved by the FDA and all four by the European Medicines Agency (EMA).3–8
Breastfeeding women are excluded from clinical trials with drugs, which implies that technical data sheet for >95% of the marketed drugs 9 does not provide information on their safety and efficacy during breastfeeding. Vaccines against SARS-CoV2 are no exception to this rule. The technical data sheet of the currently marketed vaccines states that nothing is known about their excretion into breast milk.
This point has generated fear of COVID-19 vaccination in mothers, which has led various scientific societies to issue an information statement that offers or recommends vaccination to breastfeeding individuals who belong to a risk group. However, this recommendation was not coordinated between countries. 10
In the Canary Islands, vaccination of health care workers started in January 2021. This study was based on the hypothesis that vaccination against SARS-CoV-2 is as safe in breastfeeding women as in the clinical trial population and does not cause adverse events in their breastfed infants.
Methods
Study design, population
A prospective cohort study was carried out in health care professionals who were breastfeeding at the time of their COVID-19 vaccination with either the BNT162b2 or the mRNA-1273 vaccine. The mothers were enrolled when getting their second dose of vaccine. All received written information and signed their own and the tutored informed consent for their breastfed children.
Any type of breastfeeding, that is, exclusive (breast milk only), supplemented (breast milk in combination with other liquids or infant formula), and complemented breastfeeding (breast milk in combination with other liquids and solid food), and any infant age were accepted. Risk factors for suffering severe COVID-19 were collected in mothers and infants (Table 1). Exclusion criteria were human immunodeficiency virus infection, disease or treatment causing immunosuppression, known previous COVID-19 infection, symptoms consistent with COVID-19 infection during the study period, or SARS-CoV-2 immunoglobulin M (IgM) or immunoglobulin G (IgG) virus nucleocapsid protein antibodies in serum.
Participant Characteristics
Participant's age and duration of breastfeeding at the time of the second dose of vaccine.
BMI at the time of screening = weight (kg)/height (m2).
Cancer, chemotherapy, immunomodulators, radiotherapy, immunosuppressants, or corticosteroids (e.g., >20 mg/day of prednisone or equivalent) for >14 days in the past 6 months, or immunoglobulins in the past 3 months.
Exclusive breastfeeding was defined as breast milk only, without any other liquids or solids; partial breastfeeding was defined as breast milk in combination with other liquids or infant formula; breastfeeding with complementary feeding was defined as breast milk in combination with other liquids and solid food.
BMI, body mass index; CPAP, continuous positive airway pressure; IQR, interquartile range; SD, standard deviation.
From February 2 to May 4, 2021, 100 participants were recruited and 95 of them with their 97 infants were included in the final analysis. Five were excluded, one for COVID-19 symptoms at the time of vaccination, two for past SARS-CoV-2 infection, and two for presenting serum parameters suggestive of past COVID-19 infection (Fig. 1).
