
Abstract
Background:
Human milk is the optimal form of infant nutrition. If mother's own milk is unavailable, families may seek alternative sources of human milk through milk sharing, despite potential health and safety risks with this practice.
Objective:
The purpose of this scoping review was to synthesize the current literature on human milk sharing in the United States to help health care professionals better understand how families may use this practice for infant nutrition.
Methods:
A systematic search was conducted in June 2021 using Ovid MEDLINE, Embase, CINAHL, ProQuest Central, Web of Science, and Google Scholar. Articles were included if the primary outcome was milk sharing, excluding milk banks and preterm hospitalized infants. Results were limited to studies conducted in the United States and published in English after January 1, 2000.
Results:
From 2,124 articles, 34 met inclusion criteria and were reviewed. Study designs were largely observational (30/34), and participants were predominantly white, married, and middle-income women experiencing lactation problems or in possession of excess breast milk. Milk sharing, not for profit, was often facilitated through the internet but exchanged in person. Conversely, for-profit milk sharing often involved shipping and studies found evidence of milk contamination. No studies documented infant harm.
Conclusions:
There is limited research on the milk quality and relative risks of milk sharing, and no research on clinical outcomes in infants fed shared milk. Clinicians have opportunities to engage in open conversations about this practice to guide risk mitigation, however, research on recipient infant outcomes are urgently needed to inform best practices.
Introduction
It is well known that human milk is the optimal form of infant nutrition. 1 Both the benefits of breastfeeding and the risks of formula are well established. 2 Human milk confers innumerable nutritional and immunological benefits to the infant, including both short- and long-term medical and neurodevelopmental advantages. 3 These advantages include protection against infection; improved cognitive development; and reduced risk of cardiovascular disease, obesity, and diabetes.1,3 Moreover, formula has been associated with increased risk of infections, allergies, diabetes, inflammatory bowel disease, and obesity. 2 Thus, human milk is considered the gold standard for infant feeding and the American Academy of Pediatrics (AAP) recommends exclusive breastfeeding for the first 6 months of an infant's life.1,3 However, mother's own milk or pasteurized donor milk from a milk bank may not always be available.
Recently, internet-based milk sharing networks popularized as a community-based social intervention to increase access to human milk.4,5 The availability of internet-based milk sharing networks provides opportunities to increase the number of infants fed human milk. Yet, limited data are available regarding the health and safety of these practices. Furthermore, there is a lack of consensus among public health and professional organizations, which negatively affects the ability of health care professionals to provide guidance for informed infant feeding decisions. 5 To address these gaps in knowledge, a scoping review was conducted to identify the types of available evidence on milk sharing and clarify key concepts in the literature. The primary purpose was to help health care professionals better understand the scope of milk sharing and the rationale used by families to engage in this practice. This article will add to existing literature on milk sharing by providing a framework of what is known and what types of research are needed to inform health care professionals and public health policy.
Methods
Search strategy
We conducted a systematic search in June 2021 to locate both published and unpublished research, including peer-reviewed journal articles, conference abstracts, research and committee reports, government reports, and policy documents. Due to the informal nature of milk sharing and the emerging evidence in this field, the researchers determined a scoping review would best fit this review. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist was utilized to guide this process. 6
An initial search of PubMed was undertaken to identify articles on the topic. The text words contained in the titles and abstracts of relevant articles, and the index terms used to describe the articles were used to develop a full search strategy. Searches determined keyword and index term relevance and were adapted for each information source. The search terms included informal or peer-to-peer milk sharing, or internet purchasing of human milk, using database-specific thesaurus terms (e.g., MeSH terms) as well as keyword terms.
