
Abstract
Background:
Necrotizing enterocolitis (NEC) is a severe intestinal disease that often occurs in preterm infants, and there currently is a lack of specific and effective therapy. Human milk is rich in cells that may become a potential NEC treatment.
Research Aim:
To evaluate the safety and feasibility of cell-enriched fresh human milk treatment for premature infants with stage I NEC.
Materials and Methods:
Infants born at <1,500 g birth weight who developed stage I NEC were enrolled. Along with routine treatment for these infants, those in the intervention group were treated with cell-enriched fresh mother's milk (1 mL/kg) once per day for seven consecutive days. The intervention feasibility and safety were monitored and evaluated as primary outcomes. Short-term outcomes, including the duration of antibiotics, days to full enteral feeding and prognosis, were investigated as secondary outcomes.
Results:
Forty infants were enrolled, and 20 infants were included in each group. The demographic characteristics of the two groups of infants were comparable. All infants in the intervention group completed cell-enriched fresh mother's milk feeding for 7 days without any adverse clinical issues. The infants' vital signs were within the normal range during and after the intervention. None of the enrolled patients progressed to stage II NEC or above. The time interval from milk pumping to feeding was 3.7 ± 0.5 hours.
Conclusions:
Using cell-enriched fresh mother's milk to treat premature infants with stage I NEC was safe and feasible.
Introduction
Necrotizing enterocolitis (NEC) has emerged as one of the most common gastrointestinal emergencies of newborns, especially in preterm infants. Infants who survive NEC are still at significant increased risk of long-term complications, including abnormal growth, and neurodevelopmental delay.1,2
Although considerable research has been published, there is no known effective treatment for NEC to date. Current treatments such as bowel rest (cessation of oral feeds), abdominal decompression, broad spectrum antibiotics, and ventilation are mainly supportive therapies. It is becoming increasingly evident that there is a requirement for novel treatments specifically targeting the affected intestine. Human milk has been shown to be both bioactive and rich in cells, including epithelial cells, immune cells and human breastmilk stem cells (hBSCs) with multi-lineage properties.3–5
A quality improvement initiative in our own neonatal intensive care unit (NICU) that promoted the consumption of mother's own milk resulted in reducing the severity of NEC in very low birth weight (VLBW) infants, 6 which led us to speculate whether bioactive components of human milk may play a potential role in preventing NEC and repairing damaged gut tissue. We carried out this pilot study to evaluate the feasibility and safety of treating preterm infants diagnosed with Bell's stage I NEC using cell-enriched fresh human milk.
Materials and Methods
Design
This was a prospective cohort study. The investigators responsible for data collection and analysis were blind to the study. The study protocol was approved by the Children's Hospital of Fudan University Ethics Committee. Written informed consent was obtained from all the participants. This clinical pilot study was registered in the Chinese Clinical Trial Registry, a Primary Registry of International Clinical Trial Registry Platform, World Health Organization (first registered on 20/01/2021, no. ChiCTR2100042354).
Samples
This study was conducted in the NICU of Children's Hospital of Fudan University from August 2017 to July 2018. All VLBW infants (<1,500 g) admitted to the NICU during the study period who developed stage I NEC were eligible for this study. We defined and classified NEC according to modified Bell's criteria. 7 Infants with major congenital anomalies, inborn errors, or severe birth asphyxia, and parents who could not provide any mother's milk, in addition to hospitalization <7 days were all exclusion criteria. All VLBW infants were fed with human milk, either mother's own milk or donated breast milk, according to our NICU's feeding protocol. Mother's milk was given priority when available.
If informed consent was given, and the mother of the eligible infants was willing to provide fresh human milk for the study, the infant was enrolled in the intervention group; otherwise, the infant was enrolled in the control group.
Mothers in the intervention group were requested to provide at least one pump (any volume) of fresh human milk (within 4 hours of milk expression) per day for 7 days. A dedicated certified lactation consultant (CLC) instructed mothers in the intervention group how to collect and deliver fresh milk to the NICU in a hygienic way.