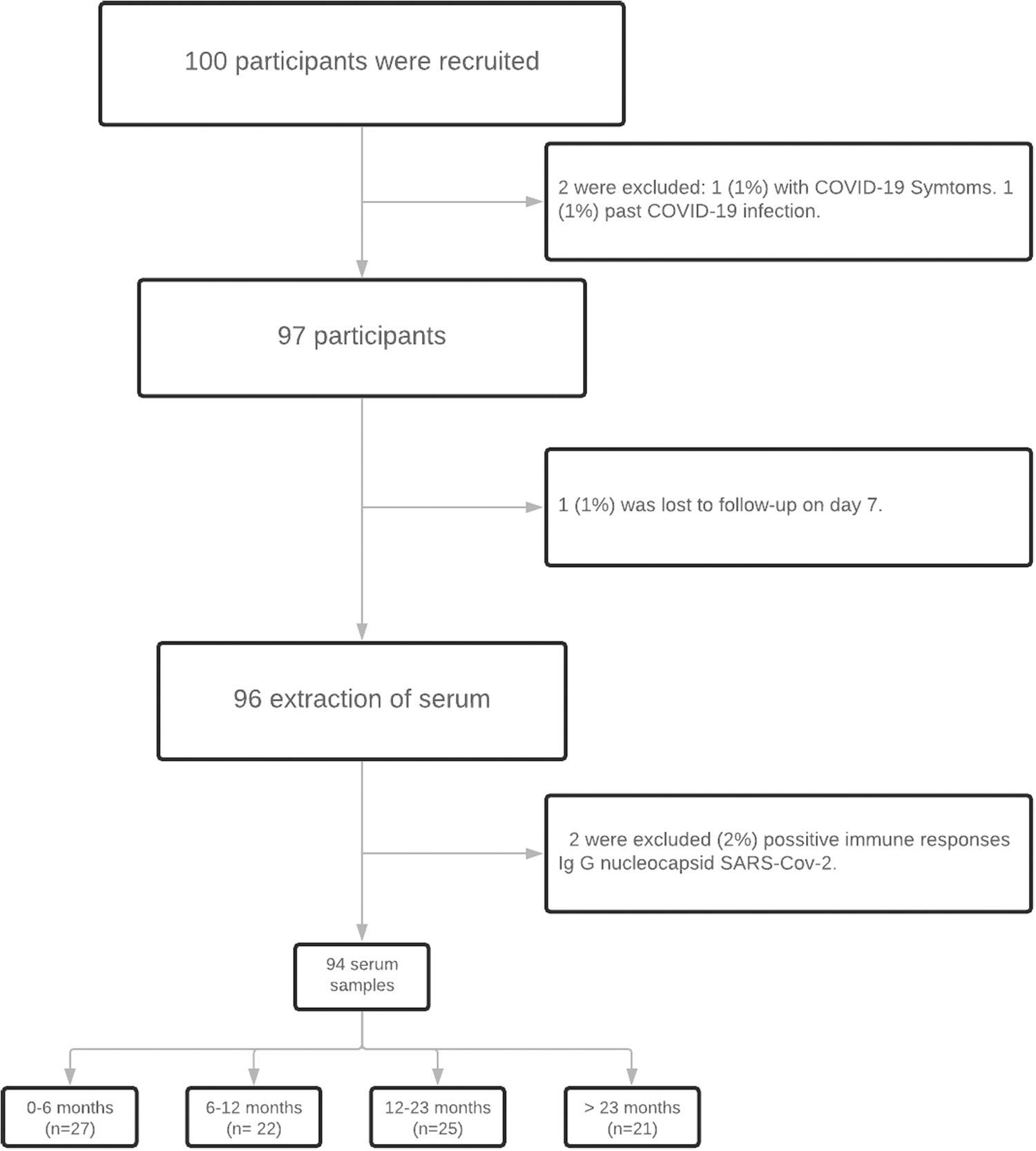
Participant enrollment.
Data and sample collection
Symptom follow-up questionnaires were made available daily to the mothers throughout the 14-day study period. In the first 2 days, a telephone survey was performed; subsequently, participants used a Google form questionnaire. These questionnaires were completed by 96% of the participants on a daily basis throughout the 14 days follow-up.
Solicited local and systemic reactions and their severity were recorded in mothers and their breastfed infants. Adverse reactions were classified as mild when not interfering with daily life activities, moderate when interfering with these activities, and severe when daily life activities had to be abandoned. To obtain a cumulative severity score, the scores 1 for mild, 2 for moderate, and 3 for severe adverse reactions were designated. The final cumulative score consisted of the sum of the individual scores assigned to each symptom that occurred within 2 weeks after the second dose of vaccine.
Unsolicited symptoms, adverse events of special interest, medication for symptom relief, emergency room visits, and hospital admissions of mothers and their infants were recorded as well.
Blood analyses
Maternal blood extraction was scheduled on day 14 after the second dose of vaccine to determinate humoral immune response with IgG, and IgM antibody production against its S1 subunit and IgG against the SARS-CoV-2 nucleocapsid protein.
