
Abstract
Background:
Infants with congenital heart disease (CHD) are at risk for feeding-related morbidity and mortality, with growth failure and oral feeding problems associated with poor outcomes. The benefits of human milk (HM) for preterm infants have been well documented, but evidence on HM for infants with CHD has recently begun to emerge.
Objectives:
Our primary aim was to examine the impact of HM feeding on outcomes for infants with CHD.
Methods:
Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines, a search was conducted using MEDLINE, CINAHL, and Cochrane Database of Systematic Reviews. The quality of each study was assessed using the Joanna Briggs Critical Appraisal Tools. A total of 16 studies were included.
Results:
There was evidence that an exclusive HM diet reduces the risk of necrotizing enterocolitis (NEC) for infants with CHD. Evidence with a higher risk for bias indicated that a well-managed HM diet may be associated with improved growth, shorter length of stay, and improved postoperative feeding and nutritional outcomes. Chylothorax outcomes were similar between modified HM and medium-chain triglyceride formula. The studies had significant limitations related to power, lack of control for covariates, and inconsistent delineation of feeding groups.
Conclusions:
Based on the reduced risk for NEC and given the conclusive benefits in other vulnerable populations, we recommend that clinicians and institutions prioritize programs to support HM feeding for infants with CHD. Large high-quality studies are needed to validate these results. Future work should clarify best practices in managing an HM diet to support optimal growth and development for these infants.
Introduction
Congenital heart disease (CHD) is the most common congenital anomaly, with nearly 1 in 100 infants affected. 1 Over the past four decades, surgical improvements have resulted in reductions in mortality of up to 38%.2,3 Most children with CHD are now expected to survive to adulthood, and attention is turning to improvement of developmental outcomes, with feeding a major area of concern. Infants with CHD are at high risk for feeding-related morbidity and mortality, with growth failure and oral feeding problems associated with negative surgical and developmental outcomes.4,5 Furthermore, family caregivers experience enormous stress around feeding, with feeding problems often cited as the number one concern—even above the cardiac condition.6,7
Best practices for feeding infants with CHD are not well established, and there is documented variation in practice among providers and clinical sites.8–10 This variation can lead to inconsistent and confusing communication about feeding practice between health care teams and family caregivers,11,12 which may lead to decreased trust or confidence in the treatment team, compromised parental mental health, and negative consequences for infant outcomes.11,13,14
Human milk (HM) is considered the nutrition of choice by national and global health organizations.15,16 For infants with CHD, multifactorial challenges related to clinical course, parent–infant separation, and lack of institutional support can lead to low rates of HM feeding and direct breastfeeding.17–19 The benefits of HM for vulnerable infants in the neonatal intensive care unit (NICU) have been well documented, 20 but a body of evidence focused specifically on HM feeding for infants with CHD has only recently begun to emerge.
A recently published Delphi study revealed general clinical consensus as to the importance of HM feeding in this population, but limited evidence to guide best practices, and highlighted the critical need for clinical guidelines on HM nutrition management for infants with CHD. 21 Currently, there is no systematic review examining the associations of HM on outcomes for infants with CHD. A 2019 narrative review is informative, 22 but several relevant studies have been published in the past 3 years and are not included in the 2019 review.
Therefore, the aim of this systematic review was to determine whether there are differences in outcomes for infants with CHD who receive HM feeding, compared with other types of feeding. Secondary aims were to examine how HM feeding groups are defined in CHD infant feeding research, and to identify whether there are any harms associated with an HM diet in this population. By critiquing and synthesizing the available literature, this review provides evidence to inform clinical guidelines, and identifies gaps in the literature as foci for further study.
Methods
Operational definitions
For the purposes of this review, operational definitions are as follows: (1) “Infants” are children <1 year of age. (2) “Congenital heart disease” is determined by confirmed clinical diagnosis. (3) “Human milk feeding” will be defined per study, and an examination of how this is defined is a secondary question of interest. (4) “Other types of feeding” will be defined per study and may include formula feeding, bovine-based fortification, or nothing by mouth (npo). (5) “Outcomes” will not be defined a priori, but will be defined per study.
Due to high variability in terminology, “human milk” will be used as an umbrella term to indicate mother's own milk (MOM) and/or donor HM, with the recognition that these two nutritional forms are not interchangeable. 23 An investigation of differences associated with the route of nutrition (e.g., direct latch at the breast, bottle, nasogastric tube) is beyond the scope of this review.
Search strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, 24 a literature search was conducted with the assistance of a university-based health sciences librarian, using MEDLINE (accessed via Ovid MEDLINE® and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, 1946 to 2021), CINAHL, and Cochrane Database of Systematic Reviews. Key subject headings included “human milk,” “breast feeding,” “heart defects, congenital,” “cardiac surgical procedures,” “infant,” and “infant, newborn.” Related keywords were added with truncation for maximum results. The search was limited to human subjects and English-language results, and review articles were excluded. The full Ovid MEDLINE search strategy can be seen in Table 1.
Sample Search Strategy Using Ovid MEDLINE
.mp, keyword search; exp “”/, subject heading search; *, term truncation.
Study selection
Articles were imported into Rayyan QCRI 25 and duplicates were removed. An initial blinded screen by title and abstract was completed by two reviewers (K.M.E. and A.C.M.). Studies that appeared to fit the inclusion criteria and those with abstracts without enough information to determine eligibility received a blinded full-text review by the same two reviewers. Reference lists of included studies were examined for additional eligible publications. Any disagreements were solved through consensus.
Articles were included in the review if (1) the study population was infants with clinically diagnosed CHD; (2) the impact of HM on outcomes for infants with CHD was a primary or secondary focus; and (3) the article reported findings from an original research study, including observational, quasiexperimental, or experimental designs. Conference abstracts were considered if there was enough information available to make a quality assessment.
Articles were excluded if (1) the study population was focused on infants with a primary diagnosis other than CHD (e.g., a genetic syndrome); (2) the article was written in a language other than English; (3) the article was not original research (e.g., review, expert opinion); and (4) the article reported findings from a case study or a quality improvement project. The search resulted in 483 records. After deduplication, title and abstract review, and full-text examination, 16 articles were included in the review. Figure 1 is a PRISMA flow diagram of the search process.
