
Abstract
Background:
Vitamin D (vitD) plays a major role in maintenance of bone mineral homeostasis. It is unknown if bone mineral content (BMC) and bone mineral density (BMD) differ between infants who receive direct vitD supplementation and those who receive vitD indirectly via their mother's breast milk, while she received a high dose of vitD. It is hypothesized that there would be no differences in BMC or BMD by treatment group.
Design/Methods:
Randomized, double-blind trial to compare BMD and BMC of infants who received direct vitD (400 IU vitD3/day) in addition to their mother receiving standard dosage (400 IU vitD3/day) versus infants whose mothers were their only source of vitD and were given high-dose supplementation (6,400 IU vitD3/day). Participants were exclusively breastfeeding mothers and their infant consuming only human milk. Infant BMC and BMD were measured by dual-energy X-ray absorptiometry (DXA) scans of the infant's total body using Hologic Discovery A Densitometer and analyzed using Hologic Infant software at 1, 4, and 7 months of age.
Results:
Infant BMC and BMD did not differ significantly at 1, 4, or 7 months of age between direct and indirect supplementation arms. The mean difference in BMC from 1 to 7 months was 1.624 and 1.464 g for the 400 and 6,400 IU groups, respectively, (p = 0.5); the mean difference in BMD over this same period was 0.042 and 0.032 g/cm2 for the 400 and 6,400 IU groups, respectively (p = 0.2). Although some differences among races were observed, this did not reflect changes in bone growth between the treatment arms.
Conclusion:
High-dose vitD supplementation of mothers during lactation provided an efficacious alternative to direct supplementation of infants, as evidenced by noninferior infant BMD and BMC.
Clinical Trial Registration number: NCT00412074.
Introduction
Among numerous other functions in health, vitamin D (vitD) plays a major role in maintaining bone mineral homeostasis through the regulation of serum calcium and phosphorus concentrations. This is accomplished through the promotion of both intestinal absorption of these nutrients and their release from bone. 1 The major source of vitD occurs when humans are exposed to sunlight, with less being obtained from foods and supplements. Ultraviolet B radiation photons convert 7-dehydrocholesterol in the skin to previtamin D3 in keratinocytes of the epidermis, which then isomerizes to vitamin D3. 2 An association is seen between lower bone mineral status and increased risk of fractures in childhood. 3 On the severe end of the spectrum, vitD deficiency in early infancy and childhood can lead to craniotabes and rickets, respectively. 4
Infants born to mothers in at-risk populations for vitD deficiency, such as those whose exposure to sunlight and dietary intake of vitD are low, are at risk for development of these skeletal disorders if not properly supplemented. 5 Breastmilk is known to be low in vitD and its metabolites if the mother herself is vitD deficient. 6 Many women throughout the world are vitD deficient or have marginal sufficiency. 7 Therefore, exclusive breastfeeding under such conditions does not provide infants with adequate amounts of vitD.
As a result of this variability in maternal vitD status, to ensure adequacy of infant vitD status, the American Academy of Pediatrics recommends that all infants who are breastfed receive 400 IU vitD/day starting within the first few days after delivery. 8 As an alternative to direct infant supplementation, there exists the alternative of higher maternal vitD supplementation of 6,400 IU/day to achieve a sufficient vitD concentration in breastmilk.9–11
Much of the literature examining the effect of a mother's gestational vitD status on her offspring's bone mineralization, as measured by bone mineral content (BMC), has shown varied results. One study examining the effect of high-dose (2,800 IU) versus standard-dose (400 IU) supplementation from the 24th week of pregnancy to the 1st week postpartum did reveal higher bone mineralization in the offspring during the first 6 years of life. 4 Ultimately, additional randomized controlled trials testing the causality of the existing observational studies are needed.
In our earlier study comparing the effectiveness of maternal vitD3 supplementation with 6,400 IU per day alone, to maternal and infant supplementation with 400 IU per day, it was concluded that the dosage of 6,400 IU per day adequately supplied the mother's breast milk with vitD for her nursing infant with a mean antirachitic concentration of 873 ± IU/L. 12 This finding was significant as it represents a safe alternative method with which to provide supplementation to infants, while effectively treating a deficient mother simultaneously.10,13 In addition to 6,400 IU/day, maternal supplementation 5,000 IU per day or 150,000 IU monthly also have been shown to achieve infant sufficiency. 14
Differences in BMC or bone mineral density (BMD) between babies receiving a standard dosage of vitD supplementation directly, and those receiving vitD solely through their mother's vitD sufficient breast milk, have not been analyzed to date. Therefore, the purpose of this study was to determine if there was a significant difference in bone mineralization observed among these two groups.