The fresh milk samples delivered to the NICU by parents were immediately processed in a sterile area of the NICU by a dedicated researcher. First, 1 mL/kg (infant current weight) whole fresh human milk was preserved in a sterile container for subsequent remixing with enriched cells. The cellular components of the remaining human milk were isolated as previously described. 4 In brief, a human milk sample was centrifuged at 805 g for 20 minutes at 20°C, the cell pellet was washed twice with normal saline and spun at 805 g for 5 minutes. The washed cell pellet from each milk sample was counted using a hemocytometer, while the enriched cells were remixed with the preserved 1 mL/kg whole fresh human milk sample and brought to the bedside ready for feeding.
In addition to routine medical management, patients in the intervention group received one dose of cell-enriched mother's fresh milk (1 mL/kg) once a day for 7 days via a nasogastric tube (NG tube) by the registered bedside nurse; 1 mL/kg of normal saline was given subsequently via the same NG tube to flush the cells attached on the tube surface. We only enrolled one patient in the NICU for intervention at any time to make sure the target patient was closely monitored by the research team. Parents had the right to withdraw from this study at any time.
Measurement
The primary study outcomes were feasibility and safety. Feasibility was defined as the ability of the mother to provide at least one sample of fresh human milk per day for 7 days following diagnosis of her infant as stage I NEC. Safety was defined as the ability of the infant with stage I NEC to tolerate administration of cell-enriched mother's own milk once a day for 7 days. Intolerance was defined as physiologic decompensation (desaturation, tachycardia or bradycardia, or hypotension) within half an hour after the intervention.
The secondary outcomes of the study included the duration of antibiotic treatment and feeding cessation, days to reach full enteral feeding (120 mL/kg/day of feeding with any milk) after diagnosis of suspected NEC, progression to NEC stage II or beyond, intestinal perforation, and death. In our center, supportive medical management alone is provided to patients with stage I NEC and most cases of Stage II NEC. Supportive medical management included bowel rest with intermittent gastric decompression, total parental nutrition, and empiric antibiotic therapy. Supportive care is initiated when NEC is suspected.
The course of treatment and whether to change antibiotics depend on serial physical examinations, laboratory (complete blood cells, C-reactive proteins, procalcitonin, blood/urine/cerebrospinal fluid culture, lactate levels) and radiographic monitoring results. Surgical intervention may be provided to patients with stage III NEC or critical case depending on surgical consultation.
Data collection
Data on each patient's demographics, clinical signs and related laboratory results, including NEC diagnosis, duration of bowel rest, days to reach full enteral feeding, and antibiotic use were recorded. For the intervention group, fresh human milk volume and total cell counts for each sample of milk provided, and the patients' vital signs before and after intervention were also collected.
After administration of each cell-enriched fresh milk feed, the vital signs (heart rate, respiratory rate, blood pressure, and transcutaneous oxygen saturation) would be monitored for at least half an hour.
Data analysis
Statistical analyses were performed using IBM SPSS Statistics 19 (IBM Corporation, 2010). Categorical variables were summarized by using counts and percentages. Continuous variables were summarized by using means and standard deviations, whereas the median (lower quartile–upper quartile) was used when there was a skewed distribution. Categorical variables were compared by using chi-squared tests or Fisher's exact test when appropriate; continuous variables were evaluated by using Student's t-tests or a Kruskal–Wallis test when appropriate. p-Values <0.05 were considered statistically significant.
Results
Characteristics of study participants
Forty patients were enrolled during the study period, with 20 patients in each group. The mean gestational age for all patients was 29.7 ± 1.7 weeks. The two groups were comparable in terms of sex, gestational age, birth weight, and maternal characteristics (Table 1).
Maternal and Infant Characteristics (n = 40)
SD, standard deviation.
In our study, the mean age at onset of suspected NEC was 23.2 ± 10.6 days. The intervention and control groups differed in timing of the onset of symptoms, and frequency of abdominal distension and apnea/bradycardia as presenting signs (Table 2).
Clinical Characteristics for Enrolled Necrotizing Enterocolitis Patients (n = 40)
CRP, C-reactive protein; PCT, procalcitonin; SD, standard deviation.
Feasibility of intervention and cell counts for each sample
All patients in the intervention group successfully received the intervention of feeding with cell-enriched human milk once a day for 7 days. A total of 140 samples of human milk was received, all of them were pumped at home and immediately brought to the hospital by parents. Most of the mother's milk sample (131/140) were received between 8:00 am and 12:00 am, and the time interval from milk pumping to feeding was 3.7 ± 0.5 hours, which met the “fresh milk” requirement of our intervention. The human milk volume provided by each mother each time varied (Fig. 1), and the average volume was 108 ± 38 mL each time in our study.