Vaccines against COVID-19 introduce information from the SARS-CoV-2 spike glycoprotein receptor-binding domain (RBD) and generate a humoral immune response with IgA, IgG, and IgM antibody production against the virus S1 subunit with its binding region for human cells. They do not generate antibodies against the SARS-CoV-2 nucleocapsid protein (anti-SARS-CoV-2 N IgG), which solely appear in infected patients and those who have had the disease.
IgG antibodies against the receptor-binding spike domain S1 subunit (anti-SARS-CoV-2 RBD-S1 IgG) were determined with the SARS-CoV-2 IgG II Quant Abbott® assay and results are expressed as international standard units (unit of 1,000 binding antibody units [BAU] per mL). 11 The SARS-CoV-2 IgG Architect Abbott® assay was used for anti-SARS-CoV-2 N IgG and anti-SARS-CoV-2 S1 IgM detection. By default, data for both assays are expressed as qualitative “positive” or “negative” results.
Safety
Our main objective was to evaluate the safety of COVID-19 vaccination in mothers and their breastfeeding infants. We expected a similar proportion of adverse events as described for the population from 18 to 55 years in clinical trials, that is, <1% of serious adverse events in vaccinated women and no serious adverse effects in their breastfed children. The adverse reactions were reported to the health authorities.
The study was approved by the institutional review board.
Statistical analysis
Quantitative data were given as mean ± standard deviation or median with interquartile ranges. Qualitative data were treated by analyzing absolute as well as relative frequencies. A 95% confidence interval (CI) was used. To compare differences in means, normally distributed variables were analyzed using the Student's t test, whereas the nonparametric Mann–Whitney U test was used for not normally distributed data. The chi-square test was applied for qualitative normally distributed variables. Pearson's correlation coefficient (r) was used to contrast correlations of continuous variables. Statistical significance was set at p < 0.05.
All statistical analyses were performed using the R package (R Foundation for Statistical Computing, Vienna, Austria), version 4.0.5.
Line charts with CIs and area charts were used to represent the proportion of the mothers' and their breastfed infants' reaction severity-dependent symptoms. A box-and-whisker plot was used to plot symptom groups in relation to their mean antibody levels produced after vaccination.
Results
Adverse effects in breastfeeding mothers
Epidemiological variables and risk factors for severe COVID-19 disease in mothers and infants are given in Table 1. Of the vaccinated study participants, 89 (94%) received the BNT162b2 mRNA COVID-19 vaccine and 6 (6%) the mRNA-1273 COVID-19 vaccine, with a mean time range between doses of 26 ± 2 to 28 ± 1 days. At least one adverse event during the 14-day follow-up after the second dose of vaccine was reported by 85% (95% CI: 76–91.5%) of the vaccinated individuals (Table 2). On day 1, 81% (95% CI: 72–88%) developed events. On day 4, the percentage dropped to 6% (95% CI: 2–13%) and by the end of follow-up the percentage dropped to 2% (95% CI: 2–7%). The chronological course of symptoms is depicted in Supplementary Figures S1 and S2.
Frequency of Local and Systemic Reactions Reported in the First 2 Weeks After mRNA COVID-19 Vaccination
Shown are solicited reactions, which the participants reported by means of a Google form questionnaire. The major severity level reported for each symptom was used.
CI, confidence interval.
The mothers reported a mean of 4 ± 3 reactions (95% CI: 3–4; Fig. 2) each. Approximately half of the vaccinated individuals had local and systemic symptoms (95% CI: 38–59%). The most frequent symptom was injection site pain (Supplementary Fig. S1), reported by 81% of the participants (95% CI: 72–89%). Local lymphadenopathy was described by 6% of the participants (95% CI: 2–14%).