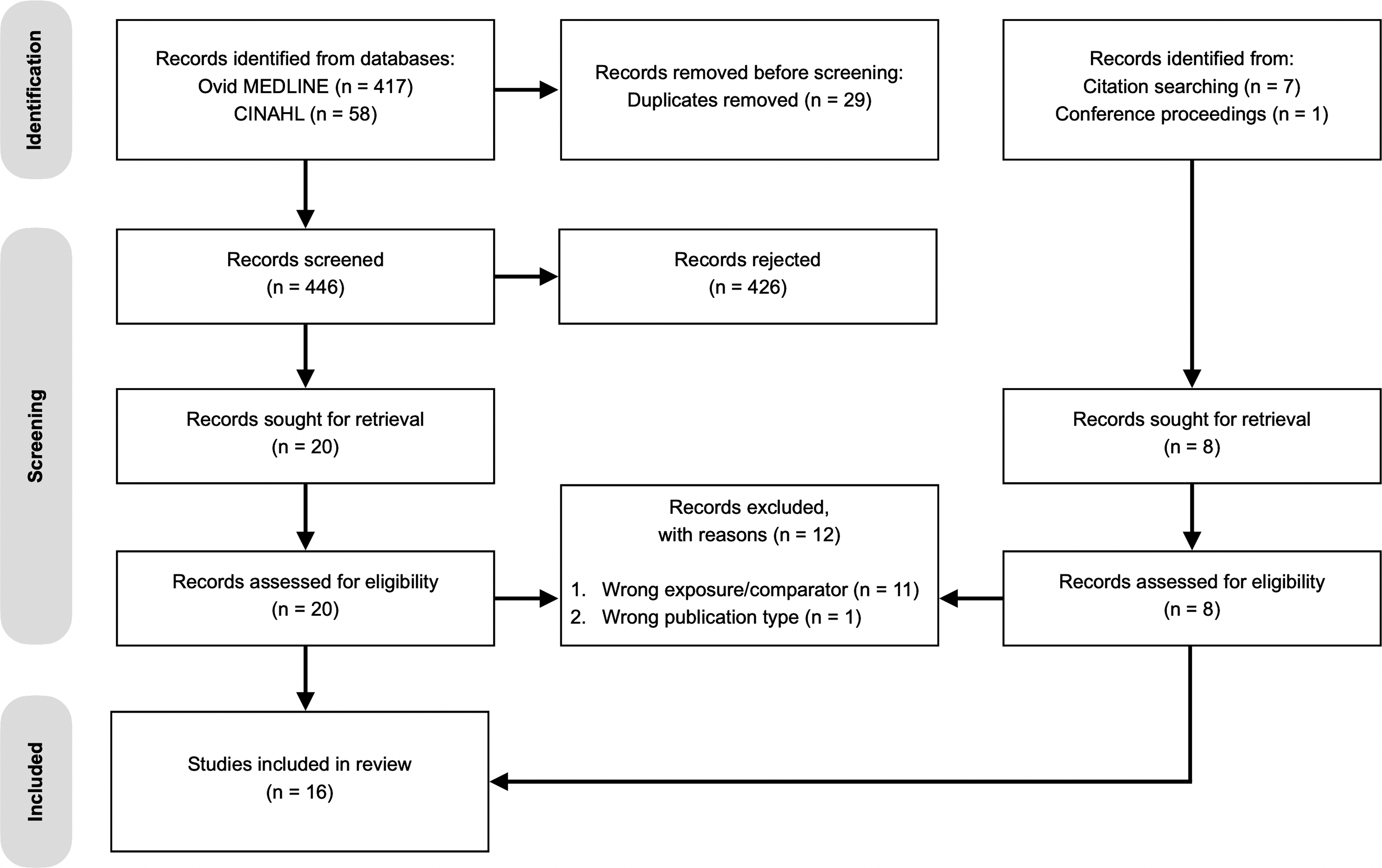
PRISMA flow diagram of the search process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Data extraction and quality assessment
Data from the included studies were extracted by one author (K.M.E.) and validated by a second author (A.L.T. or K.M.S.). Information collected included citation, study methods, sample characteristics, results, limitations, and funding sources. First authors were contacted for missing data.
The methodological quality of each study was assessed using the Critical Appraisal Tools from the Joanna Briggs Institute. 26 These are a collection of reliable, validated, design-specific tools that can be used to evaluate the quality of observational, quasiexperimental, and experimental studies. An initial quality assessment was conducted by the first author (K.M.E.), with a second blinded assessment by an additional author (A.C.M., E.N.S., N.M.S., or K.M.S.). Any disagreements were solved through consensus.
Results
Study characteristics
A total of 16 articles met the final inclusion criteria. Nine were cohort studies (seven retrospective27–33 and two prospective34,35), four featured a quasiexperimental design,36–39 two were randomized-controlled trials (RCTs),40,41 and one was a retrospective case/control design. 19 One RCT included multiple sites, 40 and two studies were secondary analyses of multisite data sets.19,32 The studies took place most often in the United States (n = 10), with Canada (n = 3), China (n = 1), Germany (n = 1), and Italy (n = 1) also being represented. A summary of characteristics of the included studies can be found in Table 2.
Summary Description of Included Studies
ø = no significant differences.
Due to variability in terminology, we have opted to use HM as a general term representing MOM and/or DHM. The specific terminology used by each study is reported in this column, with a description as provided by the authors. Whenever possible, we have indicated when the study differentiates between MOM and DHM.
Study was an open-label clinical trial; participants receiving ≥50% of feeds as HM were randomized to one of two modified HM groups; others assigned to the MCT formula group.
The authors categorize this as a retrospective study; however, participants were prospectively enrolled and assigned to a modified HM group or a formula feeding group.
