
Abstract
Objective:
This study was conducted to determine the effect of yoga practice on the breastfeeding self-efficacy and maternal attachment of primiparous mothers in the postpartum period.
Methods:
This study was performed in a quasi-experimental model with pretest and posttest control groups. The domain of the study was formed with women with 20–40-day-old babies enrolled in two Family Health Centers. One hundred and twenty-four women participated in the study. The Individual Identification Form, Breastfeeding Self-Efficacy Scale, and Maternal Attachment Scale were completed by the experimental and control groups. The experimental group engaged in 60 minutes of postpartum yoga practice 2 days a week for 8 weeks in the company of the researcher.
Results:
After yoga practice, there was a statistically significant increase in the breastfeeding self-efficacy and improvement in the maternal attachment of the experimental group (p < 0.05). The corresponding increase and improvement of the mothers in the control group were less than those of the mothers in the experimental group (p < 0.05).
Conclusion:
This study finds that it is beneficial for both the mother's and the baby's physical and psychological health for health professionals to teach mothers to practice yoga, which positively affects breastfeeding and maternal attachment in the postpartum period.
Introduction
Breastfeeding, which is beneficial for the mother and infant, is the preferred method for infant feeding in the postpartum period. 1 The World Health Organization (WHO) recommends that babies consume only breast milk, without water and other nutrients, for the first 6 months from birth, and that breastfeeding should be continued until the age of two and beyond, with complementary foods after the 6th month. 2
For the successful continuation of breastfeeding apart from sociodemographic and obstetric characteristics, such as the mother's age, education, health status, nutrition, baby's desired status, type and number of births, breastfeeding education, previous breastfeeding experiences, and support systems, the maternal attachment is also very important, which concerns the mother–infant communication and breastfeeding competencies that affect the mother's thoughts about breastfeeding.3–6
The breastfeeding proficiency is the degree to which a mother trusts herself to breastfeed her baby and trusts her ability in this regard.7,8 Mothers with a good level of breastfeeding proficiency try to solve problems they face by thinking positively in the face of those problems, and the effort they make then encourages them to breastfeed more. 8
Maternal attachment, meanwhile, can be defined as a maturing bond between a baby and its caregiver. 9 Maternal attachment, which becomes evident especially in the presence of stress factors, drives the mother and baby to seek each other and closeness between the two of them. 10 Maternal attachment forms immediately after birth as the baby begins breast seeking, sucking, swallowing, breastfeeding, catching, and seeking the mother. 10 Factors that increase the maternal attachment are a pregnancy being planned, wanted, and accepted by the mother, and the mother having been able to feel the baby's movements while pregnant, along with practices such as initiating sensory contact by holding and touching the baby after birth, and then breastfeeding the baby.10,11
It is important to support postpartum women with the continuation of breastfeeding, which can be affected by many factors. 1 Yoga, which is one of the practices that can support women in this period, is the oldest system in the world to emphasize the importance of physical, mental, and psychological balance for human development.12,13 The first stage of yoga practice, pranayama, is a breath-based method of respiratory control, and asanas (i.e., physical postures), the second stage of yoga practice, represent a form of exercise that enables active and/or passive participation of muscle groups. Meditation, the last stage of yoga practice, helps the person to feel good and escape negative thoughts.6,11,14,15
The WHO aims to increase the rate of babies receiving only breast milk for the first 6 months to 50% by 2025. 2 In accordance with this, the WHO states that it is important to support postpartum women with the continuation of breastfeeding.1,2 Specifically driving this research is the proposal that yoga practice helps mothers to cope with their negative thoughts about breastfeeding and increases mother–infant communication.
Our study aims to determine the effects of yoga practice on breastfeeding self-efficacy and maternal attachment. This study seeks to investigate two hypotheses.
H1: Yoga practice increases the breastfeeding self-efficacy of postpartum primiparous mothers.
H2: Yoga practice increases the maternal attachment of postpartum primiparous mothers.
Materials and Methods
Study design and participants
This quasi-experimental study with a pretest and posttest control group was conducted between September 2017 and December 2018 with mothers of 20–40-day-old babies registered to Family Health Centers (FHCs) No. 1 and 14 in Adıyaman, Turkey. The research was carried out on the cohort of the pregnancy education class of FHC No. 14. The pregnancy education class had a capacity of 10 people, with 2 midwives leading the class and informing the women about pregnancy, childbirth, and postpartum maternal health and child rearing.
Data collection
A power analysis was performed to determine the sample size, based on a study of women's breastfeeding self-efficacy carried out by Eksioglu and Ceber. 16 In this way, the required sample size was calculated to be 124 mothers, consisting of 62 mothers in the experimental group and 62 in the control group, with an effect size of 0.7, an error level of 0.05, and a population representation power of 0.95.