We chose to assess both BMD and BMC because both measurements have flaws and benefits. For example, dual-energy X-ray absorptiometry (DXA)-derived BMD is an areal, rather than a true volumetric density. However, children's bones grow over time and the growth is not uniform in three dimensions. BMC, on the contrary, is reproducible and lacks real density-related errors, but DXA has a slight underestimation of BMC in neonates. A combination of both parameters was determined to be the most accurate measure of bone mineralization. 15
Our hypothesis was that there would be no difference between infants who received direct and indirect supplementation, unless the mother was severely vitD deficient. The results of this aspect of the study are presented here.
Methods
Study design
The NICHD Lactation vitD Supplementation trial was conducted by our group (2006–2011) and included two sites, the Medical University of South Carolina (MUSC) and the University of Rochester (U of R). It was a randomized, double-blind trial, which compared the effectiveness of three doses of vitD supplementation (400, 2,400, or 6,400 IU vitD3/day) in exclusively lactating women and associated doses in their infants (400, 0 and 0 IU vitD3/day, respectively). Maternal blood, maternal urine, and infant urine samples were taken monthly, and infant blood samples were drawn at baseline (4–6 weeks postpartum), month 4, and month 7.
Additional previously unpublished data were collected via performance of DXA scans on the infants at 0, 4, and 7 months after birth. As Aim 2 of the aforementioned NICHD trial, we sought to determine if there was a difference in the BMD or BMC of babies who received direct supplementation (400 IU) in addition to their mother receiving standard dosage (400 IU) versus those whose mothers were given high-dose supplementation (6,400 IU). We hypothesized that the infants would not differ in their BMC or BMD based on treatment.
Study population
The participants in this study were exclusively breastfeeding mothers and their singleton infant living in Charleston, South Carolina, or Rochester, New York. Criteria for entry included that the infant must be receiving no other form of nutrition other than human milk at the beginning of the study, within 4–6 weeks postpartum, and confirmation that the mother planned to continue exclusive/full breastfeeding for the next 6 months. As long as their sole milk source was maternal breast milk, the use of complementary foods beginning at 6 months of age was permitted in accordance with the AAP guidelines and World Health Organization recommendations. In addition, infants had to be ≥35 weeks' gestation and in good general health at entry into the study.
Exclusion criteria
Women with diagnosis of type I or II diabetes, hypertension, parathyroid disease, or uncontrolled thyroid disease, or those with twins or multiple births.
Infants <35 weeks' gestation; with history of >72 hours in the neonatal intensive care unit (NICU); any inborn error of metabolism; history of congenital anomalies; or history of consuming >10% of their diet as formula at the time of enrollment. Twins and multiples were not eligible to participate.
Women who were combination feeders at the time of enrollment (i.e., partially breastfeeding and formula-feeding their infants). Those who chose to combination feed after enrollment and before the 4-month study visit exited the study.
Study interventions
Mothers were randomly assigned to receive one of three potential regimens. Group 1 received 400 IU vitD3 (placebo and 1 prenatal vitamin containing 400 IU vitD3); Group 2 received 2,400 IU (2,000 IU vitD3 per day and 1 prenatal containing 400 IU vitD3); and Group 3 received 6,400 IU (6,000 IU vitD3 and 1 prenatal containing 400 IU vitD3). The infants of these mothers were also supplemented according to their mother's assigned group. Infants of mothers in Group 1 received 400 IU vitD3, while infants of mothers in Groups 2 and 3 received a placebo containing 0 IU vitD3 throughout the 6 months of the study.
An interim analysis conducted in February 2009 by the Data Monitoring and Safety Committee deemed that the 2,400 IU treatment arm should be discontinued, as a disproportionate number of infants in that group were found to be vitD deficient (defined as <20 ng) at the 4-month visit compared to the 400 and 6,400 IU groups. 10 As such, this group was not included in this analysis.