The databases searched included Ovid MEDLINE, Embase, CINAHL, and ProQuest Central. Additionally, using secondary keyword searches, Web of Science was used to identify potential literature published outside of traditional academic publishing, for example, theses and conference abstracts. Finally, the reference list of all included sources of evidence were screened for additional studies. This scoping review was registered to OSF Registries (Registration DOI: 10.17605/OSF.IO/VXMJP) and the full search strategy is available at https://osf.io/vxmjp
Inclusion criteria
Studies included qualitative, quantitative, descriptive, and mixed methods designs. We also incorporated conference abstracts, research and committee reports, government reports, and policy documents. Studies were included if the primary outcome was related to milk sharing, defined as the exchange of expressed milk for the purpose of maintaining an exclusive human milk diet for the term healthy infant. Expressed milk was fresh or frozen and not subject to regulation or routine pasteurization according to accepted standards. For the purposes of this review, not-for-profit milk sharing was defined as the commerce-free exchange of expressed milk and for-profit milk sharing refers to the compensated exchange of expressed milk. Internet-based milk sharing refers to the use of online networks to facilitate the exchange of expressed milk; these networks may include not-for-profit and for-profit milk sharing exchanges.
Exclusion criteria
Studies were excluded if they solely reported on milk banking, or preterm and critically ill infants. We excluded preterm and critically ill infants because the risks to these infants are greater and should be discussed separately. Results were further limited to studies conducted in the United States and published in English after January 1, 2000. Studies published before this were excluded as the practice of internet-based milk sharing did not exist until approximately 2010. 7 Furthermore, given varying opinions on the degree of risk associated with human milk sharing around the world, studies conducted outside of the United States were excluded. Results were limited to exclude reviews, commentaries, and periodicals, as they are not primary research.
Study selection
Following the formal search in June 2021, all identified citations were collated and uploaded into EndNote 20 and duplicates were removed. The review process consisted of two levels of screening, a title and abstract review and a full-text review, performed with the online software application Rayyan. 8 Two members of the research team (K.C.K. and A.C.A.) independently screened the title and abstract of all retrieved citations against the inclusion criteria. Any articles that were deemed relevant by either or both researchers were included in the full-text review. Next, the two researchers (K.C.K. and A.C.A.) individually assessed the full-text articles to determine eligibility. Reasons for exclusion of sources of evidence at the full-text review stage were recorded. Any discord between the researchers at each stage of the selection process was resolved by a third researcher (L.F.W.) and further disagreements were resolved through discussion until full consensus was obtained.
Data extraction
One researcher (K.C.K.) extracted the data and evaluated the methodological quality and credibility of each included study. Data were extracted using a data extraction tool developed by the researcher (K.C.K.). Extracted data included specific details about the participants, methods, limitations, clinical implications, and key findings relevant to the research question.
Data analysis
This review used the findings of each study and the primary data therein to produce a synthesis of milk sharing practices in the United States. Articles were grouped into not-for-profit and for-profit milk sharing to highlight differences. Data are presented in tabular form and categories were created to organize the results by study design, study population, outcomes measured, and key findings. A narrative summary follows the tabulated results and describes how the results relate to the research question. Potential sources of bias and limitations of each study were identified and discussed as a research team.
Results
We initially identified 2,124 articles, and 631 duplicates were removed. During the initial title and abstract screening process, the number of articles to review decreased to 117. Full-text articles were then retrieved and reviewed for inclusion. After further investigation, 34 articles met the eligibility criteria. An overview of the review process is detailed in Figure 1.