BiV, biventricular physiology; BM, breast milk; CHD, congenital heart disease; CT, chest tube; DD, ductal dependent; DHM, donor human milk; HAZ, head circumference-for-age z-score; HC, head circumference; HLHS, hypoplastic left heart syndrome; HM, human milk; ICU, intensive care unit; L/M, lactulose/mannitol; LAZ, length-for-age z-score; LOS, length of stay; MCT, medium chain triglyceride; MOM, mother's own milk; NEC, necrotizing enterocolitis; NICU, neonatal intensive care unit; NPO, nothing by mouth; PGE, prostaglandin E1; RCT, randomized-controlled trial; SV, single ventricle physiology; WAZ, weight-for-age z-score; WLZ, weight-for-length z-score.
Sample
There were a total of 8,176 participants in the 16 included studies.* These participants were newborns diagnosed with complex CHD,27,29,32 medically stable newborns with CHD, 34 infants undergoing cardiac surgery for CHD,19,30,31,33,35,38,40,41 or infants with CHD diagnosed with chylothorax after surgery.28,36,37,39 Participants were 60.3% male and 39.7% female (female sex was often presumed, as only six studies reported female numbers). Only seven studies reported details of race and ethnicity.19,27–29,32,33,35 Of 7,659 infants, 56.5% identified as white, 26.5% as Hispanic, 11.7% as black, 0.3% as Asian, and 5.0% as other. Social determinants of health were reported in three studies, with Kocel et al. 36 and Siemienski et al. 35 detailing parental level of education, and McCrary et al. 33 reporting the percentage of patients receiving Medicaid.
The age of the participants was most often reported at three time points, depending on the study aim. Gestational age, age at surgery, and/or age at chylothorax diagnosis. The mean or median gestational age was >37 weeks in 11 studies,19,27–30,33,36,37,39–41 >36 weeks in another, 32 and unreported in 4 studies.31,34,35,38 Age at surgery was mean or median <3 months for all five studies reporting this metric.28,31,33,38,41 Age at chylothorax diagnosis varied, with four studies reporting a median range of 0.6–5.3 months.28,31,36,37
Weight was also reported at the same three time points. The mean or median birth weight was >3.0 kg in seven studies,19,28–30,36,39,41 while Rosti et al. reported a birth weight range of 2.1–4.1 kg. 30 Two other studies reported birth weights as percentages, with 77.4%> 2.5 kg in Becker et al. 32 and 93.4%> 2.0 kg in Cognata et al. 27 Blanco et al. reported that 86.9% of infants were average or large for gestational age, 40 and the remaining five studies did not report birth weight.31,33–35,38 Mean weight at surgery ranged from 2.6 to 4.0 kg in the three studies that provided these data,28,30,38 while McCrary et al. reported a mean weight-for-age z-score (WAZ) at initial shunt placement of −0.61. 33 Mean weight at chylothorax diagnosis varied, from 3.2 to 5.9 kg.36,37,39
Three studies provide information about length and head circumference at birth and/or chylothorax diagnosis.36,37,39 The median length at birth ranged from 47.5 to 51.0 cm,37,39 while the median length at diagnosis was between 51.0 and 61.1 cm.36,37,39 The mean or median head circumference at diagnosis ranged from 34 to 39.3 cm.36,37,39
CHD diagnoses included both single ventricle (SV; n, % 3,291, 40.3) and biventricular (BiV; 4,885, 59.7) defects. Transposition of the great arteries was the most common BiV diagnosis, and hypoplastic left heart syndrome (HLHS) the most common SV physiology. Information about the diagnoses of the sample can be found in Figure 2.

Primary cardiac diagnoses of participants in the included studies.
Exclusion criteria varied among studies. Eight studies excluded infants with noncardiac congenital anomalies or genetic syndromes,27,29,30,35,38–41 and two studies excluded premature infants born <32 weeks.33,37 Three studies excluded infants with noncomplex CHD (e.g., not requiring intervention or prostaglandin E1 infusion),27,29,32 while Yu et al. excluded infants with complex CHD requiring staged surgery. 38 Six studies excluded infants who experienced a complicated clinical course or death (e.g., preoperative necrotizing enterocolitis [NEC], chylothorax, extracorporeal membrane oxygenation, hemodynamic instability, or no enteral feeding).29,30,36,38,40,41
HM feeding definitions
In six studies, infants in HM feeding groups received 100% MOM or donor HM.27,29,30,32,38,40 In one of these, infants in the HM feeding group received HM-based fortifier (Prolacta), while the comparison group received bovine-based fortifier. 40 Two additional studies implied that HM feeding groups received 100% HM, but were unclear regarding MOM, donor HM, and/or fortification.19,41 Four studies on treatment of chylothorax defined HM feeding groups as receiving low-fat MOM or donor HM with some type of fortification, such as medium-chain triglyceride (MCT) oil, MCT formula, soybean oil, or bovine-based HM fortifier.28,36,37,39 Three of these studies considered varying amounts of formula supplementation acceptable in an HM diet, with ≥50%, 39 ≥75%, 28 or ≥80% 36 required for HM feeding group eligibility.
Siemienski et al. defined a “breast milk predominant” group as receiving primarily HM (defined as MOM or donor HM) throughout the first year of life. 35 In the final three studies, HM feeding was not clearly defined and allowed for any amount of HM, which led to a lack of differentiation between groups.31,33,34 For example, in Boctor et al., 6 out of 10 infants in a “breastfed” group were fed MOM supplemented with formula, with no information available about HM dose. 31 Combs and Marino defined “breastfed” as any amount of MOM, 34 while McCrary et al. compared infants with any “breast milk use” (with MOM or donor HM unspecified) with those with none. 33
Findings
Outcomes examined in the studies can be grouped into four main categories: (1) incidence of NEC, (2) outcomes related to treatment of chylothorax, (3) weight gain, and (4) other postoperative outcomes. All significant results with point estimates can be found in Table 3.
All Significant Outcomes Found in Included Studies, with Effect Size
The terminology used for feeding types is as per the authors of each individual article. Specification regarding MOM and/or DHM is provided in parentheses, whenever possible. If the authors were unclear as to the source of the HM, the original terminology is provided. Additional details about study definitions of HM feeding groups are available in Table 2.
n (%).
