
Abstract
Background:
Black women encounter many challenges to breastfeeding, including inequitable access to support and resources and medical racism. However, limited research investigates how Black women across generations interface with health care systems to initiate or continue breastfeeding and what factors facilitate or hinder their breastfeeding experiences.
Objective:
Using the social determinants of health (SDoH) theoretical framework, this study qualitatively explored how a multigenerational sample of Black mothers' interactions with health care systems facilitated or hindered their breastfeeding initiation and continuation. There were three areas of interest: (1) access and quality, (2) professional and personal support, and (3) literacy and resources.
Materials and Methods:
Four age cohorts and three breastfeeding length cohorts of Black mothers in Kentucky completed semi-structured interviews on their breastfeeding experiences. Responses to research questions (e.g., “What was your experience during the birthing process and how did it impact your decision to breastfeed?”) informed by the SDoH were analyzed using thematic analysis.
Results:
Four themes emerged on how experiences within health care systems influence Black women's breastfeeding initiation and continuation: (1) health care access, (2) health care quality/bias, (3) health care-related support, and (4) health care resource use.
Conclusions:
Interpersonal and systemic barriers in health care related to access, quality, support, and resources hindered Black mother's breastfeeding across generations. Mothers across each age and breastfeeding cohorts emphasized a need for culturally tailored pro-breastfeeding health care systems to meet their breastfeeding needs.
Introduction
Health care determinants of breastfeeding among black women in kentucky
Black women report the lowest rates of breastfeeding initiation, continuation, and exclusivity compared with women of all other racial and ethnic groups. 1 In Kentucky, these numbers are striking, as 37% of Black mothers initiate breastfeeding compared with 65% of White mothers. 2 Despite the benefits of breastfeeding for reducing the development of chronic health problems such as obesity, diabetes, and cardiovascular disease, 3 Black women are less likely to receive these benefits compared with other women due to breastfeeding barriers, such as inequities in the access and quality of breastfeeding support and resources within the health care system. 4
Social determinants of health (SDoH) theory suggests that health and health care may be modifiable determinants of breastfeeding. 5 For example, research indicates that access to primary and specialized health care increases the likelihood of breastfeeding initiation and continuation. 6 However, for Black women, access is one step in a sequential line of health care determinants for breastfeeding decisions. Once health care is accessed, the variance in quality of care, including inequitable treatment from health care providers, is a prime area for systemic intervention. 7 Although Black women's experiences within health care systems for birth and breastfeeding have been studied,8,9 there is a need to specifically understand how Black women in Kentucky interact with health care providers, policies, and practices regarding breastfeeding.
The present study qualitatively explores how a multigenerational sample of Black women in Kentucky accessed and navigated health care systems to initiate and sustain breastfeeding. Considering the history and current reality of medical racism in health care, 10 more studies providing a multigenerational perspective on breastfeeding and health care support among Black women are warranted. 11 Thus, the current study fills a gap in the literature by using the SDoH as a guiding framework to better understand the interface between health care systems and breastfeeding practice among Black mothers living in Kentucky, a group with one of the lowest breastfeeding rates in the United States.
We present a model derived from Black women's lived experiences of how their engagement in the health care system related to three areas: (1) access and quality; (2) professional and personal support; and (3) literacy and resources facilitated and hindered their breastfeeding. Findings from this study can inform health care policies and practices to improve breastfeeding outcomes among Black mothers.
Materials and Methods
Participants and procedures
Participants were recruited from summer to fall 2020 as a part of the pilot study, Support Peers for Breastfeeding Expansion among African American Kentuckians (SPEAK) study. The purpose of the SPEAK study was to determine generational and cultural messages about breastfeeding among African American women in Kentucky. Participants were recruited through convenience sampling using social media posts, word-of-mouth, and email listservs for organizations that serve Black women. Eligible participants were (1) mothers; (2) older than 18 years; (3) identified as African American/Black; (4) lived in Kentucky; (5) and were willing to discuss their experiences regarding breastfeeding via Zoom.
A multigenerational sample of 37 participants was recruited across four age cohorts (18–29, 30–45, 46–60, and older than 60 years) and three breastfeeding cohorts (breastfed less than 6 months, breastfed more than 6 months, never breastfed) (Table 1). Interested participants provided verbal consent and completed 45- to 60-minute semi-structured interviews on their breastfeeding decisions and experiences.
