
Abstract
Purpose:
Recently, maternal nutrient intake has been associated with human milk oligosaccharides (HMOs) composition. The goal of this study was to assess HMO composition in breast milk samples from vegan, vegetarian, and nonvegetarian lactating women. Second, we assessed impact of maternal body mass index (BMI), age, parity, and lactation stage on HMO composition.
Materials and Methods:
A cross-sectional analysis of HMO composition from vegan (n = 26), vegetarian (n = 22), and nonvegetarian (n = 26) lactating women was carried out. The majority of participants took dietary supplements.
Results:
In an unadjusted bivariate model, there was no difference in individual HMO composition, total HMO-bound fucose and HMO-bound sialic acid, or diversity and evenness scores by diet group. When adjusting for factors that significantly differed between groups (maternal BMI and lactation stage), no differences in HMO composition were observed. Secretor status was significant for 13 of the outcome variables with the strongest positive relationship with total HMO (β = 0.922) and HMO-bound fucose (β = 0.910), and the strongest negative relationship with sialyl-lacto-N-tetraose b (LSTb) (β = −0.544). Lactation stage was significant for eight analytes, with the strongest positive impact on 3′sialyllactose (3′SL) (β = 0.433), and the strongest negative impact on 6′sialyllactose (6′SL) (β = −0.519). Maternal BMI had a significant positive relationship with total HMO composition (β = 0.113) and 3′SL (β = 0.325).
Conclusions:
Lactating women who consume plant-based diets do not produce different breast milk as it relates to HMO composition.
Introduction
Human milk oligosaccharides (HMOs) are nondigestible carbohydrates found in human milk, where they are the third most abundant constituent after lactose and lipids. 1 HMOs can be categorized as nonfucosylated/nonsialylated (neutral), fucosylated/nonsialylated (neutral), nonfucosylated/sialylated (acidic), or fucosylated/sialylated (acidic), according to their structural composition.2,3 Several factors have been associated with HMO composition, including genetics, geographical location, lactation stage, and gestational age.3–8 HMO composition has been linked to various health benefits that may be mediated by the development of a beneficial gut microbiome, including protection against infectious pathogens, reduction in inflammatory illnesses, such as food allergies, asthma, and necrotizing enterocolitis.2,8–11 HMOs promote infant health through their prebiotic, antibacterial, and antiviral effects, but may also have direct effects on infant's development, independent of the microbiome.2,12
Limited number of previous studies has shown an association between maternal diet along with maternal nutritional status and breast milk composition of some nutrients.13–18 For example, when comparing the breast milk samples of mothers consuming a high-fat diet with those of mothers consuming a high-carbohydrate diet, the former exhibited significantly lower concentrations of sialylated acidic HMOs. 16 Quin et al. 19 found that maternal fruit intake was associated with several individual sulfonated HMOs in breast milk. These findings suggest that maternal diet patterns may exert an influence on the HMO composition of human milk. However, other studies did not find similar associations.20,21 Thus, the impact of maternal diet and maternal nutrient intake on HMO composition is not clear.
The objective of this study was to investigate HMO composition in vegan, vegetarian, and nonvegetarian lactating mothers. We hypothesized that there would be statistically significant differences in individual HMOs in samples collected from women adhering to different diet type. The analysis also included assessing the impact of other maternal factors including secretor status, body mass index (BMI), lactation stage, maternal age, and parity on HMO composition.
Materials and Methods
Recruitment and sample
The study was approved by the institutional review board (IRB) at the University of North Carolina at Greensboro (UNCG IRB 16-0310) and the University and Medical Center IRB at East Carolina University (UMCIRB 16-001726). Vegan and vegetarian organizations, breastfeeding support groups, and faith-based institutions were used as the primary source of recruitment. To determine eligibility, potential participants (n = 371) completed a basic online screening questionnaire (BSQ) that included questions about diet adherence and breastfeeding status. Inclusion criteria included residing in the United States, being 18–46 years old, giving birth to a healthy term infant (at least 2 weeks old at the time of milk sample collection/expression), willing to complete a diet survey, and willing to collect a breast milk sample in a manner that abided by the provided study collection protocol. Exclusion criteria included having a methylene tetrahydrofolate reductase (MTHFR) gene mutation diagnosis or other health conditions that affect vitamin B12 status, having hypo or hyperthyroidism, advanced liver disease, myeloproliferative disorders, or being pregnant. Once eligibility was determined through the BSQ, individuals were invited to participate in the study based on their self-reported diet type. Invited individuals (n = 142) were sent the IRB-approved consent form. The goal was to enroll ∼25 individuals from each diet group. Once we collected 74 milk samples, we informed others who were invited to participate that we have completed data collection. Recruitment and milk sample collection occurred between November of 2016 and April of 2017. Once milk samples were collected, participants received a $25 gift card.