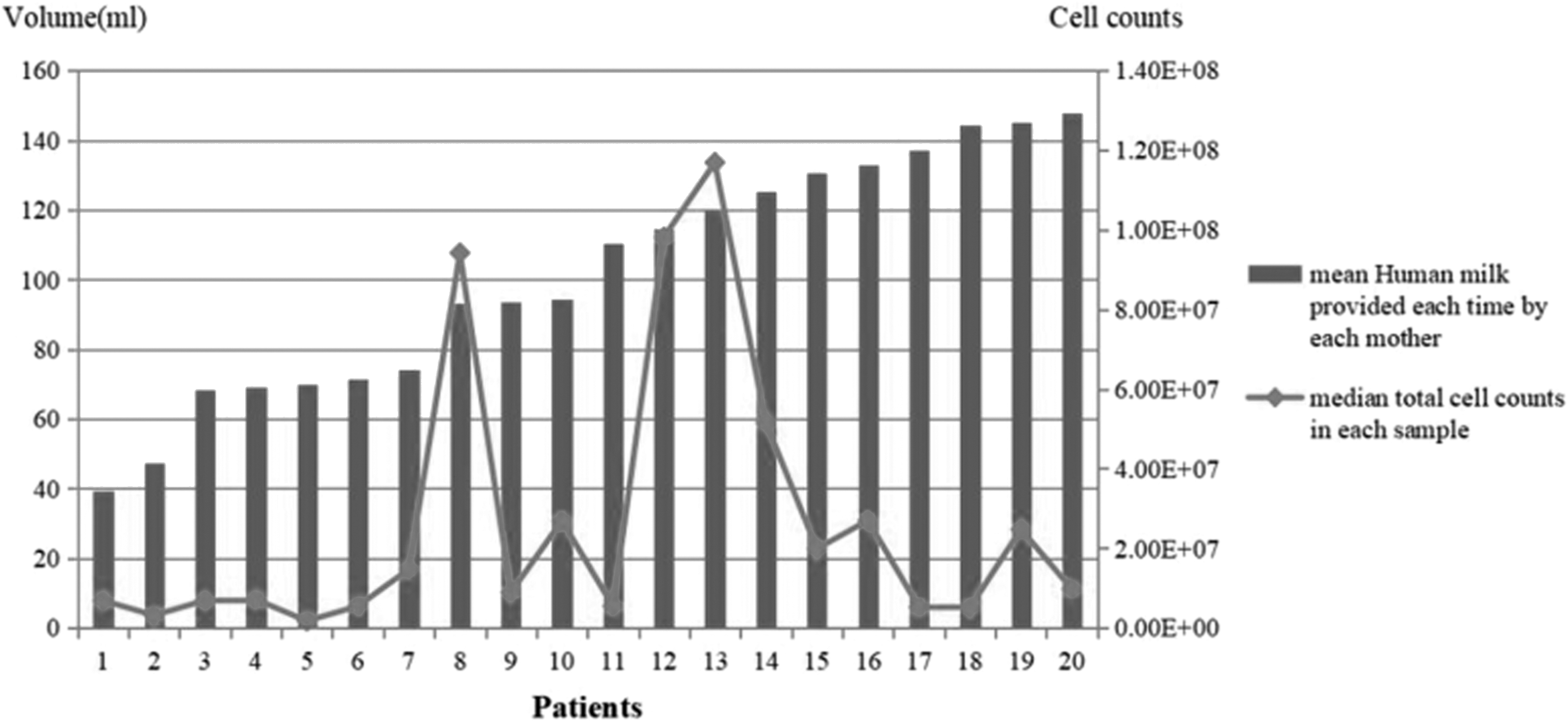
Human milk volume (mean) and cell counts (median) by each mother each time.
Apart from Patient 1 and Patient 2, other infants' mothers could provide an average of more than 50 mL of human milk each time. The median number of viable cells for all samples was 1.1 × 107 (interquartile range from 5.5 × 106 to 2.7 × 107). There was no correlated relationship between viable cell count and human milk volume according to our data (Fig. 1).