Odds ratio (95% confidence interval).
At stage I palliation surgery discharge.
Mean (standard deviation).
Median (interquartile range).
Median (range).
No difference at baseline.
Feeding intolerance is defined as: The infants had symptoms, such as gastric retention and vomiting, and gastric retention was more than 50% of the previous total feeding amount. Physical examination revealed increased bowel sounds and abnormal abdominal tenderness.
Dyspeptic diarrhea is defined as: Defecation multiple times a day, mostly in the morning or after feeding, and mushy and watery stool, with a pungent odor.
BF, breastfed; BM, breast milk; BMF, breast milk fed; DHM, donor human milk; HAZ, head circumference-for-age z-score; HM, human milk; ICU, intensive care unit; LAZ, length-for-age z-score; LOS, length of stay; MCT, medium chain triglyceride; MOM, mother's own milk; NEC, necrotizing enterocolitis; WAZ, weight-for-age z-score.
Necrotizing enterocolitis
Six studies examined the associations between an HM diet and NEC.19,27,29,32,40,41 An HM diet was associated with a lower incidence in NEC in five studies, with three results reaching significance.19,27,40 Cognata et al. found that an exclusive unfortified HM diet resulted in 83% lower odds of preoperative NEC, after controlling for cardiac lesion, race, feeding volume, small-for-gestational age birth weight, inotrope use, and prematurity. 27
Blanco et al. reported a reduced incidence of NEC and suspected NEC in infants receiving HM plus HM-based fortifier, compared with HM or formula plus bovine fortifier (3.6% versus 15.4% incidence), 40 while Lopez et al. found that infants with HLHS who developed NEC during the initial hospitalization were more likely to be receiving an exclusive formula diet at hospital discharge (n = 35, 61%) than those without NEC (n = 39, 29%). 19
The only study that reported a higher incidence of NEC in an HM feeding group had only three infants who developed the disease (2 in a trophic HM group, and 1 nil per os). 41 In Cognata et al. 27 and Kataria-Hale et al., 29 a diagnosis of NEC was determined by Bell's modified criteria and reviewed by two neonatologists and a radiologist to determine staging. Blanco et al. 40 and Zyblewski et al. 41 reported the modified Bell stage of the NEC cases examined, but did not provide details about who determined the diagnosis.40,41 Lopez et al. 19 and Becker et al. 32 completed secondary analyses of large national registries and were not able to verify a uniform grading system for diagnosing NEC.
Chylothorax
Four studies focused on outcomes related to the treatment of chylothorax with modified HM, compared with MCT formula.28,36,37,39 Two studies examining duration of treatment found that infants receiving modified HM experienced shorter treatment,37,39 with the result in Neumann et al. reaching significance (41 days versus 67 days). 37 Two studies investigating the number of chest tube drainage days reported conflicting results, but neither was significant.28,36 Similarly, three studies recorded volume of chest tube drainage with inconclusive results.36,37,39 Hospital length of stay (LOS) was examined in two studies, with infants in the modified HM group experiencing a shorter LOS in both; however, differences were not significant.28,37
Changes in anthropomorphic measurements from chylothorax diagnosis to treatment end were examined in four studies, with mixed results.28,36,37,39 Kocel et al. found significant decreases in WAZ (−0.76) and length-for-age z-score (LAZ; −0.44) in the modified HM group, but not in the MCT group. 36 Similarly, the head circumference-for-age z-score increased in the MCT group (0.59), but not in the modified HM group. 26 In contrast, Fogg et al. reported a trend toward higher absolute growth velocity from baseline to discharge in the modified HM group, 28 while DiLauro et al. and Neumann et al. found no differences in any anthropomorphic measurements between feeding groups.37,39 Taken as a whole, most results related to physical growth during treatment for chylothorax were inconclusive.
Weight gain
Seven studies described weight-related outcomes,30,31,33–35,38,40 with findings in four studies reaching significance.31,34,38,40 Of these, three demonstrated improved outcomes for infants in HM feeding groups.34,38,40 Yu et al. reported improved average daily weight gain for postoperative infants receiving an HM diet (19.0 g/kg/day versus 14.4 g/kg/day), 38 while Combs and Marino found that, by 5 months after discharge, more infants who were bottle fed experienced >20% negative change in weight percentile (83% versus 46%). 34 Blanco et al. reported that, from birth to the end of the study period, infants fed HM-based fortifier experienced a higher median weight velocity than those fed with bovine fortifier (3.62 g/kg/day versus 2.79 g/kg/day). 40
In contrast, Boctor et al. found significant differences in median weight change at discharge between infants who were exclusively directly breastfed (−49 g/day), fed a combination of HM and formula (5 g/day), or 100% formula fed (20 g/day). 31 The results in McCrary et al. did not reach significance, but trended toward a higher WAZ for palliated infants in the HM feeding group at the first clinic visit after discharge (−1.5 versus −1.78, p = 0.12), and at shunt takedown (−1.21 versus −1.60, p = 0.058). 33 The remaining two studies found no difference between the feeding groups.30,35
Other postoperative outcomes
HM feeding was associated with a shorter postoperative LOS in five of the six studies examining this outcome.28–30,37,38,40 Only the results in Yu et al. reached statistical significance, with shorter hospital (13.9 days versus 17.8 days) and intensive care unit (ICU, 6.0 days versus 8.1 days) LOS for the HM feeding group. 38 Yu et al. also found that infants fed with HM were started on enteral feeds earlier (27.8 hours versus 50.4 hours), and achieved full feeds in 3.0 days versus 5.2 days. 38 Infants in this study also experienced improved outcomes in several markers of nutritional status (prealbumin, albumin, and anemia) and incidence of complications (feeding intolerance, dyspeptic diarrhea, and nosocomial infection). 38 Additional information about these outcomes can be found in Table 3.