Breast milk collection
Each participant was provided detailed instructions for collecting a single breast milk sample. Participants were instructed to collect the sample in the morning, during their first or second feeding of the day, and ≥2 hours since the previous feeding. They were told to collect the sample in a dimly lit room as means to protect the light-sensitive nutrients present in breast milk. Participants were instructed to completely express the content of one breast using the expression method of their choice. Expressed milk was to be transferred to a storage bag appropriate for freezing breast milk, labeled with the collection date, wrapped in aluminum foil for further protection, and stored in a home freezer until samples were collected or mailed to the laboratory at the University of North Carolina at Greensboro. The samples were either collected in-person or received in the mail by shipping it on dry ice to the laboratory. Participants also completed a digital survey with demographic, anthropometric, dietary, and supplement use information.
Diet classification
Vegans were defined as individuals who did not ingest any meat but may have ingested other animal products <1 time per month. Vegetarians were defined as individuals who did not eat meat but regularly ingested other animal products, such as eggs or dairy.
HMO analysis
Nineteen HMOs were analyzed. They included 2′fucosyllactose (2′FL), 3fucosyllactose (3FL), lacto-N-neotetraose (LNnT), 3′sialyllactose (3′SL), difucosyllactose (DFLac), 6′sialyllactose (6′SL), lacto-N-tetrose (LNT), lacto-N-fucopentoase I (LNFPI), lacto-N-fucopentoase II (LNFPII), lacto-N-fucopentoase III (LNFPIII), sialyl-lacto-N-tetraose b (LSTb), sialyl-lacto-N-tetraose c (LSTc), difucosyllacto-N-tetrose (DFLNT), lacto-N-hexaose (LNH), disialyllacto-N-tetraose (DSLNT), fucosyllacto-N-hexaose (FLNH), difucosyllacto-N-hexoase (DFLNH), fucodisiayllacto-N-hexaose (FDSLNH), and disialyllacto-N-hexaose (DSLNH).
HMO analysis was conducted at the University of California San Diego using established methods. 6 In brief, human milk (20 μL) was spiked with raffinose (a non-HMO carbohydrate) as an internal standard at the beginning of sample preparation to correct for sample losses during sample processing and allow for absolute oligosaccharide quantification. Oligosaccharides were extracted by high-throughput solid phase extraction over C18 (Hypercarb-96, 25 mg bed weight; Thermo Fisher Scientific, Waltham, MA) and Carbograph microcolumns (Hypersep-96 C18, 25 mg bed weight; Thermo Fisher Scientific) using a controlled vacuum manifold. Use of high-throughput microcolumns was validated in multiple different ways: (1) establishing parallelism in serial dilutions, (2) spiking milk with individual HMO standards to determine recovery, and (3) comparison with direct in-sample derivatization as used by others. 22 Oligosaccharides were fluorescently labeled with 2-aminobenzamide (2AB; Sigma-Aldrich, St. Louis, MO) in a 96-well thermocycler at 65°C for exactly 2 hours. The reaction was stopped abruptly by reducing the thermocycler temperature to 4°C. The amount of 2AB was titrated to be in excess to account for the high and variable amount of lactose and other glycans in milk samples. Unreacted 2AB was removed by high-throughput solid phase extraction over silica microcolumns (Hypersep silica, 25 mg bed weight; Thermo Fisher Scientific). Labeled oligosaccharides were analyzed by HPLC (Dionex Ultimate 3000; Dionex, now Thermo Fisher Scientific) on an amide-80 column (15 cm length, 2 mm inner diameter, 3 μm particle size; Tosoh Bioscience, Tokyo Japan) with a 50-mmol/L ammonium formate–acetonitrile buffer system. Separation was performed at 25°C and monitored with a fluorescence detector at 360 nm excitation and 425 nm emission. Peak annotation was based on standard retention times of commercially available HMO standards (Sigma, Dextra, Elicityl) and a synthetic HMO library 23 and offline mass spectrometric analysis on a Thermo LCQ Duo Ion trap mass spectrometer equipped with a Nano-ESI source. Absolute concentrations were calculated based on HMO standard response curves for each of the annotated HMO. (Oligosaccharide detection limit: ∼20 pmol, dynamic range between 20 and 5,000 pmol; milk samples were diluted accordingly.) The total concentration of HMOs was calculated as the sum of the annotated oligosaccharides. The proportion of each HMO making up the total HMO concentration was also calculated. HMO-bound fucose was calculated on a molar basis. One mole HMO with one fucose residue counted as 1 mole HMO-bound fucose whereas 1 mole HMO with two or more fucose residues counted as 2 or more moles of HMO-bound fucose. The same was calculated for HMO-bound sialic acid. Maternal secretor status was determined by the high abundance (>1,000 nmol/mL, secretor) or near absence (<100 nmol 2′FL/mL, nonsecretor) of the HMO 2′-fucosyllactose in the respective milk samples.