Participant Cohorts by Age and Breastfeeding Duration
Individual interviews were conducted via HIPAA-compliant Zoom, audio-recorded, and transcribed by a third-party company. A team of six Black women—three doctoral students, a postdoctoral fellow, and two associate professors—interested in Black maternal health conducted interviews with participants. Only two of the interviewers were mothers. Both previously breastfed their children and one (the principal investigator) is a certified lactation consultant. Participants received a $20 gift card.
Participants were asked several questions about their experiences with health care and medical providers including: “Did you use a physician, doula, midwife or other maternity care provider during your birthing process?” “What was your experience during the birthing process and how did it impact your decision to breastfeed?” “What are the main reasons you think Black women do not breastfeed?” “What other support systems did you have when you breastfed (e.g., community support groups, lactation consultations, doulas, childbirth classes, internet, etc.)?” and “What do Black women need to see or hear to encourage them to breastfeed?” All participants answered the interview questions posed.
Participants' ages ranged from 23 to 77 years with a mean of 45.27 (standard deviation = 16.15) years. They had between one and four children. All participants identified as heterosexual. Many women earned graduate/professional degrees (n = 16; 43.2%) and were currently employed full time (n = 21; 56.8%). Some were married (n = 12; 23.4%), but more were single/never married (n = 14; 37.8%). Most reported their income did not influence their decision to breastfeed (n = 21; 83.8%) (Table 2). This study was approved by the university's institutional review board.
Participant Demographics (N = 37)
M, mean; SD, standard deviation.
Data analysis
This study employed thematic analysis of existing data.12,13 Transcripts were hand-coded by the entire team, where all members familiarized themselves with the entire data corpus. Each team member coded three to four interview transcripts and reflexively memoed throughout the coding process. Team members added semantic and latent codes to the codebook, and the definitions of the codes were updated as we read through the entire data corpus. Semantic codes summarize the content of the data, whereas latent codes are based on researcher interpretations. Last, a smaller team of four women conducted focused coding on the transcripts, using the SDoH model. 14
Researchers created themes under each determinant and selected salient quotes to finalize themes and subthemes. We established rigor and trustworthiness of our study through the following methods: (1) researcher reflexivity, (2) prolonged engagement with data, (3) interviewer memoing, (4) team-based coding and analysis, and (5) purposive sampling.
Results
Four themes based on the SDoH model emerged from the interviews. The themes captured how health and health care influenced Black women's breastfeeding. Themes were as follows: (1) health care access, (2) health care quality/bias, (3) health care-related support, and (4) health care resource use. Figure 1 provides a description of how participants sequentially interacted with the health care system to initiate and continue or cease breastfeeding.