Quality of evidence
The quality of evidence of each of the included articles was appraised using the Joanna Briggs Critical Appraisal Tools, 26 with results presented in Table 4. It should be noted that quality assessment was focused solely on the strength of evidence as related to HM feeding and outcomes for infants with CHD, which was not a primary focus of all studies. The assessment does not necessarily reflect the strength of studies in regard to other outcomes.
Quality Assessment Using the Johanna Briggs Institute Critical Appraisal Tools
Reasons for an “unclear” or “no” rating as to the reliability of outcome measurements in all study designs were generally related to diagnosis criteria for NEC or means of weight/anthropomorphic measures. Regarding NEC diagnosis, Becker et al. 32 and Lopez et al. 19 did not use a standardized grading system (e.g., modified Bell staging). Regarding weight or anthropomorphic measurements: Blanco et al., 40 Boctor et al., 31 Fogg et al., 28 McCrary et al., 33 Neumann et al., 37 Rosti et al., 30 Siemienski et al., 35 and Yu et al. 38 either rely on retrospective chart data, which are subject to inconsistency, or do not describe a standardized process of measurement. The study from Combs and Marino 34 included weights from maternal self-report, with no standardization of measurement.
✓, yes; X, no; ?, unclear.
NEC, necrotizing enterocolitis.
As a group, the HM findings from the 16 studies exhibited methodological issues that call into question the validity of the results. Only four studies described clear, reliable outcomes measures (e.g., diagnosis of NEC and methods to track weight or other anthropomorphic measurements).27,29,36,39
Seven of the nine cohort studies were retrospective chart reviews,27–33 with inherent bias in data collection due to potential differences in accuracy between electronic health record users and potential for missing data. Most of these cohort studies did not report on baseline differences between feeding groups, with only Rosti et al. providing satisfactory evidence that the feeding groups were similar at study initiation. 30 Of the four quasiexperimental studies, two did not confirm clear differentiation between the feeding groups, with some infants in HM groups consuming an appreciable amount of formula.36,39
All but four studies19,27,29,39 exhibited risk for bias regarding sample size, power, or statistical analysis, although this is understandable considering the small population and rare outcomes under study (e.g., NEC). Ten studies had very small samples or low incidence of outcomes (e.g., NEC), and/or did not provide information on whether power was adequate for HM-related outcomes.28,30–37,41 Five studies controlled for covariates,27,28,30,39,40 but it was unclear whether four of these were powered for all outcomes.28,29,39,40 For example, Blanco et al. reported sufficient power for the primary outcome of weight velocity, but were unclear as to the power for NEC outcomes. 40
Yu et al. completed a power analysis but did not control for covariates, and used potentially inappropriate tests for categorical variables with low frequency. 38 Becker et al., Boctor et al., and Combs and Marino reported large amounts of missing data 32 or lacked adequate description of analytical methods,31,34 which were significant limitations for results related to HM feeding.
Discussion
This review identified 16 articles that examined the impact of an HM diet in infants with CHD during the hospital stay. With the existing evidence, it is difficult to conclusively answer the primary research question regarding differences in outcomes between infants with CHD who receive HM, compared with other types of feeding. The result with the highest level of certainty relates to the incidence of NEC. There is evidence that the incidence of NEC is lower in infants with CHD who are fed HM,27,29,32 with Cognata et al.'s 27 well-designed retrospective cohort study and Blanco et al.'s 40 RCT both reporting significantly lower NEC with an exclusive HM diet. Both of these studies included modified Bell staging to determine diagnosis.
In Lopez et al., infants with HLHS who developed NEC during the initial hospitalization and survived to stage I palliation discharge were less likely to be receiving any HM at discharge. 19 In this study, it should be noted that the type of feeding was reported at hospital discharge rather than before NEC development. While it is plausible that an infant's feeding plan at hospital discharge is reflective of the nutrition received during the hospital stay, it is not certain that the infant received a 100% HM diet during the hospital stay. For example, not all hospitals utilize pasteurized donor HM as a bridge to MOM. In this case, an infant may be exposed to infant formula as the lactating parents are developing their milk supply.
It is also possible that HM provision could have been negatively impacted by a complicated clinical course, lack of adequate support for the lactating parents in establishing milk supply, or provider or institutional preference—all of which could result in nutrition changes throughout the hospital stay. Thus, infants in Lopez et al.'s study may have been exposed to formula during their hospitalization, even if their feeding method at discharge was noted as 100% HM. In addition, this study is a secondary analysis of the National Pediatric Cardiology Quality Improvement Collaborative registry, which includes ∼60 cardiac centers across the United States. The authors note that the criteria for NEC diagnosis were not standardized among institutions, which is a further limitation.
Overall, the findings in this review lend support to the hypothesis that HM is protective against NEC in infants with CHD. This is consistent with previous findings in the very low birthweight and preterm populations,42,43 and reveals that an HM diet offers protection against this potentially devastating disease. However, there may be some concerns that an exclusive HM diet could prevent NEC while resulting in slower growth. For example, Chowning et al. reported a dose-dependent relationship between exclusive HM feeding, decreased NEC, and decreased weight gain in very low birth weight neonates. 44
In the current review, only one study examined the impact of HM feeding on both NEC and growth outcomes. 40 Blanco et al. found that infants fed exclusive HM with HM-based fortifier demonstrated initial slower growth than infants fed bovine-based fortifier. 40 By day 30 of life, growth in the HM-based fortifier group exceeded that of the bovine-based fortifier group, and this trend continued through the end of the study—a result consistent with recent evidence on HM-based fortifier for preterm and very low birth weight infants.45,46
Cognata et al. did not report growth outcomes; however, the focus of this study was on the development of NEC preoperatively, and most infants had surgery during the first 2 weeks of life (median 19.2 days for infants with ductal-dependent BiV physiology, n = 119; 9.2 for all others, n = 427). 27 Considering the potential for clinical instability during the preoperative time, growth trends during the study period may not have been well established. While the results from Blanco et al. indicate that an exclusive HM diet with HM-based fortifier allows for both reduced risk for NEC and improved physical growth, future studies should investigate strategies to support growth with an exclusive HM diet when HM-based fortifier is not available.