Statistical analysis
Descriptive statistics were calculated for numerical variables. Categorical variables including secretor status, education, and race were evaluated using a Fisher's test. Differences in HMOs by diet type were evaluated using ANOVA tests with a Tukey's adjustment for multiple comparisons. Because of the large number of outcome variables, a Bonferroni correction to the p-value was computed as 0.05/24 that resulted in a significance threshold of 0.002. A regression model was used to explore the role of secretor status, maternal BMI, lactation stage, maternal age, and parity on individual HMO composition. Results are reported as standardized β-coefficients. SAS Enterprise Software 9.4 (SAS Corporation, Cary, NC) was used for analysis.
Results
Seventy-four milk samples were collected and analyzed. Of these, 26 (35%) were from vegans (mean diet duration 6.2 years), 26 (35%) from nonvegetarians (mean diet duration 25.8 years), and 22 (30%) from vegetarians (mean diet duration 7.5 years). The majority (n = 63, 85%) of the milk samples were from participants who identified themselves as Caucasians, three samples (4%) were from Hispanics, one (1%) sample was from an Asian participant, and the remaining seven samples (9%) were from women of mixed decent. Seventy-eight percent (58/74) of participants took supplements containing B-vitamins, and 69% (51/74) were classified as secretors, with no difference between diet groups (p > 0.05). Demographic, anthropometric, and secretor characteristics of participants are found in Table 1. There were significant differences between diet groups for BMI, lactation state, and diet duration (p < 0.05).
Characteristics of Study Participants
Indicates means ± standard deviations. Data are evaluated for differences between groups using one-way ANOVA, and Tukey test was used for multiple comparisons. Groups with a common letter in the superscript are not significantly different.
Data represent n (%) and are evaluated for differences between groups using Fisher's exact test.
One subject in the vegan group and one subject in the vegetarian group had inconclusive secretor status.
BMI, body mass index; GED, general education dDiploma; HS, high school.
HMOs by diet type
A summary of HMOs by diet type is presented in Table 2. In an unadjusted bivariate model, there was no difference in individual HMO composition, total HMO-bound fucose, and HMO-bound sialic acid, or diversity and evenness scores by diet group. This finding also held true in a subanalysis of secretors (n = 17 per diet type). Our sample size of nonsecretors was too small (n = 4–9 per diet type) for a subanalysis of nonsecretors. When adjusting for differences between groups (maternal BMI and lactation stage), no differences in HMO composition were observed in the total sample (n = 74) or in a subanalysis of secretors (n = 51).
Summary of Human Milk Oligosaccharides by Maternal Diet Pattern
Data represent means ± standard deviation and are expressed in μg/mL unless otherwise noted. Significance at p < 0.002 using a Bonferroni correction due to multiple outcome variables. All p-values were >0.05 in an unadjusted model and when adjusting for BMI and lactation stage.
BMI, body mass index; DFLac, difucosyllactose; DFLNH, difucosyllacto-N-hexoase; DFLNT, difucosyllacto-N-tetrose; DSLNH, disialyllacto-N-hexaose; DSLNT, disialyllacto-N-tetraose; 3FL, 3fucosyllactose; FDSLNH, fucodisiayllacto-N-hexaose; FLNH, fucosyllacto-N-hexaose; HMO, human milk oligosaccharide; LNH, lacto-N-hexaose; LNT, lacto-N-tetrose; LNnT, lacto-N-neotetraose; LSTb, sialyl-lacto-N-tetraose b; LSTc, sialyl-lacto-N-tetraose c.