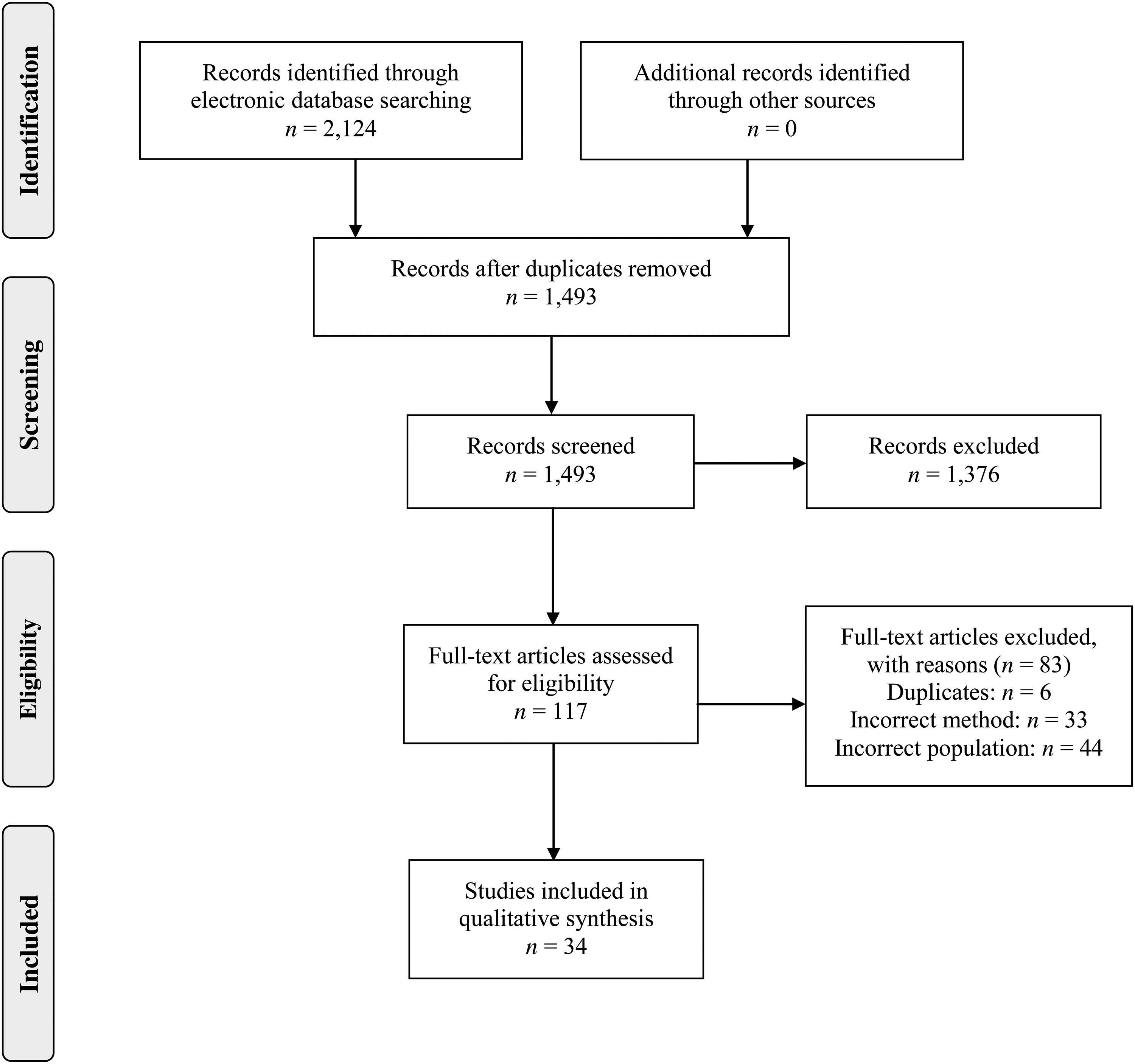
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Articles were excluded for the following reasons: intended recipients were preterm or critically ill; did not use milk sharing or used milk banking; were review articles, commentaries, or periodicals; were not written in English; conducted outside of the United States; and were duplicates. However, two articles were included in this review despite containing participants from outside the United States.9,10 The research team determined that 90% of the study participants were from the United States and the results were pertinent to the current review.9,10 Similarly, a few studies included in this review contained participants that were preterm or critically ill.11,12 Again, the researchers determined that this subset of the study population was marginal in each case, and these studies were important to include in this review.