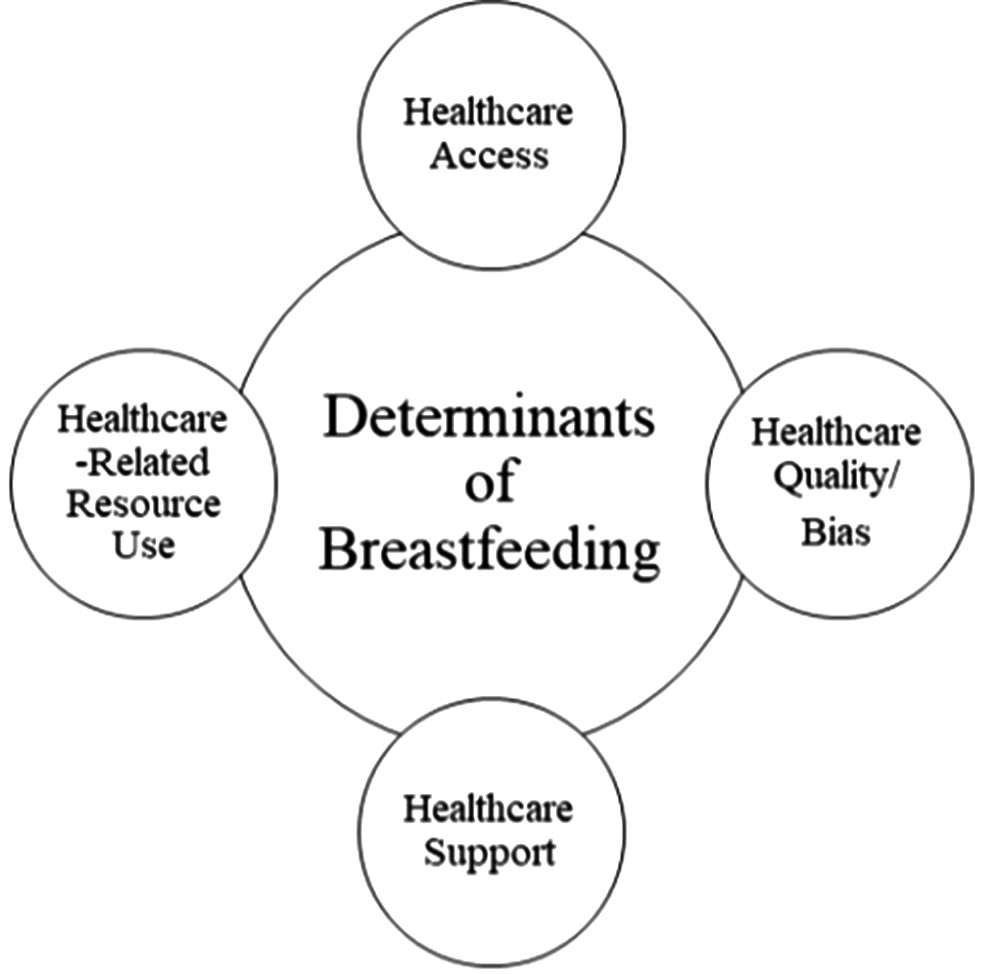
Health care determinants of breastfeeding among Black women in Kentucky.
Health care access
Health care access represented how readily available health care resources and supports were to mothers. Health care access suggested that mothers had the ability, right, and/or choice to approach, enter, get, use, or benefit from health care resources that could facilitate or hinder breastfeeding. Some mothers accessed health or primary care professionals to assist with breastfeeding. Toni (23) shared “I had a doula and a midwife.” Celia (40) stated, “I did the lactation consultants, and I did the breastfeeding classes at the hospital.” Other mothers had access to a combination of health care resources such as Lauren (36), who reported having a lactation consultant and using her knowledge as a doula to initiate and continue breastfeeding.
Some hospitals provided a lactation consultant to mothers immediately postpartum. For example, Olivia (36) shared, “the lactation consultant visited me in the hospital. And they encouraged me to pump.” Other mothers learned about breastfeeding briefly from nurses when lactation specialists were not available. Without a lactation consultant, struggles such as inverted nipples hindered successful latching and impacted breastfeeding initiation. Doriah (30) said, “I needed a lactation specialist […] I think I talked to maybe two nurses or asked them about being able to do that, especially just getting a breast pump. They didn't have any breast pumps there. I was like, how y'all have no breast pumps? You know what they did have? They did have formula.” Ultimately, lack of access to a lactation specialist prevented Doriah from successful breastfeeding initiation.
Another access deterrent was participants' low-income status. For example, Terry (68) said, “depending on your financial situation, like the person I was talking about who went back after a month, I mean that person works a low-income, probably a little bit over minimum wage-type job and could not financially afford to be off for a long time [to breastfeed].”
Low-income status prevented some participants from having access to breastfeeding resources. Specifically, participants reported their providers encouraged and offered access to free formula provided by Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), rather than resources about or assistance with breastfeeding, prompting them to forgo breastfeeding. For example, as a low-income teenage mother, Cara (43) received access to a free program that introduced breastfeeding but emphasized using formula through WIC services.
Health care quality/bias
Health care quality/bias represented the standard of care received by mothers once they accessed health care. Reports of inadequate health care, including providers' anti-Black discrimination practices, deterred some participants from breastfeeding. Of note, the experience of anti-Black discrimination practices was evident across age cohorts.