Maternal characteristics influencing HMO composition
Maternal characteristics including secretor status, BMI, lactation stage, age, and parity were probed for relationships with individual and total HMO composition. Results are presented in Table 3 as standardized β-coefficients (p-values). Secretor status was significant for 13 of the HMOs and had the strongest positive relationship with total HMO (β = 0.922, Fig 1), and total HMO-bound fucose (β = 0.910), and the strongest negative relationship with LNFPIII (β = −0.546). Lactation stage was significant for eight HMOs, with the strongest positive impact on 3′SL (β = 0.433), and the strongest negative impact on 6′SL (β = −0.519). Maternal BMI had a significant positive relationship with total HMOs (β = 0.113) and 3′SL (β = 0.325). Maternal age and parity were not significant predictor variables for any HMO analytes. Four HMO outcome variables (total HMO-bound sialic acid, DSLNT, LNH, and LNnT), and diversity and evenness were not influenced by any of the maternal factors in our model.
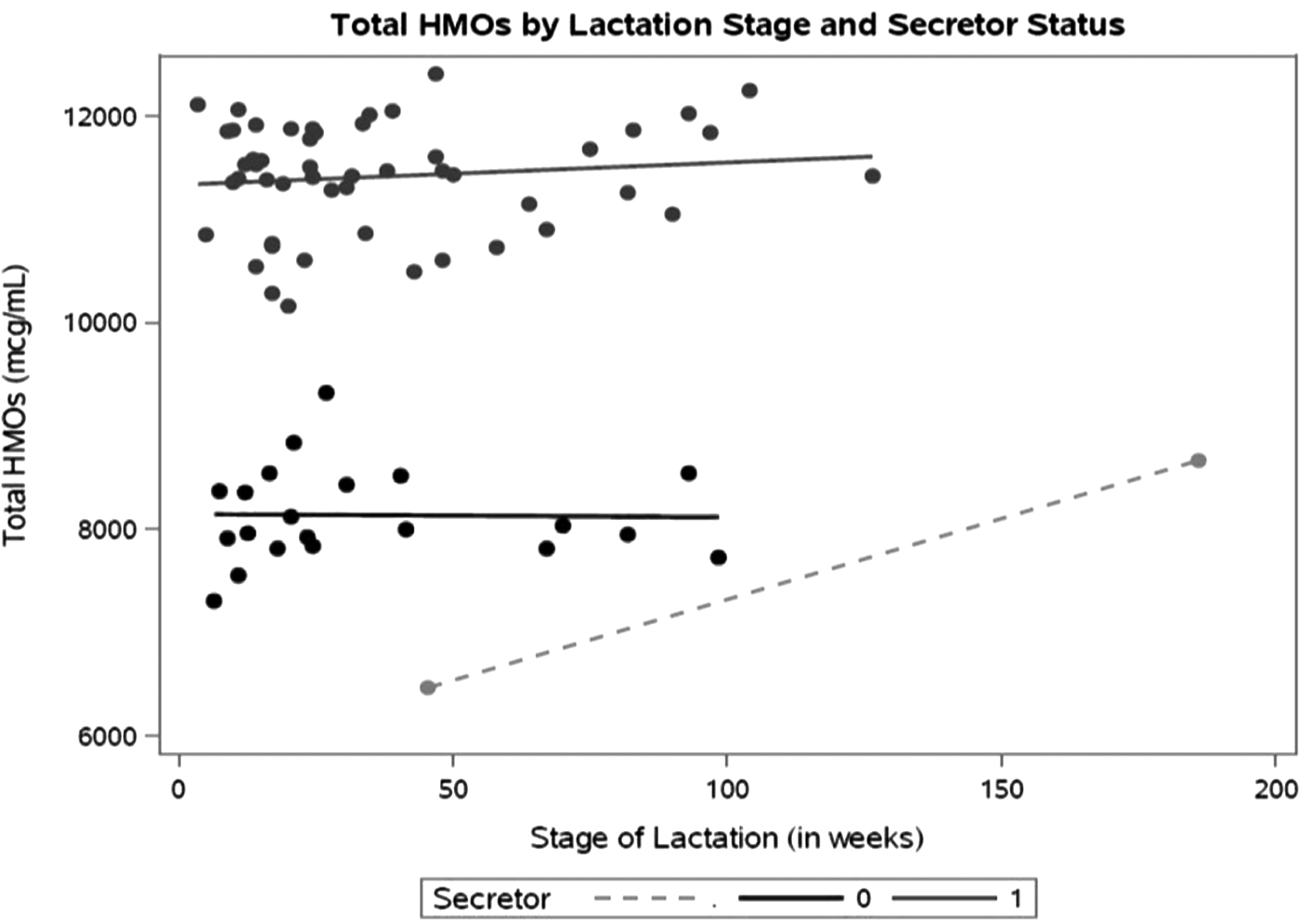
Total HMOs by secretor status and lactation stage (μg/mL). Total HMO concentrations were significantly lower in nonsecretors (
Maternal Factors Associated with Human Milk Oligosaccharides
Data represent standardized β-coefficients (p-values) in regression model using five predictor variables.