Included studies were mostly observational, descriptive studies using cross-sectional data (30/34). Study methods also included one nonrandomized controlled trial (1/34), a research report (1/34), and position statements (2/34). Almost half of the studies included were not designed to evaluate a potential relationship between milk sharing and infant health-related outcomes (16/34). Seven studies conducted research on milk quality and no studies measured clinical outcomes or long-term outcomes in infants fed shared milk.
Findings from the included studies underlined key differences between articles related to donor compensation for the exchange of expressed milk. The following sections separate articles into two categories, which are, not-for-profit milk sharing and for-profit milk sharing. Relevant studies are summarized for each section (Tables 1 and 2, respectively).
Not-For-Profit Milk Sharing
IgA, immunoglobulin A.
For-Profit Milk Sharing
HM4HB, Human Milk 4 Human Babies.
Not-for-profit milk sharing
Milk sharing participants were predominantly white, married, middle income, educated, and employed women experiencing lactation problems or in possession of excess breast milk.13–20 Participants were motivated by the known health benefits of human milk and its superiority over formula.10,21 Participants were also driven by the benefit of helping and connecting with families through milk sharing. 16 Additionally, they were motivated by barriers to milk banking; for example, costs, prescriptions, and pasteurization since it destroys beneficial human milk components.21,22
Not-for-profit milk sharing was often facilitated through internet-based milk sharing networks (Human Milk 4 Human Babies, Eats on Feets, and Milk Share), yet the physical exchange of human milk often occurred in person.23,24 Research showed donors reported providing frozen milk as well as fresh milk through local, in-person delivery, and less often shipped frozen milk. 24 Milk was exchanged among family and friends, but also frequently between strangers. 23 Most participants reported following safe milk handling practices, such as hand washing and sanitizing equipment. 25 Few participants reported heat treatment upon receipt of the milk. 26
The most common concerns of women not participating in milk sharing included disease transmission, contamination, exposure to drugs, or dilution with cow's milk.17–19 However, most participants had few or no concerns and did not medically screen donors because they trusted them.12,21,22 In addition to limited donor medical screening, several studies reported minimal involvement of health care professionals in milk sharing.11,22,24,26 Studies also highlighted challenges families faced; for example, logistical stressors and effort to secure milk, fear of running out, institutional barriers, and social stigma.9,10,12 In response, participants avoided physicians, family, and friends who might judge them. 15
No studies have documented infant harm, including two case studies, in which there were also no reports of milk contamination associated with not-for-profit milk sharing.27,28 Furthermore, research has shown that samples of expressed milk under various ambient temperature conditions did not develop a microbial load approaching 104 CFU/mL. 29 Another study found no evidence of differences in macronutrient, antimicrobial protein, and bacteria composition by method of human milk exchange. 30 Moreover, milk sharing has the potential to help infants meet the AAPs breastfeeding goals.13,31 One study reported higher rates of exclusivity and duration of human milk feeding among milk sharing participants than the national average. 13 Similarly, research found more participants using shared milk were feeding their infants human milk at 6 months than nonusers. 31 The potential benefits of not-for-profit milk sharing are evident, although there is a lack of research on the milk quality and relative risks of not-for-profit milk sharing.
For-profit milk sharing
While several internet-based milk sharing networks exist, the for-profit sale of human milk was found on one website (i.e., Only the Breast). 32 This study revealed 5.0% of participants reported for-profit milk sharing solely to make money. 32 Statements about donors' diet, exercise, drug use, milk handling practices, and milk quality were associated with the sale of human milk. 32 These findings support differentiating for-profit milk sharing, where milk was purchased from anonymous donors and shipped to strangers, from not-for-profit milk sharing.