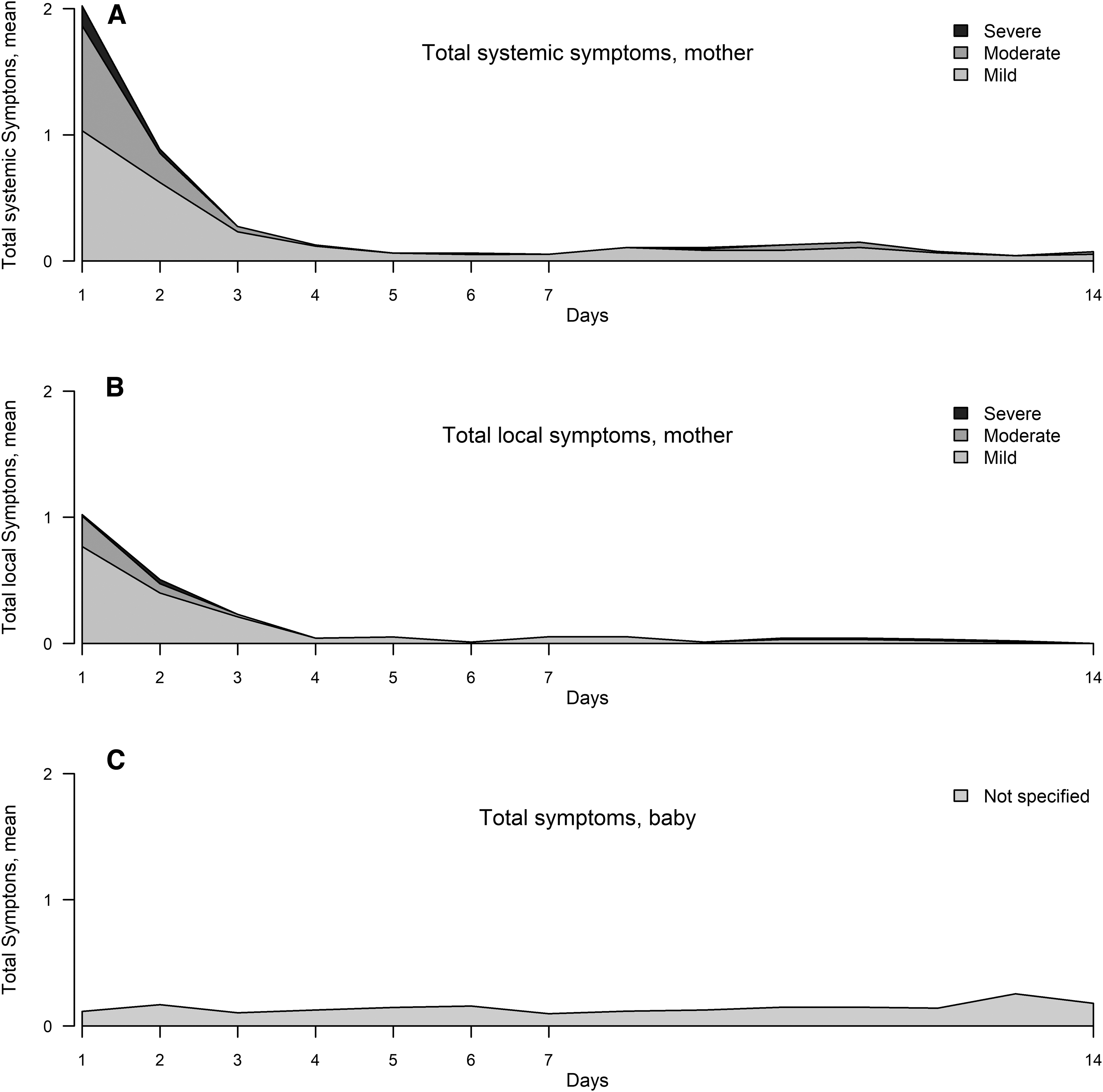
Area chart of solicited local and systemic adverse reactions in breastfeeding mothers and their infants, followed up from days 1 to 14 after second-dose SARS-CoV-2 vaccination. Reactions to mRNA-based vaccines were classified as mild (
The most frequent systemic symptoms (Supplementary Fig. S2) were fatigue and tiredness, which occurred in 49% of cases (95% CI: 38–59%), followed by myalgia, joint pain, or both in 53% of cases (95% CI: 42–64%). Headache was reported by 42% of the individuals (95% CI: 32–53%), 3% of whom had suffered severe pain (95% CI: 1–9%). Of all the events reported during follow-up, 70% were declared as mild and 3% as severe (Fig. 2). The mean severity score in the first 3 days was 5 ± 6. In 52% of the cases the value was <3 points.