For example, Terry (68) said, “I knew one young lady who was in the hospital, had her baby. She was not married to the child's father, and they tried to get her to apply for WIC and all that kind of stuff.” Rochelle (60) said, “And then not having physicians who even talk to you about the option of breastfeeding and having you consider it. If I had not said that I wanted to breastfeed, I'm wondering if they just would have started her on formula without even asking me or telling me that there were other options.” Sabrina (25) added, “And that's one thing that the doctors or anyone … They didn't tell me about that [breastfeeding]. I think I had to Google that.”
Terry, Rochelle, and Sabrina implied stereotypes such as Black women may not want to learn about breastfeeding or single Black mothers are all on public assistance may have informed health care providers' failure to introduce breastfeeding as an option.
Toni (23) said, “I feel like the white race, gets better treatment than us African-Americans, especially when it comes to birth and stuff like that. I think if she [lactation consultant] would've sat down with me, talked through it a little bit, latched the baby on herself maybe. Went through a lot more than what she did with the experience she got.” Across generational cohorts, mothers seemed to experience poor health care quality attributed to anti-Black discrimination, and as referenced by Toni, noticeable favoritism toward White mothers.
Many mothers had traumatic birth experiences or interactions with health care systems that hindered their breastfeeding. Patti (64) said, “I never asked for anything. I just suffered through whatever I had to suffer through until the day nurse came on because you've got to remember if you all think Black Lives Matter is bad now. Go back 40 years.”
Quality healthcare facilitated their breastfeeding initiation and continuation. Components of quality health care were resourcefulness, support, reliability, and availability. Jan (37) stated, “The follow-up lactation consultant was very good. The lactation consultant was helpful in helping me get the pump, and she did try to get her to latch on.” Josephine (34) discussed how reliable and available her doula was in sharing, “I called her like every five minutes when I was in hospital.” Jan and Josephine breastfed for less than 6 months. However, because they received quality and bias-free health care, they discontinued breastfeeding knowing their decisions were not informed by stereotypes or inadequate care that deter breastfeeding initiation in the first place or make them think a decision has been made for them.
Health care-related support
Health care-related support emerged as individualized ongoing care, advice, consultations, or check-ins from physicians, doulas, lactation consultants, or other medically trained professionals that decreased challenges to breastfeeding. For example, Ebony (55) shared, “I had a very caring doctor, which made the process easier for me.” Lauren (36) stated, “I need more hands-on support. I can't just read it and try and figure it out. So, I think that's where the lactation consultant really came in and helped a whole lot for me.” Health care support provided early encouraged participants to initiate breastfeeding. For example, Michelle (30) said, “the support was really the deciding factor.” Continuation support helped mothers persist in breastfeeding. Josephine (34) shared how her lactation consultant provided continuation support:
She followed up with me. I could tell, but she wanted me not to give up. I kept pumping and pumping and pumping and nothing was coming out. And so, I think more than anything, just navigating through my frustration. So, she came to my room two or three times to help me with pumping and just calm my nerves of why it wasn't happening the way I wanted it to.
When health care providers supported mothers with ongoing care, consultations, or check-ins, mothers reported more motivation to initiate breastfeeding and less challenges related to breastfeeding continuation.
Health care resource use
Health care resource use described how mothers used health care resources accessible to them. Representation and quality informed health care resource use. Regarding resource representation, Black women desired more representation of Black women in the health care resources. Resources, such as pamphlet images, were predominantly oriented toward White people, specifically White women. Aaliyah said, “You don't get a lot of attention on how Black women should breastfeed. I don't see that a lot. I would see Caucasian women.” The overrepresentation of White women among health care resources was another form of racism mothers encountered. Mothers reported that more Black resource representation would increase comfort, decrease discriminatory experiences, and encourage more questions about breastfeeding.
For example, Lauren (36) shared, “if you see someone doing something who looks like you, you can relate a little bit more. That gives me someone who I can ask questions to, to help me understand what's going on.” Quality resources were defined as readily accessible to mothers, supportive, and representative of Black women. Olivia (36) disclosed how lactation consultants were immediately available to her following her child's birth, “they [providers] talked about, ‘We have a lactation consultant here,’ and ‘We will come to the hospital; we will schedule a time to come in. Bring your baby in,’ so I was all gun-ho to do that to make sure he was latching on right, and all the things.” Frequent and consistent health care resource use led to breastfeeding continuation rather than cessation.