Chylothorax
Chylothorax is another rare but serious complication of cardiac surgery, and treatment with a modified HM diet is a relatively new approach, with the first case study on this process published in 2004. 47 In the context of care for chylothorax, outcomes were generally not different between modified HM groups and infants receiving MCT formula. While Neumann et al. reported significantly fewer treatment days for infants in a modified HM group, their results are skewed by one infant who received an MCT formula diet for 230 days. 37 Considering the small sample size of the MCT group (n = 10), the true difference between groups is likely much lower. Differences in other treatment outcomes (e.g., number of chest tube days, volume of chest tube drainage, and LOS) were not significant.
The impact of a modified HM diet on growth in the context of chylothorax was inconclusive. Kocel et al. 36 reported significant decreases in WAZ and LAZ from baseline, but included only 16 infants with a lack of definition between feeding groups. For example, infants in the modified HM group received as little as 45% modified HM, with the remainder supplemented by MCT formula. 36 Conversely, 3 (38%) infants in the MCT group required parenteral nutrition between 5 and 19 days, compared with none in the modified HM group. 36 This variation in feeding practice highlights the difficulty of conducting feeding research in infants with CHD—particularly when examining a rare outcome, such as chylothorax.
The remaining three studies found no significant differences in growth outcomes, although DiLauro et al. caution that they did not recruit the most severely ill infants, who may have been at highest risk for growth failure. 39 In addition, all studies examining the use of modified HM in chylothorax included small samples (n ≤ 35), and it is possible that different groups may experience different results. Based on the available evidence, it appears that treatment of chylothorax with modified HM is a viable alternative to formula-based nutrition plans, with similar results related to chest tube volume and duration, treatment duration, LOS, and growth.
High-quality evidence including larger sample sizes is needed to clarify the impact of modified HM on outcomes related to chylothorax. It is also important to note that all four studies examining chylothorax outcomes in this review used a centrifuge to create low-fat HM,28,36,37,39 with one of these providing parents with the option of portable centrifuges to use at home. 39 It is understandable that many hospitals in North America many not have the resources to implement centrifuge-based skim milk programs for chylothorax. Institutions would require a strong HM culture, along with financial and personnel resources to implement this type of program. 48
Other less expensive methods of modifying HM for chylothorax treatment have been described. 49 Further testing of these methods in the CHD population is warranted, and should include qualitative methods to investigate any potential burden for families and hospital staff.
Weight gain
Impaired weight gain and physical growth can be a major concern for infants with CHD due to increased risk for poor surgical and developmental outcomes4,5,50 and psychological stress for family caregivers.6,7 It is difficult to compare growth outcomes between studies in this review, due to differences in feeding groups, outcome measures, and length of follow-up. For example, four studies compared “breastfeeding” or “breast milk” groups with “formula,” or “bottle” groups.31,33,34,38 In three of these studies, infants in the breastfeeding groups were not required to receive exclusive HM.31,33,34
Other studies examined HM feeding compared with standard or high-calorie formula, 30 predominant breastfeeding compared with mixed feeding or exclusive formula, 35 or HM-based fortifier compared with bovine-based fortifier. 40 Older studies may not reflect current practices regarding postoperative or interstage fortification. Anthropomorphic measures also varied among studies (e.g., average daily weight gain,30,31,38,40 percentage of weight change, 34 and WAZ33,35), and length of follow-up ranged from the initial postoperative hospital stay30,38 to the first year of life. 35
Despite these limitations in study design, there appears to be some evidence that a well-managed HM diet may support improved weight gain for infants with CHD. Blanco et al.'s recent RCT reported that infants with SV CHD who received HM-based fortifier had greater weight velocity from birth to the end of the study than those on bovine fortifier. 40 Similar results have been found in other surgical congenital populations. 51 As Blanco et al.'s results were available only as a conference presentation, it was not clear whether the findings were adjusted to reflect the time that infants spent in the study, as length of participation varied due to infant clinical course. Full published results are needed to verify the strength of these findings.
Additional studies supported increased growth for infants receiving HM, with Yu et al. reporting significantly increased average weight gain for infants on exclusive HM diets, 38 while Combs and Marino found that infants in HM feeding groups tended to lose less weight at 5 months postdischarge. 34 Both of these studies exhibit risk for bias related to design and analysis. While McCrary et al. reported that infants fed any HM tended to lose less weight at shunt palliation takedown surgery (at mean 5.6 ± 2.7 months), the authors cautioned that weight gain was insufficient for all infants in their cohort, and baseline differences between the HM and non-HM groups were not well described.
The only study that demonstrated inferior weight-related outcomes for infants in HM feeding groups has serious design flaws (e.g., crossover between feeding groups; heterogeneous diagnoses and age groups; small sample; statistical analysis not well described) and does not reflect current practice. 31 The remaining studies revealed no significant differences in weight gain between infants receiving HM and those receiving other diets.30,35 Taken as a whole, the results tentatively indicate that a well-managed HM diet—potentially including an HM-based fortifier when needed—may result in similar or improved weight-related outcomes for infants with CHD, although the evidence exhibits risk for bias.
High-quality, carefully designed studies are needed to fully understand the impact of HM feeding on weight gain and physical growth, so that best practices in managing an HM diet can be identified. Moreover, future research should investigate the impact of nutrition on the quality of growth outcomes for infants with CHD. Previous work in the preterm population reveals that infants fed with HM or direct breastfeeding experience slower initial weight gain, but ultimately better neurodevelopment 52 and recovery of body composition through fat-free mass deposition. 53 Infants with CHD are at risk for impaired neurodevelopment, 54 and inadequate growth has been shown to be associated with poor neurodevelopmental outcomes. 50
However, the relationship between nutrition type (e.g., MOM, pasteurized donor HM, formula, and bovine or HM-based fortifier) and growth quality has not been examined in infants with CHD. The potential impact of HM feeding on neurodevelopment for these infants is an important direction for future research.