The unsolicited adverse events consisted of one case of rash 8 hours after vaccination, three cases of axillary pain without lymphadenopathy, one case of pain in the breast accompanied by ipsilateral lymphadenopathy, three cases of local warming, one case of a sensation of heaviness in the arm, one reddish lesion on the breast, and one case of sore nipples. All these symptoms were temporary. One of the mothers was monitored for hyperglycemia after the first dose of vaccine.
In the course of follow-up, 70% (95% CI: 66–75%) of the mothers took short-term medication for relief, that is, for 1 (40%) or 2 days (22%) only (Supplementary Fig. S3).
No adverse event of special interest was declared, and there were neither visits to the emergency room nor hospital admissions as a result of vaccination. None of the mothers was diagnosed with COVID-19 during follow-up.
Symptoms in breastfed children
Some health event in their breastfed children (Table 2) was reported by 31% of the recently vaccinated mothers (95% CI: 22–41%). A mean of 1 ± 1 (95% CI: 0–1%) different symptoms were described throughout follow-up (Fig. 2). Most frequently, 19% (95% CI: 12–28%) children were irritable, 13% (95% CI: 7–21%) had a fever, 11% (95% CI: 6–19%) had cough, and 15% (95% CI: 9–24%) had nasal congestion at some point during follow-up (Fig. 3).

Line graph of symptoms in breastfed children reported from days 1 to 14 after second dose of mRNA-based SARS-CoV-2 vaccination. Reactions were ranked according to their frequency of occurrence (percentage of participants who reported the specified reaction). The top local event shown was irritability. The
Irritable children frequently exhibited concomitant symptoms, except for 5% (95% CI: 1–11%), in whom even this sole sign of discomfort resolved within 1 day. During the 14 days of follow-up, 36% of the children (95% CI: 27–46%) were diagnosed with respiratory infection (Supplementary Fig. S4), which was associated with fever (69%; p = 0.02) and declared cough (91%; p < 0.01). Thirty-seven percent of the participating children attended nursery or nursery school (95% CI: 37–63%), and 53% had siblings (95% CI: 37–63%).
We found a significant association between cough and respiratory infection in 22.2% of cases (relative risk 4.52; p = 0.02) and attending nursery (relative risk 2.87; 95% CI: 1.66–4.96%; p < 0.001). Nonetheless, we did not find a significant association between respiratory symptoms and having siblings (relative risk 1.6; 95% CI: −0.9 to 2.88%; p = 0.09), although these symptoms were more frequent in children with a school-age sibling. Sleepiness and fatigue in the breastfed infant were only reported in boys and girls without siblings.
We did not find any association between maternal adverse events and the symptoms described in the infants.
Also, as to the course of symptoms observed in the breastfed infants (Fig. 2), we did not detect any differences during follow-up.
Within the symptoms, fever was observed most frequently on day 9 (three children) and cough on days 5 and 6 (five children). Irritability was found in six children on days 1, 2, and 13, but without significant difference to the other days. Sleepiness was described by one participant throughout follow-up period. Breast rejection on day 1was described by two mothers and on days 2 and 3 of follow-up by one mother (Fig. 3).
In the course of the study, diagnostic tests for COVID-19 were performed in five infants (two SARS-CoV-2 antigen and three PCR tests) and resulted negative. A gastrointestinal infection with Campylobacter yeyuni and bronchitis due to rhinovirus were diagnosed in one case each. Throughout the study period, five visits to the emergency room due to intercurrent infections were recorded. None of the infants needed hospital admission.
Immunogenicity
We detected anti-SARS-CoV-2 N IgG antibodies in two participants, who were, therefore, excluded for previous SARS-CoV-2 infection. Only one participant was lost to follow-up on day 7 and, therefore, her tests were not performed.