Discussion
The current study explored how health care influences four generations of Black women's breastfeeding experiences in Kentucky. Four themes emerged from the interviews based on the SDoH: (1) health care access, (2) health care quality/bias, (3) health care support, and (4) health care-related resource use. Our findings suggest across age cohorts and birth experiences, Black women encounter barriers and facilitators to breastfeeding in health and health care systems during initiation or continuation of breastfeeding.
Furthermore, the barriers and facilitators to breastfeeding are informed by cultural preferences (e.g., desiring Black mothers in the resources) and gendered racism in health care systems, 14 ultimately influencing the way they navigate the health care system and their breastfeeding experiences. As it relates to generational differences, the former two determinants were not reportedly experienced differently; however, the latter two determinants were, in those women who breastfed more recently had access to more health care supports (e.g., lactation consultants) and resources (e.g., breast pumps).
Social determinants of health
SDoH posits the interactions between the “places where people live, learn, work, and play affect health risks and outcomes.” 15 Within the health and health care component, the relationship between access to health care and health literacy can influence one's breastfeeding experiences. 15 However, racism and sexism that undergird inequitable and inconsistent treatment in the U.S. health care system adversely impact the health of Black women and their infants, despite generation.
Health care access was a determinant and deterrent of breastfeeding among Black mothers. Accessible health care consists of insurance coverage, geographically accessible health care services, and timely access to health care. 6 When mothers could access all three components of accessible health care, they reported more positive experiences related to breastfeeding and longer breastfeeding duration. However, when mothers could not access health care resources, health care access was identified as a deterrent to breastfeeding. For example, having a low-income background, rather than generation, emerged as a barrier to access health care.
With increased socioeconomic resources, Black women may seek medical providers who can help them understand their health and health service options. Additionally, accessing a continuity of care from prenatal to postpartum can help Black women receive high-quality health care while also increasing the likelihood of breastfeeding. 16
Our second theme of health care quality/bias indicates that these Black mothers experienced barriers to quality health care on a systemic and interpersonal level. On a systemic level, mothers across generations reported receiving inadequate health care when providers withheld breastfeeding information and resources. Our results are substantiated by research reporting a limited number of hospitals in the Southern United States are baby-friendly and support hospital-based breastfeeding initiatives. 17
The most recent CDC Breastfeeding Report Card reported Kentucky hospitals were ranked among the lowest in the nation when assessing maternity practices in infant nutrition and care among hospitals in the United States. 16 Kentucky's low rankings suggest a deficit in hospital-based efforts to implement policies and practices that promote ideal breastfeeding practices and provide quality care to new mothers.
On an interpersonal level, mothers shared experiences with health care providers' anti-Black discrimination practices that resulted in unacceptable treatment and self-reported trauma. Specifically, older participants reflected more on traumatic experiences with childbirth and breastfeeding, but younger participants also noted discrimination despite reporting more health care support. 18
Older Black women's breastfeeding experiences influence younger Black women's breastfeeding experiences through oral communication and feeding history. It is possible that women who had traumatic breastfeeding experiences may have been less likely to encourage breastfeeding among their children. 11
Furthermore, negative experiences with health care providers also account for low breastfeeding rates among Black women. 19 Navigating the health care system involves encountering gendered racial discrimination that influences Black women's quality of care. For example, Black women are nearly four times more likely to die from pregnancy-related complications than White women, and provider biases partially account for these disparities. 20 Training medical providers to engage Black women in culturally relevant and unbiased health care, such as presenting breastfeeding options to all Black women, may improve the quality of health care Black women receive and encourage more Black mothers to initiate breastfeeding.
An indicator of quality health care is perceived support. Several studies indicate that Black women desire breastfeeding information and support from their health care providers.20–22 In the current study, mothers who reported positive experiences with breastfeeding attributed persistence through breastfeeding challenges to the continued health care support they received from medical providers. These were predominantly mothers from younger generations. Additionally, mothers who reported consistent and ongoing support from their medical providers also reported fewer challenges related to breastfeeding continuation.