Safety of the intervention
Within half an hour after giving cell-enriched fresh human milk, all infants' vital signs were within the normal range, and there were no significant differences before and after the intervention (Table 3).
Vital Signs Pre and Post Intervention for Intervention Group (n = 20)
bpm, beats per minute (for heart rate); breaths per minute (for respiratory rate); IQR, interquartile range.
Short-term outcomes
There were no significant differences in antibiotic treatment duration, enteral feeding discontinuation, or days to reach full enteral feeding between the intervention group and the control group (Table 4). None of the patients in either group progressed to stage II NEC or above, and none of them presented with intestinal perforation, septic shock, or death through discharge.
Short-Term Outcomes of Enrolled Patients (n = 40)
NEC, necrotizing enterocolitis; SD, standard deviation.
Discussion
NEC is a potentially enticing target for stem cell treatment in neonates because it is a common and devastating disease for which there is currently no existing treatment, but clues exist that point to the potential benefit of stem cell therapy, particularly with human milk stem cells.
First, many studies have reported that the exclusive use of human milk feeds decreases the incidence and severity of NEC in preterm infants, and it is now recommended as best practice for very preterm infants.8,9 Second, Sun et al. 10 reported that the use of fresh human milk in very preterm infants offers greater protection against NEC than human milk that has been previously frozen. This suggests that there is a bioactive component of human milk that is degraded by time, freezing, and potentially, both. Third, several authors have reported that fresh human milk contains not only nutritional components, but also bioactive components including immunoglobulins, immune cells, probiotics, and others.5,11
Finally, Hassiotou et al., 4 Kakulas, 12 and Hassiotou and Hartmann 13 reported that fresh human milk is a rich source of stem cells capable of self-renewal and differentiation into cells of all three germ layers in in vitro studies. She also reported the survival of milk stem cells in the gastrointestinal tract of young mice and their transfer through the blood to the brain, thymus, pancreas, liver, spleen, and kidneys of the mice.14,15 More recently, these findings have been confirmed by independent researchers. 16 Although their exact function and fate are not yet well understood, human milk stem cells may possibly benefit the infant through active participation in growth and/or regeneration, and they may also have potential reparative effect on injured intestine epithelial cells of NEC. 17
While conventional treatment wisdom is that diseased or injured gut should be rested, that is, no oral feeding until recovery, we hypothesized that if fresh human milk contains bioactive components with repairing and/or regenerative capacity, it may actually have a beneficial effect on injured gut like NEC. In this study, we demonstrated that cell-enriched mother's own fresh milk intervention (1 mL/kg/day × 7) in Stage I NEC was feasible and safe for very preterm infants. Indeed, feeding is an ideal way of delivering milk stem cells with reparative capacity directly to the injured gut tissue.
Thus, this pilot study lays the groundwork for further research into the potential use of fresh human milk for prevention or treatment of NEC. We chose to use cell-enriched fresh human milk to minimize the volume of feeds and maximize its available bioactivity. We used fresh human milk with a 4 hours cutoff because Hassiotou et al. 18 reported that stem cells were sensitive to temperature change and had a half-life of about 4 hours. Consequently, our procedures for preparing the cell-enriched fresh human milk were designed to maximize survival of the stem cells in human milk and optimize its therapeutic potential.
This is a pilot study with a small sample size, and while the results here confirmed the feasibility and safety of this intervention, its effectiveness has not yet been studied. We did not collect data about consumption of mother's own milk for each group, which is also the limitation of this study.
Conclusion
Our pilot trial indicates that it is feasible and safe to feed preterm infants with stage I NEC with minimally cell-enriched mother's own fresh milk for potential treatment. This provides important information and the foundation for further efficacy research, opening up new avenues for exploring the effective prevention and treatment of NEC.
Footnotes
Acknowledgments
We thank all the study participants for their valuable contributions. We thank the nursing staff and the dedicated CLC of Children's Hospital of Fudan University for their great support in breastfeeding education to the parents.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors disclosed receipt of funding support from The Canada–China Clinical Research Program (2015: A pilot study using stem cell-rich human milk to treat early NEC) for the research, authorship, and/or publication of this article.