All 94 included participants generated antibodies with titers >560.9 BAU/mL, which, according to the manufacturer of the applied test, correspond to a neutralizing capacity. The median anti-SARS-CoV-2 RBD-S1 IgG antibody concentration (antibodies against the S1 subunit of the SARS-CoV-2 spike glycoprotein RBD) in vaccinated participants was 3,391 ± 1,634 BAU/mL (95% CI: 3,051–3,732%). On day 14 after vaccination, 23% of the samples (95% CI: 14–33%) were positive for SARS-CoV-2-S1 IgM antibodies.
We did not find any correlation between serum antibody levels and maternal age, BMI, or breastfeeding period, nor was there an association with symptoms in the breastfed children (p = 0.47). We observed a significantly positive correlation between the total score of symptoms in the first 2 weeks past vaccination and the specific antibody levels in blood (r 0.25; 95% CI: 0.36–0.42%; p = 0.02). Also, systemic and local symptoms within the first 3 days after the second dose of vaccine were significantly associated (p < 0.01) with increased IgG antibody levels in blood (Fig. 4). Participants taking medication also had higher antibody levels (p = 0.01).

Box and whisker plots of SARS-CoV-2 RBD-S1 IgG distribution according to solicited local or systemic reactions and medication for relief in the first 3 days. The four represented groups were assigned as no events, local, systemic, or local and systemic events.
Discussion
In our sample of breastfeeding mothers, we observed a safety profile similar to that described in other recently studied populations 12 and in clinical trials of the mRNA vaccines used in our study.4,5 The limited convenience sample size we worked with is not ideal to draw conclusions on vaccine safety, but the fact that our CIs coincide with those in clinical trials and other population studies makes us consider our data valid information on this subgroup. We observed frequent mothers' adverse events, which commonly consisted of local and systemic symptoms during follow-up, but most of them were mild and did not interfere with the participants' daily life activities.
The most frequent symptoms were (local) injection site pain and (systemic) fatigue, tiredness, or both. Axillary symptoms were described by nine participants; one of them described pain radiating into the breast. The proportion of these symptoms was higher than described in the clinical trials for the Pfizer vaccine (0.9%) 13 and similar to those reported for the Moderna trials. 5 The incidence declared in the registries of adverse events, such as the Spanish drug surveillance system, also resembles ours. In our study, medication for symptom relief was used timely limited and with a similar frequency compared with others large prospective observational studies.
We did not observe adverse reactions requiring special surveillance, emergency room attendance, or hospital admission. However, there was a statistically significant difference between antibody levels in serum of participants with systemic or local symptoms and those without adverse reactions. The clinical relevance of this point will have to be defined in the future, as the immunological correlation with protection is currently under study.14–16
This difference was also observed in participants who took medication for symptom relief. However, we cannot differentiate between the impact of medication versus degree of symptoms on serum antibody levels, as most individuals who took medication suffered a combination of local and systemic symptoms (Fig. 4).
Assessing adverse reactions in breastfed infants is a contribution to resolving many mothers' concerns about possible vaccine effects in breastfed children at the time of vaccination. Although, after vaccination, 31% (95% CI: 22–41%) of the participating mothers observed health events in their infants, these cannot be considered adverse reactions due to the vaccine itself. The effects in the infants were nonspecific and without a clearly defined temporal association. We did not detect a notable peak on any particular day of follow-up, and many events were associated with concomitant infectious processes. Moreover, fever and declared cough were associated with respiratory infection.
In fact, to affect a breastfed child, a substance taken by the mother must either inhibit her milk production by inhibiting prolactin or fulfill each of the following steps: The substance must pass into the mother's blood, pass into her milk, persist there at considerable concentrations, pass to the infant, and also be harmful to the infant. 17 Only few drugs meet this profile.