Conversely, mothers also expressed a desire to receive more support from health care providers in the form of ongoing care, advice, consultations, or check-ins. A lack of support can directly influence mothers' breastfeeding self-efficacy. 19 For these reasons, many Black women may desire culturally tailored care and support from pro-breastfeeding, Black health professionals such as lactation consultants.
Resources are a way in which breastfeeding information is disseminated to mothers and their support systems. Our final theme of health care-related resource use indicated younger mothers intentionally sought out breastfeeding information, including books, social media, and websites. These resources were nonexistent for the older generation. However, most mothers in this sample expressed a desire to see more Black women represented in breastfeeding resources.
Existing literature suggests that Black women may exhibit distrust of breastfeeding resources without culturally tailored information and representation. 23 Black mothers in the current study utilized breastfeeding resources when they were specific to Black women or when Black women were visually represented or acknowledged because they deemed them more credible. Ultimately, when Black women do not access breastfeeding resources, they limit their exposure to information that can increase their breastfeeding knowledge and community support. 23
Black women may exhibit mistrust of health care systems and professionals because of historical and current experiences of gendered, anti-Black racism and discrimination. For example, Black women faced exclusion from community organizations such as La Leche League, 8 which hindered their access to knowledge and support from breastfeeding communities. Despite new culturally tailored breastfeeding groups, including Georgia's Reaching Our Sisters Everywhere, Indiana's Black Breastfeeding Coalition, and Michigan's Black Mothers' Breastfeeding Association, 8 these organizations are geographically few and far between.
Many Black women without socioeconomic resources experience gaps in accessing and utilizing health information and services to initiate breastfeeding. Developing breastfeeding resources representing Black women and their breastfeeding experiences may increase interest to initiate breastfeeding and support to continue breastfeeding. 24 Additionally, increasing access to Black health care professionals, lactation consultants, and support groups may build trust with health care providers and ultimately foster Black mother's willingness to access and utilize breastfeeding resources.
Clinical implications
Our findings have meaningful implications for Black women who seek to breastfeed and are navigating the U.S. health care system. First, across age and breastfeeding cohorts, Black mothers desired more representation of Black women in breastfeeding resources and health care information. A way to increase breastfeeding literacy among Black women is to culturally tailor breastfeeding messages and images to meet their unique needs. 25 Second, mothers reported issues with timely access to health care to increase breastfeeding initiation. Similar to hospital peer navigation programs, 2 the development of hospital-based breastfeeding peer support programs can help develop community to provide breastfeeding education and support to Black mothers.
Additionally, family-centered approaches such as including Black mothers and grandmothers who have breastfed while providing education can increase breastfeeding literacy and support among Black women. 11 Last, Black women discussed needing to advocate for their rights to be informed of all breastfeeding options when interacting with health care providers. Our participants' experiences of retroactively learning how to breastfeed, without advice from their doctors, indicate a need to provide culturally tailored breastfeeding education to health care providers, including lactation consultants.
As many of our participants expressed a desire for more professional support, these training courses can also discuss the wanted support from health care providers to help initiate and sustain breastfeeding. Implementing health care practices specific to Black women can ensure that they receive optimal health care and avoid harm by a system intended to meet their health care needs.
Limitations and future directions
This study has a few limitations. First, due to the study's qualitative methodology and the location of interest being Kentucky, generalizability of breastfeeding experiences cannot be made across Black women living in other geographic U.S. regions. Future research should acquire samples from various U.S. locations to research Black women's breastfeeding experiences more broadly. Additionally, most of our sample identified as highly educated, middle-class Black women, which may have influenced women's experiences because higher education and socioeconomic status likely increases access to health care resources. Other studies should consider examining how intersecting identities (e.g., educational achievement and socioeconomic status) influence health care access and experiences among Black mothers who breastfed.
Furthermore, we did not complete member checking in our study protocol, thus limiting the transferability of our results. Future studies should consider including member checking to assess transferability and increase generalizability. Last, given the study was conducted during COVID-19, future studies should explore the impact of COVID-19 on Black mothers' breastfeeding initiation or continuation experiences, especially considering how COVID-19 disproportionately affected Black people.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the University of Kentucky Center for Health Equity Transformation (PI: Stevens-Watkins). The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the University of Kentucky.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.