Study outcome measures
Laboratory measurements
The mother and infant serum calcium and phosphorus concentrations were measured at baseline using standard methodology and laboratory normative data by both MUSC and the University of Rochester's Clinical Chemistry Laboratories. Cross-validation between these two laboratories was performed for 5% of the samples (interassay variation 5.4%).
Circulating 25(OH)D and vitD (parent compound) were measured in the laboratory of Dr. Bruce Hollis using radioimmunoassay and high-performance liquid chromatography, respectively, expressed in nmol/L. On the basis of clinical laboratory classifications and the work of Heaney et al. and Vieth et al., deficiency was defined a priori as total circulating 25(OH)D concentration of <50 nmol/L (20 ng/mL). The inter- and intra-assay coefficient of variation was <10%.
Maternal and infant circulating Intact PTH (iPTH) was measured by immunoradiometric assay (IRMA) that uses two polyclonal antibodies (Diasorin, Stillwater, MN). The first antibody, specific for PTH 39–84, is bound to a solid phase bead. The second antibody is specific for PTH 1–34 and is labeled with 125I. The adult normal range for iPTH in our laboratory is 13 to 54 pg/mL (1.3 to 5.4 pmol/L). Higher vitD levels are associated with lower iPTH; as vitD status improves, iPTH concentration declines.
BMD (g/cm2) and BMC (g) were measured by Dual-energy X-ray absorptiometry scans of the infant's total body using Hologic Discovery A Densitometer and analyzed using Hologic Infant software at 4 weeks, 4 months, and 7 months of age. There were two primary regions of focus—region 1 (spine) and region 2 (hip). Hologic software does not provide normal values for these two regions. To prevent movement during the scans, infants were swaddled in a sheet and an infant video was played during the entire scan. There was one certified radiology technician at each site who performed the DXA on all patients. A phantom spine was used to ensure standardization and inter-reliability between the sites, with <10% variability between the two sites.
Statistical methods
Sample size
Based on the goal of supplementation, which was to achieve a minimum average circulating 25(OH)D of 100 nmol/L (40 ng/mL) in the three racial/ethnic maternal groups, a final analytic sample of 15 white/Caucasians in each supplementation group (paired analysis, ∞ = 0.05, two tailed) would achieve a statistical power of 80%. To oversample in accommodation of possible attrition, 21 white/Caucasian maternal subjects per treatment group were to be enrolled. Despite the estimation that four African Americans/Hispanics in each supplementation group would achieve statistical power of 80%, to attain a balanced design and to ensure more stable variances, a final analytic sample of 21 subjects (per treatment group) was enrolled. Therefore, the study was appropriately powered to detect important changes specific to each racial/ethnic group and each study site.
Randomization
We originally intended to randomize the 189 participants into three treatment arms, with 63 participants in each group further substratified by race/ethnicity. This was accomplished using Proc Plan in SAS. At the time of enrollment, the study coordinator accessed the randomization Web page from the General Clinical Research Center website (later CTRC) developed uniquely for this investigation. Only the Research Pharmacy and the Data Coordinating Center were notified via the computer program that a patient had been newly enrolled and of the group assignment. Investigators, study team, and subject remained blinded to treatment assignment throughout the study period.
The loss of the 2,400 IU treatment arm resulted in 216 mother/infant pairs in the two remaining arms. The loss of the 2,400 IU arm did not alter the ability to assess effectiveness of the remaining arms, as each arm could be viewed as an independent trial.
As shown in the Consolidated Standards of Reporting Trials (CONSORT) flow diagram in Figure 1, of the 564 women who consented to participate, 175 mother/infant pairs met the exclusion criteria as described previously. Of the remaining women, 389 met the criterion for exclusive breastfeeding at entrance into the study and had baseline 25(OH)D concentrations measured; 55 were in the 2,400 IU group and were excluded from the final analysis, with 334 mother/infant pairs randomized to the 400 and 6,400 IU groups.