Other postoperative outcomes
The association between an HM diet and LOS was examined frequently, with five of six studies finding that infants in HM feeding groups had a shorter hospital LOS. The statistically significant result in Yu et al. should be interpreted with caution, as this study did not control for potential covariates (e.g., age and diagnosis). 38 In addition, the authors note that infants in the formula feeding group often lived in rural areas, with parents who could not always travel to the surgical center. It is possible that this disparity in health care access could have delayed discharge or may have impacted outcomes in other unmeasured ways.
Future studies with large sample sizes and robust analytical techniques should carefully examine the impact of HM on hospital LOS, as a reduction in LOS by even 1 day has clinical implications for lower hospital costs and benefit to families.
Yu et al. also reported differences in other postoperative feeding outcomes, with infants in the HM groups beginning enteral feeds earlier and achieving full feeds sooner. 38 Similar results in faster achievement of full feeds have been noted in some preterm populations.55,56 For Yu et al., criteria for beginning enteral feeds included resumption of bowel sounds, typically on postoperative day 2–4, with feeds advanced based on gastric residuals. The authors present hypotheses for faster achievement of full feeds, but do not discuss potential reasons for earlier feeding readiness in the HM group, which could have been impacted by unmeasured covariates (e.g., variation in feeding based on individual clinician preference and level of family engagement/advocacy for feeding).
Multisite studies with larger samples are needed to corroborate these findings, particularly as postoperative feeding practices are highly site and provider specific. 9 Yu et al. found additional benefits of HM feeding related to markers of nutritional status and incidence of complication. 38 Many of these analyses included low numbers and were likely not powered to detect true differences. Further evidence is needed to validate the results described in this study.
Definition of HM feeding
Studies focused on HM feeding have been historically imprecise in defining what constitutes an HM feeding group. 57 The 16 studies in this review exhibit notable variation in delineating HM feeding, with 10 studies providing either no clear definition of HM feeding,19,35,37,41 or allowing infants in HM groups to consume significant amounts of formula.28,31,33,34,36,39 While it should be noted that examining HM feeding outcomes was not the primary aim of Becker et al., this study assessed infant nutrition type on the day of NEC diagnosis, and assigned 5 (24%) infants to HM or formula feeding groups based on this data point. 32 The remaining 16 (76%) infants diagnosed with NEC were not included in the analysis due to missing feeding data on the day of diagnosis.
The ambiguity in feeding group assignment in the studies under review complicates pooling of results and cross-study comparison. While there are ethical challenges inherent in researching HM feeding, it is difficult to make recommendations based on studies with multiple treatment interference, or with large amounts of missing data. Several recent studies addressed this problem by providing pasteurized donor HM for infants who were not able to receive 100% MOM,27,29,40 although it should be noted that pasteurized donor HM is not an equivalent substitute for MOM.58–60
Future studies should explore HM dose/response. Many studies in the current review allowed infants in an HM group to consume significant amounts of formula (e.g., range of up to 65% in Kocel et al. 36 ), or considered an HM feeding group to include any amount of HM.31–34 Kataria-Hale et al. hypothesize that their nonsignificant association between preoperative HM feeding and postoperative NEC may have been different if they had been able to calculate HM dose. 29
To our knowledge, no study has quantified the amount of HM received by infants with CHD or analyzed volume-associated differences in outcomes. Accurate methods to measure HM transferred via direct breastfeeding exist (e.g., test weighing), 61 and can be used to quantify volume for those infants who are not receiving exclusive expressed HM.
Harms
In the included studies, there were no harms associated with an HM diet. There is a need for well-designed, prospective research on the best ways to support long-term physical growth through an HM diet in this population, but the results in this group of studies indicate that an HM diet is not harmful to growth or development, and may in fact support physical growth. Given the well-documented nutritional, immunological, and relational benefits of an HM diet in both the healthy newborn population and in those needing NICU care, 43 the benefits of a well-managed HM diet outweigh any potential risks.
Clinical implications
Considering the evidence supporting decreased odds for preoperative NEC in infants with CHD who receive exclusive HM feeding, the possibility that an HM diet may decrease hospital LOS, the potential for improved postoperative feeding and nutrition outcomes, and the finding that a well-managed HM diet may support improved growth, we recommend that clinicians and health care systems make a concerted effort to support an exclusive HM diet, potentially fortified with HM-based fortifier when needed, for infants with CHD both during the hospital stay and after discharge. This aligns with global health organizations, which agree that HM is the optimal nutrition for both typically developing and vulnerable infants.15,16,62
Clinicians should identify ways to support lactating parents in providing HM for their infant with CHD. Direct breastfeeding and HM expression are inherently challenging in the context of neonatal surgery and hospitalization,11,63 and infants with CHD are at particular risk for early weaning from HM.17,64 Furthermore, infants with CHD are often cared for at children's hospitals, potentially in a cardiovascular ICU. These institutional environments may not have a strong culture of prioritizing HM feeding and direct breastfeeding, in comparison with a birth hospital or an NICU. Previous research has demonstrated that parents of vulnerable infants born in a specialized birthing center inside a children's hospital were significantly more likely to initiate pumping and HM feeding for their infant with CHD, compared with infants born at an outside hospital. 65
This systematic review could serve as a call to action for institutions caring for infants with CHD. First, health care providers in these facilities should examine their current lactation services and ensure that they are providing comprehensive, evidence-based lactation interventions during the antenatal period, through birth, during the infant's hospitalization, and postdischarge. Second, health care institutions should examine their process of documenting enteral nutrition. Ideally, every enteral feed should be quantified to determine percentages of MOM, pasteurized donor HM, and infant formula so that percent exposure to HM could be calculated daily, weekly, and over the entire hospital stay.
Third, hospitals caring for infants with CHD should consider investing in the necessary equipment and personnel to implement a skim milk program. For an infant with CHD, the early weeks of life are often a time of crucial interventions, intended to optimize growth and development throughout the life span. Support of HM feeding should be a key component of this early development plan, requiring a concerted interdisciplinary, family-centered approach, including comprehensive, culturally responsive lactation services that include prenatal intervention, support for parental mental health, and evidence-based care. 66
Directions for future research
The current review demonstrates that there are major gaps in the literature to be addressed through future research. The overall quality of the current evidence has limitations, with issues of statistical power and analysis affecting the group of studies.