We observed more events in these infants than described in other recent studies.18,19 However, this should be interpreted with caution, as our study was prospective with a relatively long follow-up period. Many of the reported events seemed to be related to concomitant infectious processes, which makes their occurrence more likely in the course of a prolonged follow-up.
We found isolated cases of irritability in 5% of the children, as well as breast rejection in 4% (95% CI: 1–10%) on days 1 and 2 after vaccination in two and one patient, respectively (Fig. 3). As postulated in other studies, these findings could be related to changes in milk production. 19 However, although the daily milk volume was not assessed in our study, no mother reported a negative effect on breastfeeding. In accordance with Perl et al., 20 we observed symptoms of fever and respiratory infections in breastfed children after maternal vaccination.
It should be pointed that children from newborn to 3 years of age have a median of 14 multiple episodes of infection. Overcrowded nurseries and the contact with older siblings have been associated with the incidence of respiratory infections. 21 In our study, 36% of the infants suffered respiratory infections most likely not related to vaccination. In the Spanish sentinel network, an increase in respiratory infections was recorded in children from newborn to 4 years of age between the weeks 3 and 17 of this year, overlapping with the period in which our study population was enrolled. None of the participants, neither children nor their mothers, was diagnosed with COVID-19 at the time of our study.
Strengths and Limitations
The fundamental strength of our study is the strong participant adherence. We only lost one participant during follow-up, and received reliable daily records from the rest during the first 2 weeks postvaccination.
However, this study has some limitations. The absence of an adequate control group prevented comparison of symptoms between infants of unvaccinated and vaccinated mothers. Moreover, the study did not include analytical studies in the infants.
Conclusion
We believe that informing of possible adverse events, adverse reactions, and contraindications is an essential aspect of vaccination. Knowing that mothers' reactions are mostly mild and transitory, in most cases limited to 3 days after vaccination, helps to lessen fear of the unknown and increases confidence in vaccination. The CIs of our results lie within the data published in clinical trials and population series,5,12,13,22 which suggests that the COVID-19 vaccine safety profiles for breastfeeding persons are very much like those for the general population.
Neither the mothers nor the infants suffered serious adverse events, and all the participating mothers would recommend vaccination after 1 month of follow-up. The adverse events observed in the infants seemed simply coincidental and not related to the vaccine itself. Because of the low incidence of reactions, a larger number of study participants would be needed to substantiate this assumption.
We believe that it is important and invite all breastfeeding mothers to declare all their reactions on vaccination. We urge pharmacovigilance systems to include women and infants as an interest group to be analyzed separately. This is the only way to obtain sufficient evidence and to be able to safely report vaccine effects in this population. Thus, recommendations against COVID-19 vaccination for breastfeeding women or, even worse, advice on weaning due to misinformation to prioritize vaccination can be avoided. We would like to remind the public that supporting breastfeeding beyond the infant's first months is a public health priority and that every mother has the right to decide when to wean her infant, without any psychological pressure that is based on a lack of appropriate research.
Article Summary
The mRNA COVID-19 vaccines in breastfeeding mothers have safety profile similar to that described in other studied populations.
What Is Known on This Subject
The COVID-19 mRNA vaccines appear safe in breastfeeding mothers.
What This Study Adds
This study provides daily information on the symptoms reported by the participants. It provides information on symptoms in infants after vaccination in a population of 95 mothers and 97 infants.
Footnotes
Acknowledgments
The authors express their gratitude to all the families who have participated in the study and have dedicated their time and effort providing this valuable.
Authors' Contributions
D.S.R.R. conceptualized and designed the study, as well as coordinated and supervised data collection. She drafted the initial article and revised the article. M.M.L.P. and M.C.P. coordinated and supervised data collection and revised the article. M.I.S.H. and A.M.F.V. drafted the initial article, conceptualized and designed the study, and revised the article. S.M.P., L.P.V., M.R.F., P.G.C., and B.R.M. designed the data collection instruments, collected data, and reviewed and revised the article. O.M.M.M. critically revised the article. S.R. translated and critically revised the article. M.Á.G.B. worked on statistical analysis, interpretation of data, and revised the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.