NS, not significant at p = 0.01 (adjusted for five predictor variables).
BMI, body mass index; DFLac, difucosyllactose; DFLNH, difucosyllacto-N-hexoase; DFLNT, difucosyllacto-N-tetrose; DSLNH, disialyllacto-N-hexaose; DSLNT, disialyllacto-N-tetraose; 3FL, 3fucosyllactose; FDSLNH, fucodisiayllacto-N-hexaose; FLNH, fucosyllacto-N-hexaose; HMO, human milk oligosaccharide; LNFPI, lacto-N-fucopentoase I; LNT, lacto-N-tetrose; LNH, lacto-N-hexaose; LNnT, lacto-N-neotetraose; LSTb, sialyl-lacto-N-tetraose b; LSTc, sialyl-lacto-N-tetraose c.
Discussion
There has been an increased interest in factors influencing HMO composition. Findings from previous studies have suggested that, along with genetics, mode of delivery, and geographical location, some dietary/nutritional factors may affect HMO profile.15–18 The primary aim of this study was to evaluate, for the first time to our knowledge, whether milk samples from vegan, vegetarian, and nonvegetarian lactating women differ with regard to HMO composition.
HMO and diet type
We did not find a statistically significant difference regarding total HMO composition among milk samples collected from vegan, vegetarian, and nonvegetarian women. In addition, we did not find a statistically significant difference in the 19 individual HMOs, total HMO-bound fucose, or sialic acid, from the respective diet groups (Table 2). This finding aligns with that reported by Azad et al. 21 They found that, in a sample of 427 Canadian breastfeeding women, the Healthy Eating Index was not associated with HMO composition at 3–4 months postpartum. 24 These findings are particularly relevant given the limited information that is available regarding the impact of plant-based diets during lactation on breast milk composition. 25
HMOs have been associated with several infant health benefits including promoting the growth of a beneficial microbiome through their prebiotic effects, promoting growth and development, suppressing pathogenic bacteria, protecting against infectious pathogens, and decreasing the prevalence of allergies.4,5,9,10,26 Individual HMOs have been attributed to specific benefits including observational studies linking DSLNT to reduced rates of necrotizing enterocolitis in the preterm infant, 27 and randomized clinical trials showing lower rates of infection and inflammatory biomarkers in infants supplemented with 2′FL and LNnT. 26
The Academy of Nutrition and Dietetics has stated that a vegan diet is appropriate for all stages of the life cycle, including pregnancy and lactation. 28 However, several European organizations have issued recommendations against adhering to a vegan diet during pregnancy, lactation, and/or infancy and childhood.29–32 In the context of these inconsistent recommendations and, considering that HMO composition has been associated with specific health benefits briefly summarized above, the present findings are significant. We previously reported on vitamin B12 (B12), choline, and fatty acids composition in breast milk samples from the same vegan, vegetarian, and nonvegetarian participants.33–35 For the most part, those findings showed no statistically significant differences in these nutrient contents between diet groups. The majority of vegan subjects in our study supplemented with B12; therefore, these findings suggest that vegan lactating women who supplement with B12 are not at a nutritional disadvantage to other lactating women regarding the nutrients we evaluated (B12, water-soluble choline, total fat, and HMO). Our current findings on HMO composition add to the limited data available on the breast milk composition of vegan lactating women and show that the breast milk in vegan women supplemented with B-vitamins is not different in HMO composition.