Considering the possibility that a small number of mothers would not be able to continue with the research for different reasons, 65 mothers were included in the experimental group and 65 in the control group, with 130 mothers in total. Three mothers from the experimental group of the study (not wanting to continue with monitoring n = 1, occurrence of health problems n = 2) and three mothers from the control group (occurrence of health problems n = 1, transition to additional food n = 2) were later excluded from the study. As a result, the research was completed with 124 mothers. As the pregnancy education class in which the study was conducted was held in FHC No. 14, the mothers registered in this FHC formed the experimental group, and the mothers registered in FHC No. 1 formed the control group.
The inclusion criteria for this study were mothers: in the age range of 20–35 years, who managed a term vaginal delivery, with only one infant who was exclusively breastfed, and with at least a primary school level of education. The exclusion criteria for the study were mothers who had a cesarean delivery, or with an infant who started receiving complementary food. The criteria for the termination of study participation were determined as the mother's desire to withdraw from the study, the occurrence of any complication related to the health of the mother or infant during the study, or the initiation of complementary food for the infant.
Measurement scales
The data for this study were collected using the Individual Identification Form, Breastfeeding Self-Efficacy Scale (BSES), and Maternal Attachment Scale (MAS).
Individual Identification Form
This form, prepared by the researcher, consisted of questions examining the sociodemographic and obstetric characteristics of the mothers.
Breastfeeding Self-Efficacy Scale
This scale, which was developed by Cindy Lee Dennis to determine the breastfeeding self-efficacy, consists of two subdimensions (“technical scale,” “scale for personal thoughts”) and 33 items. 8 The minimum and maximum total scores that can be obtained from the scale are 33 and 165, respectively, with the breastfeeding self-efficacy increasing as the total score increases. The Turkish validity and reliability of the scale was examined by Eksioglu and Ceber, and Cronbach's alpha value for the scale was calculated as 0.95. 16 In our study, Cronbach's alpha value was calculated as 0.93 (technical scale: 0.92, scale for personal thoughts: 0.94).
Maternal Attachment Scale
This scale, which was developed by Mary E. Muller, is applied to postpartum women with 1–4-year-old infants to determine their maternal feelings and behaviors. 17 The scale consists of 26 questions and a four-point Likert-type scale for the responses. The minimum and maximum total scores that can be obtained from the questions are 26 and 104, respectively. A high score indicates good maternal attachment. The scale was adapted to Turkish by Kavlak and Şirin, and Cronbach's alpha internal consistency reliability coefficient was calculated as 0.82. 17 In our study, Cronbach's alpha value was calculated as 0.95.
Ethics approval
İnönü University Health Sciences “Scientific Research and Publication Ethics Committee” approval was received for the research (no.: 2017/19-8) and written permission was obtained from Adıyaman Public Health Directorate. The mothers who agreed to participate in the study completed a consent form.
Intervention
After the mothers were informed of the study, data collection started with those who agreed to participate. The researcher collected data from the mothers through face-to-face interviews during the pregnancy education class. In September 2017, the mothers in the control group completed the pretest (Individual Identification Form, BSES, and MAS), and then 8 weeks after that the posttest (BSES and MAS).
After collecting the data from the control group, the experimental group filled out the pretest forms. In the pregnancy education class where the study would be carried out, it was arranged that these women would undertake postpartum yoga practice.15,18,19 The yoga was carried out in groups of five to seven mothers. In each session, the previously described steps of postpartum yoga practice were performed. The women in the experimental group were divided into two and either took yoga between 12:00 and 13:30 on Mondays and Wednesdays, or between 12:30 and 13:30 on Tuesdays and Thursdays, for a total of 8 weeks, at which time a posttest was completed. Figure 1 presents a flowchart of the research process.