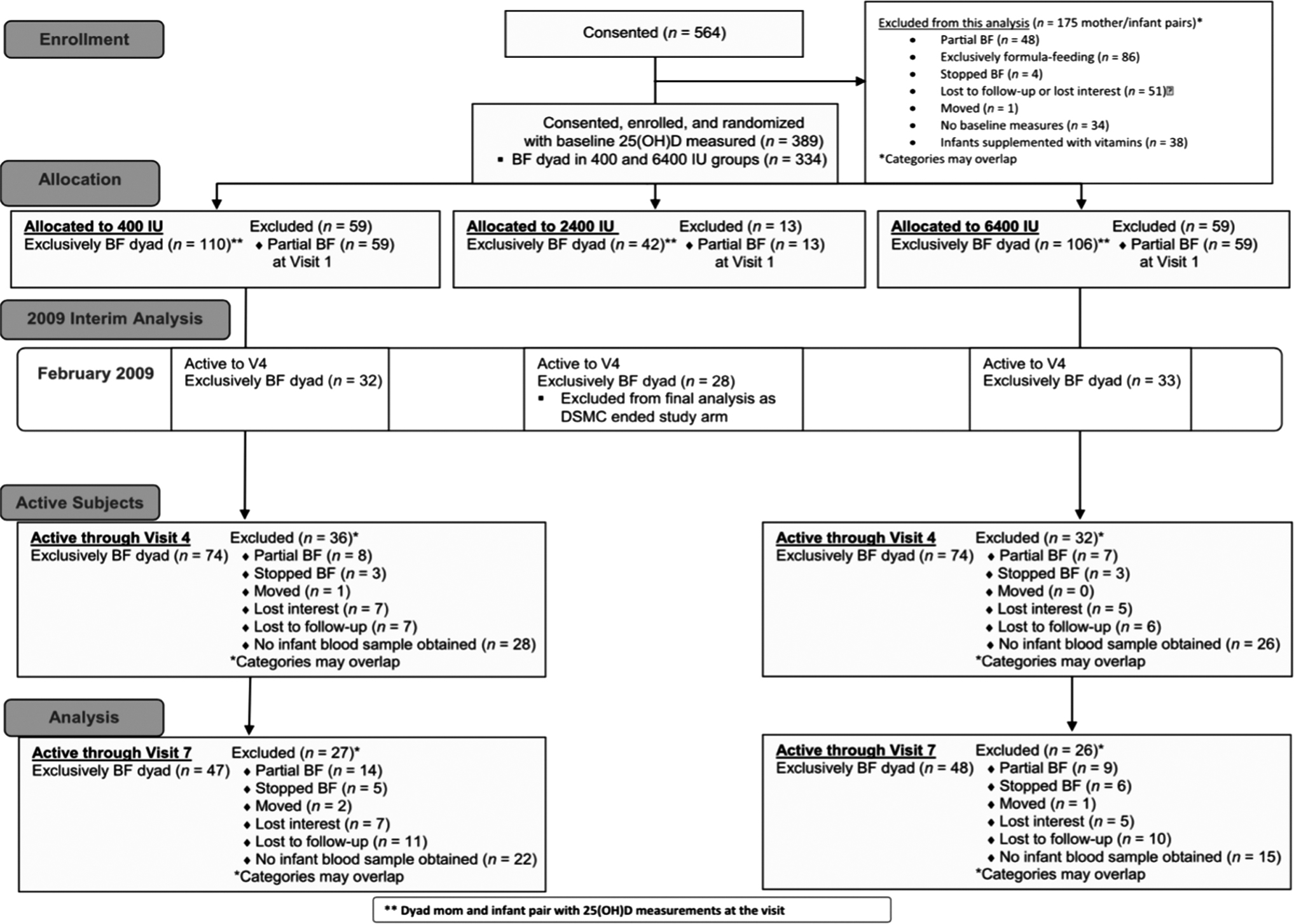
CONSORT flow diagram of study participants throughout the trial. CONSORT, Consolidated Standards of Reporting Trials.
Statistical analysis
Descriptive statistics were used to characterize and compare the treatment groups at baseline. Chi-square and analysis of variance (ANOVA) were used to test for differences in categorical data. Student's t-test analyses were used to test for differences in normally distributed variables. The Wilcoxon rank-sum test was used for analyses involving nonparametric variables. Regression methods (multivariate and logistic) included variables that were significant in bivariate analysis to model 25(OH)D status. Correlation analysis was performed by Spearman's correlation. SAS v version 9.4 (Cary, NC) was used for these analyses. Significance was set a priori as p < 0.05.