Other maternal factors influencing HMO status
Secretor status had the largest influence on milk HMO composition in our study, impacting total HMO and 11 individual HMOs. The impact of secretor status on HMO composition in well documented in the literature.4,9,19,36 Lactation stage also had a significant influence on several HMOs in our study, including positive (e.g., 3′SL, DFLac) and negative correlation (e.g., 6′SL, LSTc) correlations. Others have identified lactation stage as a major factor influencing HMO composition. Sprenger et al. 37 reported decreases in 2′FL, 3′SL, 6′SL, LNnT, and LNT over the first 4 months postpartum in a cohort of 50 mothers of healthy term infants in Singapore. Samuel et al. 38 studied the longitudinal changes in 20 HMOs from 290 European mothers over the first 4 months of lactation and reported that most HMOs decreased over time, with the exception of 3FL that increased over time. Chaturvedi et al. 36 also described an increase in 3FL in a longitudinal study of 12 women over the first year postpartum. We did not observe an increase in 3FL by lactation stage; however, our study was cross-sectional that may have limited ability to detect some time-dependent changes. In addition, several participants in our study were >12 months postpartum and there is little information on the longitudinal composition of HMOs beyond 1 year. In a longitudinal study of 19 women from 11 to 17 months postpartum, total HMO concentration significantly increased, though trends in individual HMOs were not reported. 39 Longitudinal changes in HMOs in later stages of lactation are an important area for future research. 40
We observed that maternal BMI was positively associated with total HMOs and 3′SL. Findings in the literature regarding the impact of maternal BMI on HMOs are inconsistent. Azad et al. 21 measured HMOs at 3–4 months postpartum in 427 Canadian mothers and reported that a single HMO, LNH, was lower in women with a prepregnancy BMI >30 kg/m2. Ferreira et al. 41 described a significant association between prepregnancy BMI and LNnT (positive), LNFPIII (negative), and DFLNH (negative) in a semilongitudinal study of 101 Brazilian women. Parity was positively associated with four HMOs in the Brazilian cohort, whereas maternal age had no relationship with HMOs. In our study, parity and maternal age were not associated with HMO composition, but that could be due to the relatively low overall sample size.
Understanding the factors that impact HMO composition is important in fostering optimal infant health, as HMOs are associated with aiding in the promotion of physical and mental development, protection against infectious pathogens, and reduction in the prevalence and severity of inflammatory conditions (e.g., allergies and asthma).5,10,24,27,42 In this pilot study, we showed that maternal plant-based diets were not associated with different HMO profiles in breast milk.
Limitations
Our original study was powered to detect differences in B12 composition. 35 Detecting a 20% difference in the HMO LNT, which is not influenced by secretor status, would require a sample size of 206 based on the variability in LNT concentrations reported by McGuire et al. 6 in 41 lactating women from Washington; therefore, larger studies are needed to confirm the findings of our pilot study. Furthermore, we had limited diversity in our convenience sample, with the majority of participants being Caucasian well-educated mothers; therefore, findings may not be generalizable to other populations including food insecure. The majority of vegans in our study were taking B-vitamin supplements, which may have contributed to their nutritional status. HMOs are influenced by the stage of lactation and our samples came from mothers who breastfed from just a few weeks to over a year.
Conclusions and Practical Application
There is a substantial evidence for the health benefits of HMOs in infant growth and development. In this first study to date on assessment of HMOs in milk from well-educated vegan, vegetarian, and nonvegetarian mothers who regularly consumed B-vitamin supplements, we did not observe a statistically significant difference in the HMO composition. This finding suggests that lactating women who are vegans consuming B12 supplements do not produce breast milk that is different as it relates to HMO composition. As the status of key nutrients in vegans varies, the findings may not be applicable to all vegans, especially those not regularly taking B12 supplements or those who are food insecure. Additional research with larger sample size is needed to confirm our results regarding HMO composition in milk from mothers adhering to different diet types. A research study that assesses impact of plant-based diets on HMO in colostrum may give an additional light in impact of diet on HMO.
Footnotes
Acknowledgments
Authors thank all study participants for contributing their milk samples for analysis.
Authors' Contributions
R.P. designed the study, conducted research, and wrote the article. M.T.P. designed the study, conducted the study, analyzed data, and wrote the article. J.N. wrote the article. M.C., A.F., and L.B. analyzed samples. All authors reviewed and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by a grant from the Vegetarian Nutrition Dietary Practice Group, The Academy of Nutrition and Dietetics.