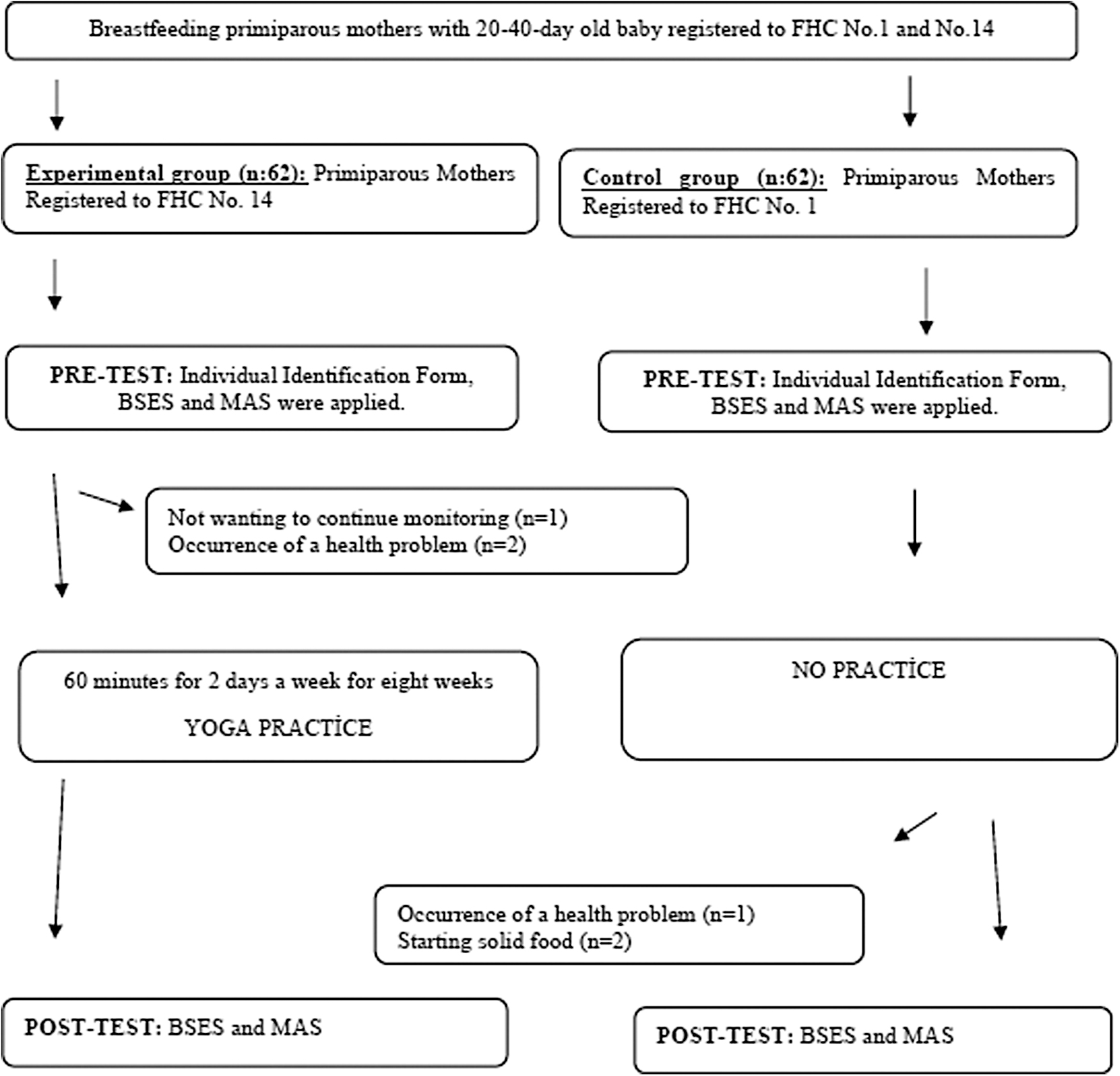
Application plan of the study.
The steps of yoga practice
In this study, yoga was practiced in the postpartum period for an average of 60 minutes, of which 5 minutes were reserved for breathing exercises, 45 minutes for yoga asanas, and 15 minutes for mother–baby communication and meditation.
Breathing awareness practice (5 minutes): The mothers were asked to sit comfortably and cross-legged on the yoga mat, put their hands on their knees, and close their eyes. Their attention was directed to their breathing. Through regular and soft abdomen, chest, and shoulder breathing, the body slowly relaxed.
Yoga asanas (45 minutes): The mothers performed yoga asanas, such as Bharadvajasana-Uttanasana (in the supine position, arm, shoulder, neck, and spine stretching intense forward bending), Supta and Jathara Parivartanasana (spine, arm, and leg stretches on the floor), Halasana (the waist is bent so that the toes touch the back of the head and rest for a while), Dandasana (forward bend and spine stretch), and Bidalasana (knee and arm stretch in all fours pose) for the main part of their postpartum yoga practice.
Mother–infant communication and meditation (15 minutes): The mothers were brought to the left lateral position, and their legs and necks were supported with yoga mats and blocks. The baby is laid sideways next to the mother. In this posture, the mothers closed their eyes and directed all their attention to the breathing. A calm and peaceful environment was created for deep relaxation and meditation. Music that the women liked was played in this setting to help them to relax. The mothers' attention was drawn to the love cord between the mother and baby during this meditation.
Data analysis
The coding and statistical analysis of the data were performed on a computer using SPSS (Statistical Package for the Social Sciences). The Shapiro–Wilk normality test was used to determine whether the quantitative variables' data showed a normal distribution. Percentages, arithmetic means and the standard deviation, the chi-squared test, and independent-samples t test were used to evaluate the normally distributed data.
Results
No statistically significant difference was found between the mothers in the control and experimental groups in terms of their sociodemographic and obstetric characteristics (p > 0.05) (Table 1).