In the analysis of the BMC and BMD data, summary statistics were used to show mean, standard deviation, minimum, and maximum values. Student's t-test analyses were used to show difference in mean DXA measurements between treatment group, gender, and feeding type. ANOVA analyses were used to show difference in mean DXA measurement among the races. Linear regression analyses were used to show association between DXA and maternal and infant 25(OH)D values, race, and feeding type. Mixed model analyses were used to show effects over time to DXA and race, treatment, feeding type, maternal 25(OH)D, infant 25(OH)D, and visit.
Study sites
As previously described, the study was conducted at the Medical University of South Carolina (MUSC; latitude 32.78°N) and the University of Rochester (U of R; latitude 43.15°N) (1, 2). Approval for this two-site study was granted by (1) MUSC's Institutional Review Board for Human Subjects HR #16536 and the Clinical and Translational Research Center (CTRC; Protocol #752) and (2) the U of R's Institutional Review Board for Human Subjects (#14460) and the CTRC (Protocol #1129). The study was registered via ClinicalTrials.gov.
Results
Of the 334 women and their infants who were initially randomized into the 400 and 6,400 IU treatment arms, 148 continued to exclusively/fully breastfeed and completed the study to visit 4; 95 completed the study through visit 7. The main reason for subject attrition during this study was change in breastfeeding status, as outlined in Figure 1. The potential interactions of treatment and time of year (season) or location (SC versus NY) were both found to be nonsignificant.
The sociodemographic characteristics of the two treatment groups are outlined in Table 1 below. Baseline vitD status for mothers and their infants who participated in the study through visit 4 are found in Table 2 below. As outlined in this table, African American mothers and infants had significantly lower circulating 25(OH)D concentrations than did white/Caucasian subjects. In fact, several minority infants exhibited severe vitD deficiency after 1 month of breastfeeding.
Sociodemographic Characteristics of 400 and 6,400 IU Treatment Groups
Baseline Vitamin D Status for Mother/Infant Pairs
Profound deficiency by the IOM's Guidelines is defined as a 25(OH)D concentration, 25 nmol/L (10 ng/mL) for both adults and children (including neonates and young infants). 1
The level of detection of the assay for 25(OH)D is 2.5 nmol/L.
SD, standard deviation.
Significant results found in the earlier effectiveness treatment study (NICHD Lactation vitD Supplementation trial, 2006–2011) included a trend where mothers in the 400 IU treatment group were more likely to have 25(OH)D concentration <50 nmol/L at visit 4 compared with the 6,400 IU group. In women who continued to exclusively/fully breastfeed through visit 7, significant differences by treatment group were found at visits 4 and 7, with 25(OH)D and vitD being lower in the 6,400 IU group. In addition, at visit 7 only, iPTH and serum phosphorus were lower in the 6,400 IU group.
The infants in the study who were fully breastfed through visit 4 did not differ by treatment group on any of the parameters measured at either baseline or at visit 4. The infants who were fully breastfed through visit 7 did not differ by treatment group at baseline, visit 4 or visit 7 on any of the parameters measured. Thus, infants whose only source of vitD was maternal (6,400 IU group) did not differ from those infants who received oral supplementation of 400 IU/day (400 IU group) on any of the laboratory parameters tested.
Also, no differences between treatment groups were found in infant weight, length, and head circumference at any of the visits. This trend persisted after being controlled for race/ethnicity. The number of adverse events and serious adverse events did not differ by treatment group in this study or in this subcohort of infants included in this analysis with DXA results at 1, 4, and 7 months. 10
BMC and BMD, as measured by DXA scan of infant spines, were not statistically significantly different among infants who received direct vitD supplementation of 400 IU (400 IU treatment group) versus those whose sole source of vitD was their mother's breast milk, where she received high-dose supplementation of 6,400 IU vitD3/day (6,400 IU treatment group). This was true at 1, 4, and 7 months of age, as indicated in Figure 2A and B below. When adjusted for breastfeeding, no significant differences were found in BMC or BMD at 1, 4, or 7 months.