In addition, studies used varying or unclear criteria for feeding group assignment, with infants in HM feeding groups often receiving significant amounts of non-HM nutrition for supplementation or fortification. While fortification may be necessary for some infants with CHD, future research should be clear about the percentage of non-HM feeding that is acceptable for an infant categorized in an HM study group. Ideally, improvements in enteral nutrition measurement and documentation would allow for studies to determine whether there are dose/response differences in outcomes between infants receiving HM, formula feeding, and/or bovine-based fortifier.
While some recent studies exhibit more clarity in HM feeding group delineation,27,39,40 this review highlights the fact that CHD is inherently difficult to study. Physiological combinations of anomalies may be highly individualized, and two patients with the same diagnosis may experience very different clinical courses. 67 Research on nutrition for hospitalized infants with CHD is similarly complicated, as feeding plans can include various forms of nutrition and routes of nutrition delivery. It is challenging to tease apart the factors that interact to impact each infant's experience with CHD. Finally, clear standardization of outcome measurements would improve the quality of the evidence, particularly for rare diagnoses such as NEC and for growth-related outcomes.
Large multisite studies implementing high-quality, adequately powered prospective designs are needed to fully understand the impact of an HM diet on outcomes for infants with CHD, with robust statistical analysis that carefully controls for clinically relevant covariates. These studies should aim to clarify the current inconclusive evidence, with a particular focus on outcomes related to growth and physical development. Growth failure is associated with increased morbidity and mortality in infants with CHD,4,5 and a recent study highlighted the lack of evidence for best practices in managing growth with an HM diet in this population. 21
Therefore, future research should focus on exploring techniques for managing an infant's HM diet, which may include individualized fortification or separating the hindmilk of MOM.68,69 Future work should focus on describing the longitudinal impact of an HM diet on physical growth and development, and should consider dose-dependent outcomes. Multisite studies can provide power to determine differences in rare outcomes such as NEC; however, standardization of outcome measurements among sites is a key consideration, and may be challenging to implement.
Of note, fewer than half of studies in this review reported race or ethnicity,19,27–29,32,33,35 and only three offered any type of information on social or economic characteristics of the sample.33,35,36 There may be unexplored social determinants of health (e.g., structural racism and structural inequity) or barriers to health care access (e.g., distance from center and language barriers) that could play a role in the relationship between infant nutrition and health outcomes. 70 For example, Yu et al. mention that many of the infants in their formula feeding group came from rural families, who lived far from the tertiary hospital and could not travel to provide HM for their child. 38 This raises questions about differences in parental proximity or engagement that may have impacted health outcomes.
Future studies should report social and familial information, and should interrogate the ways in which systems and institutions contribute to inequities in HM-associated outcomes for infants with CHD, particularly given that factors such as parental race, country of birth, level of education, neighborhood, socioeconomic status, and maternal parity have been shown to impact HM feeding and direct breastfeeding in other vulnerable neonatal populations.71–73
In addition, the impact of parental mental health on infant feeding and health outcomes cannot be ignored. Previous literature demonstrates the negative impact of emotional and physiological stress on HM production,74,75 with higher levels of parental engagement and lower levels of anxiety and depression associated with improved HM outcomes. 76 Considering the potential for parental trauma in the context of a neonatal hospitalization, future work should adopt a holistic, culturally responsive, family-centered approach to HM research that acknowledges infant feeding as an innate, nurturing parental act of care, as opposed to merely a medical intervention to be measured and documented. 77
Strengths and limitations
The current review has several strengths. The search was conducted in multiple databases, with the assistance of an experienced health sciences research librarian. Reference lists were carefully examined for relevant publications. While non-English-language studies were excluded, a title review of non-English results identified no studies that appeared to meet the inclusion criteria. The review process included an in-depth methodological quality assessment by at least two independent reviewers, following the guidelines of validated critical appraisal tools. 26
Limitations include risk for bias in many studies; only one non-pilot RCT; a lack of information on social determinants of health and health inequities; and inconsistency in defining HM feeding among studies. The precise type of nutrition (e.g., MOM or donor HM) was often unclear. Sample sizes varied and many studies were not well powered, with subsequent issues for statistical validity.
While the review represents diverse CHD diagnoses, the exclusion criteria of several studies raise questions about the generalizability of the findings. For example, Yu et al. 38 report several significant results, yet include no infants with staged surgery for CHD, effectively eliminating infants who could be at the greatest risk for feeding-related morbidity and mortality. Similarly, DiLauro et al. 39 decided not to approach some unstable HM-fed infants undergoing treatment for chylothorax. Therefore, the results of this review may not fully describe the wide range of clinical experiences in the CHD population, with the sickest infants possibly underrepresented.
Conclusions
The current review included 16 studies reporting on the impact of an HM diet on outcomes for infants with CHD, compared with other types of feeding. Based on assessment using the Joanna Briggs Critical Appraisal Tools, 26 the studies with the strongest evidence indicated that an exclusive HM diet reduces the odds of NEC in this population. Studies with higher risk for bias revealed that an HM diet may be associated with a shorter hospital LOS, improved postoperative feeding and nutritional outcomes, and improved growth. Therefore, given what is known about the conclusive benefits of HM diets in other populations (e.g., low birth weight and surgical infants) and the fact that this review identified some similar benefits for infants with CHD, we recommend that clinicians prioritize programs to improve HM feeding in infants with CHD.
High-quality multisite research on HM for infants with CHD is warranted, provided institutions have the appropriate resources and documentation. Larger studies with careful nutrition documentation and robust measures would allow for appropriate statistical power to provide more conclusive outcome data than those currently available.
Footnotes
Acknowledgment
The authors wish to acknowledge Liz Weinfurter, MLIS, Associate Librarian, Health Sciences Library, University of Minnesota, for her assistance with the search.
Authors' Contributions
The authors affirm that they have each met the criteria for authorship as defined by the International Committee of Medical Journal Editors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.