Distribution of Sociodemographic and Obstetric Characteristics of the Mothers in the Control and Experimental Groups
Chi-square test.
The differences between the experimental group's total mean scores for the BSES “scale for personal thoughts,” BSES “technical scale,” and MAS in the pretest and posttest settings were found to be statistically significant (p < 0.05) (Table 2).
Comparison of Pretest, Intermediate Test, and Posttest Mean Scores of the Mothers in Terms of BSES and MAS
t Test in independent groups.
Statistically significant data are indicated in bold.
BSES, Breastfeeding Self-Efficacy Scale; MAS, Maternal Attachment Scale; SD, standard deviation.
Moreover, the differences between the control group's total mean scores for the BSES “scale for personal thoughts,” BSES “technical scale,” and MAS in the pretest and posttest settings were also found to be statistically significant (p < 0.05) (Table 2).
When mothers in the experimental and control groups were compared in terms of their total mean scores for the BSES and MAS pretests, there were no statistically significant differences between the groups (p > 0.05). Yet, the posttest results of the mothers in the experimental group were higher than those of the mothers in the control group, and the difference was statistically significant (p < 0.05) (Table 3).
Comparison of Pretest, Intermediate Test, and Posttest Mean Scores of the Mothers in the Experimental and Control Groups in Terms of BSES and MAS
t Test in independent groups.
Statistically significant data are indicated in bold.
BSES, Breastfeeding Self-Efficacy Scale; MAS, Maternal Attachment Scale; SD, standard deviation.
Discussion
In this study, the total BSES mean scores of the mothers in the experimental group were found to have increased after postpartum yoga intervention. Breastfeeding self-efficacy; it refers to the feelings that determine the mother's self-confidence and ability to breastfeed her baby. Mothers with good breastfeeding self-efficacy try to solve the problems by thinking positively in the face of the problems they experience.
Yoga is essentially a mental and spiritual practice involving physical movement (asana), techniques for conscious breathing (pranayama), and deep concentration, that is, meditation.15,19 In the study carried out by Trakroo et al., it was reported that pranayama practices calmed people down by providing deep relaxation. 20 Yet, in the literature review, no study was found into the effects of pranayama practices on breastfeeding. Nonetheless, it is proposed that pranayama practices included in postpartum yoga calm mothers down and direct them to their infants, which encourages the mothers to breastfeed their infants more frequently.
Asana, meanwhile, the physical postures of yoga practice, provides a form of exercise since it requires active and/or passive participation of the muscle groups.15,19 Although many women experience fatigue and exhaustion in the postpartum period, these can be reduced by systematic body movements 21 and in their study, Karbandi et al. determined that relaxation exercises increased breastfeeding self-efficacy in postpartum women. 22 In their study, Bender et al. also determined that relaxation exercises performed in the postpartum period encouraged women to breastfeed. 23
Then, meditation, which is the last stage of yoga practice, helps the mother to feel good and move away from negative thoughts. 24 In a study carried out by Kawanishi et al. on pregnant women, meditation during yoga practice was found to eliminate the pressure and tension felt by a mother-to-be, while promoting the development of the self and increased feelings of love and compassion. 25 Perez-Blasco et al. determined that 8 weeks of meditation practice increased breastfeeding self-efficacy and decreased the mothers' stress and depression. 21 It is proposed that yoga performed during the postpartum period will help a mother to cope with the stressors during this period, relax her, and increase the success of her breastfeeding. 15
In our study, the mean MAS scores of the mothers in the experimental group after the yoga practice were determined to be significantly higher than those of the mothers in the control group. In the literature, it has been determined that yoga is psychologically good for mothers and positively contributes to mothers' attachment to their babies by increasing the communication between mother and baby.25–30 The results of our study are similar to those found in the literature.
It is worth highlighting, however, that in our study, it was determined that the mean MAS scores of both groups after 8 weeks were higher than those before (p < 0.05), which supports the notion that maternal attachment is a special and meaningful relationship that develops between an infant and mother over time. In their study, Barone et al. determined that maternal attachment before a baby's birth, which was termed prenatal attachment increased with gestational age, suggesting that the development of the relationship between the mother and baby grows even before the baby enters the world and the two of them meet. 31
Conclusion
After yoga practice, there was a statistically significant increase and improvement in the breastfeeding self-efficacy and maternal attachment of the experimental group (p < 0.05). In accordance with the results obtained from the study, health care professionals serving in the postpartum period are recommended to take into account the factors that would affect breastfeeding and maternal attachment of mothers and to take steps to improve their physical and psychological health. To support the findings of the study, it may be recommended to work with mothers with different sociodemographic and obstetric characteristics in larger sample groups at different times.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by İnönü University Scientific Research Projects (TDK-2017/852).