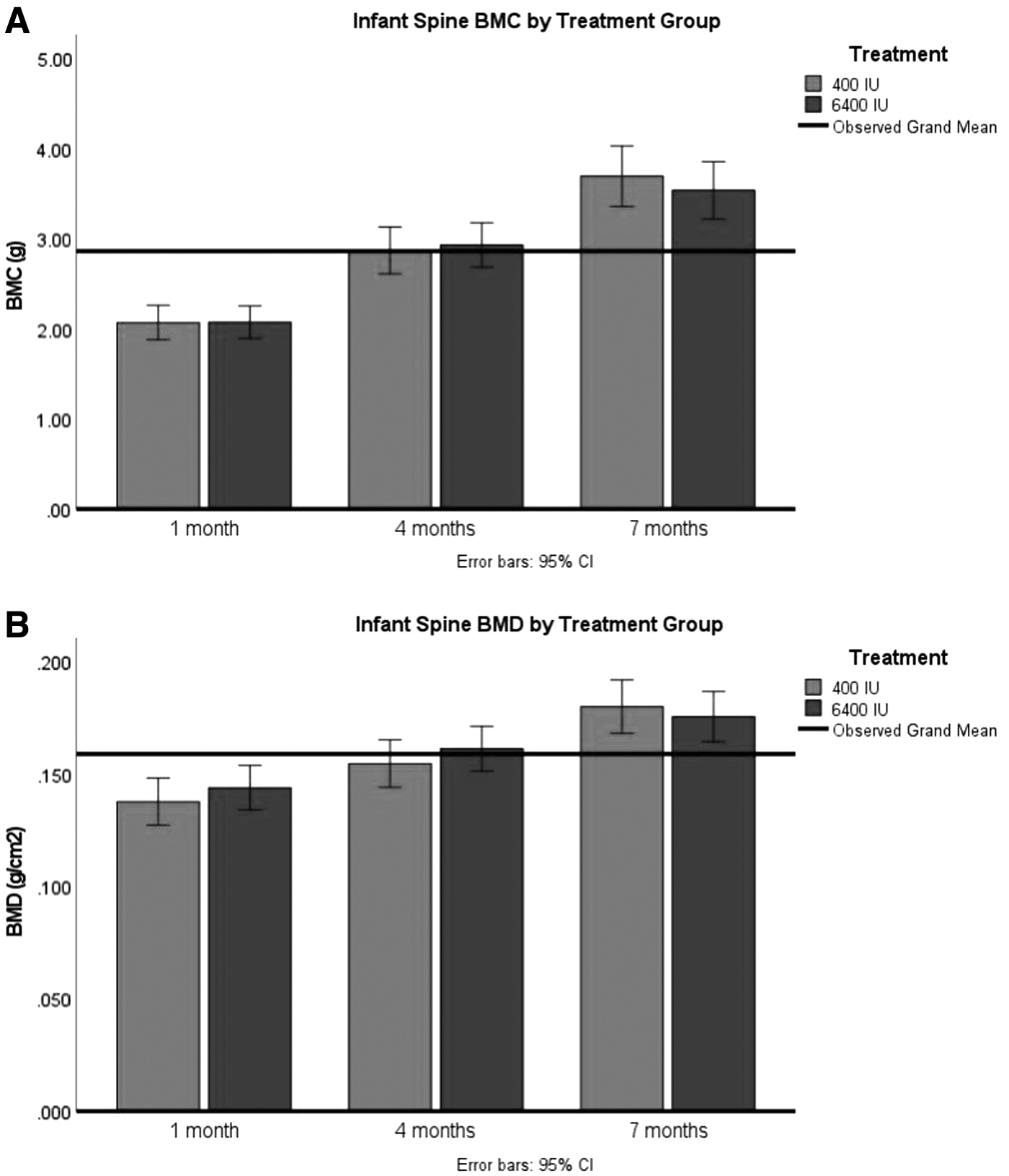
The mean differences in BMC and BMD from 1 to 7 months also did not differ significantly between the two treatment arms, as indicated by the statistically insignificant p-values in Table 3 below.
Mean Difference in BMC and BMD from 1 to 7 Months
BMC, bone mineral content; BMD, bone mineral density.
When adjusted for race, both Hispanic and white/Caucasian infants had significantly higher BMC at baseline (1 months of age) than their African American counterparts (p = 0.007), as shown in Figure 3A below. BMD at the same age, displayed in Figure 3B below, did not differ significantly among races (p = 0.3). There were no significant differences in either BMC or BMD by race/ethnicity at 4 or 7 months.

When stratified by race, the mean difference in BMC between 4 and 7 months of age was larger for African American infants than for white/Caucasian infants (p = 0.048). Between the 6-month study period of 1–7 months, African American infants also had a larger increase in BMC than white/Caucasian infants (p = 0.02) and a larger increase in BMD than white/Caucasians and Hispanic infants (p = 0.02). The rate of change in infant spine BMC and BMD, stratified by race, is presented below in Supplementary Figure S1A and B.
Discussion
The objective of this study was to determine if BMC or BMD differ between infants who are directly supplemented with vitD and those who are indirectly supplemented via their mother's vitD sufficient breast milk. We hypothesized that no significant differences would be observed between the direct (400 IU) and indirect (6,400 IU) treatment groups. The results of our data analysis support this hypothesis. Based on these BMC/BMD findings and the safety profile of high-dose supplementation in mothers and their breastfeeding infants, maternal high-dose vitD supplementation provides a safe alternative to direct supplementation of infants. 13
The work performed in this study is novel, and the literature lacks similar studies for comparison. Although differing from our methodology, a multicenter, double-blind, placebo-controlled trial in 2016 assessed the effect of vitD supplementation (cholecalciferol 1,000 IU) during pregnancy on neonatal BMC, as measured by DXA. This large trial of over 1,000 pregnant women found that neonatal whole-body BMC of those infants born to mothers assigned to cholecalciferol 1,000 IU/day did not differ significantly from that of infants born to mothers who received a placebo (p = 0.21). Although these results did not match the expected relationship, that infants of mothers receiving supplementation would have increased whole-body BMC compared with placebo, it showed that this level of supplementation was safe. 16
As previously mentioned, another study focusing on the effects of gestational vitD supplementation on bone mineralization compared high-dose (2,800 IU/day) versus standard-dose (400 IU/day) vitD. Instead of looking at infant bone mineralization alone, this study performed longitudinal anthropometric assessments until age 6 years, and measured BMC and BMD at age 3 and 6 years by DXA scans. The results of this study showed that those in the high-dose supplementation group in pregnancy had improved bone mineralization through age 6 years compared with the standard dose. 4 While both aforementioned studies provide us with important information, studies focused on supplementation of lactating mothers in the postpartum period, and on the results of indirect supplementation of infants through their breast milk, are necessary.
Strengths of this study include its performance at two different sites, SC and NY, with varying latitudes. The study was performed as a randomized controlled trial. Inter-reliability measures were used among the two sites to ensure consistency of the DXA scan performance, including calibration using infant software and a standard phantom spine. A potential limitation of this study is movement artifact in the DXA scans, although multiple measures were taken to avoid infant movement during the scans. Other limitations such as a study population limited to only three racial/ethnic groups and a relatively small sample size by the 7th month of the study (due to cessation of breastfeeding) are important to note.
A future direction for investigation may be to expand upon the racial differences we observed in BMC and BMD. A better understanding of baseline bone mineralization among racial/ethnic groups may allow dosage to be tailored appropriately. Another topic for future exploration is the comparison of DXA versus quantitative ultrasound for measurement of bone mineralization.
Conclusions
It is well accepted as a current standard of care that exclusive breastfeeding necessitates direct vitD supplementation of infants within a few days of birth. Our earlier effectiveness treatment study (NICHD Lactation vitD Supplementation trial, 2006–2012) countered this notion when it demonstrated that when given 6,400 IU of vitD, a lactating mother can fully transfer from her circulation to her milk enough vitD for her nursing infant, with no additional supplementation required by the infant. 13 However, the potential impact of direct versus indirect vitD supplementation on infant BMC and BMD was previously unknown. In support of our hypothesis, analysis of the collected data revealed no significant difference in infant BMC and BMD spanning 7 months of age between treatment groups.
Footnotes
Authors' Contributions
The authors listed made significant contributions to the above article.
Acknowledgments
We are thankful to the women and their infants who participated in this clinical trial, as well as the research and medical staff at the Medical University of South Carolina (MUSC) and the University of Rochester.
Disclosure Statement
No competing financial interests exist.
Funding Information
Funded, in part, by National Institutes of Health (NIH) 5R01HD043921, NIH RR01070, MUSC Department of Pediatrics, and by the South Carolina Clinical & Translational Research (SCTR) Institute, with an academic home at the Medical University of South Carolina, NIH/National Center for Advancing Translational Sciences grant no. UL1 TR000062.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.