Five studies included in this review were published from research on human milk samples purchased anonymously online.33–37 The investigators excluded milk samples from individuals who inquired additional information about the recipient, to maintain anonymity. The first study found milk samples shipped without ice and milk leaking out of plastic bags upon arrival. 33 Subsequently, these same investigators found evidence of bacterial contamination and bacterial growth was associated with days in transit. 34 The high prevalence of bacterial growth was likely due to improper storage conditions, although the milk samples included in this study were shipped to an off-site mailbox that was only accessible 6 days a week. 34 Next, the researchers discovered bovine DNA in several samples, suggesting cow's milk adulteration. 35 They also reported detectable levels of caffeine and tobacco metabolites in the majority of samples. 37 Nevertheless, they found no evidence of drugs of abuse in the milk samples and no samples were positive for HIV-RNA.34,36
Discussion
Milk sharing participants navigate lactation problems and limited access to breast milk obtained from milk banks to provide infants with an exclusive human milk diet.13,31 Those involved in milk sharing place a high value on human milk and this practice ultimately supports breast milk continuation and exclusivity.13,31 Yet, the Food and Drug Administration and the AAP do not recommend milk sharing.38–40 Whenever human milk is expressed and handled, there is a risk of contamination.28,39 Human milk is a bodily fluid and can carry medications, drugs, and other substances.28,39 Viral, bacterial, and fungal transmission through human milk is also possible, the most concerning of which are HIV, Hepatitis B, and Hepatitis C.28,39 To reduce these risks, the Academy of Breastfeeding Medicine has recommended donor medical screening and safe milk handling practices. 41 In addition, home pasteurization can further reduce the risk of infections, however, it decreases some nutritional and immunological components of human milk as well. 41 Home pasteurization is also complicated and may be difficult to practice in certain settings without access to uniform heating sources.
Milk sharing practices can incorporate a combination of the following: community-based (sharing between friends or relatives) or internet-based (connecting through online networks), not-for-profit or for-profit, and direct in-person exchanges or shipping milk. Thus, the possible health and safety risks may vary based on individual practices. Currently, the potential risks to the infant fed shared milk are inferential and no studies have documented infant harm. It is unknown if internet-based milk sharing, for-profit milk sharing, or shipping milk increase the level of risk associated with this practice, as comparative studies would permit outcome analyses. Moreover, internet-based milk sharing is not synonymous with anonymous exchanges of expressed breast milk. Internet-based milk sharing may be associated with increased risk of exposure to medications or infectious diseases if there is no donor medical screening involved. However, studies also found limited donor medical screening among community-based milk sharing and exchanges with friends and relatives.21,22
Nonetheless, this review identified evidence of potential harm from for-profit milk sharing and especially when shipping is involved. For-profit milk sharing donors face different incentives than not-for-profit milk sharing donors. Consequently, included studies found evidence of milk dilution and contamination with cow's milk associated with for-profit milk sharing. 35 This research also found evidence of bacterial contamination associated with shipping milk. 34 Although these studies involved for-profit milk sharing, not-for-profit milk sharing can also involve shipping milk. Therefore, the potential risk of contamination is also relevant to not-for-profit milk sharing practices that involve shipping milk. Health care professionals have opportunities to understand how families may use milk sharing for infant nutrition to explain potential risks. Understanding that individual practices may vary, clinicians should consider the known benefits of human milk and the possible health and safety risks when facilitating patient-centered discussions with families concerning infant feeding decisions.
Limitations
There are a few limitations of this scoping review; first, this review was limited to milk sharing for the term healthy infant. Although the search strategy and study selection process used in this review were rigorous, the data extraction and analyses were performed solely by one researcher (K.C.K.). Nonetheless, the data extraction was supervised by an experienced research librarian (A.C.A.) and the analyses were discussed with an experienced researcher in breastfeeding medicine (L.F.W.). Lastly, this review was limited by the external validity of the available research on milk sharing. Current studies are largely observational, descriptive studies and prevalence reports. However, the exact prevalence of milk sharing in the United States remains unknown due to a lack of population-level studies. Consequently, the limited generalizability of these studies restricts the ability to fully assess risk mitigation of milk sharing practices.
Conclusions
This review highlights the complexity of milk sharing practices. For-profit milk sharing in the included studies involved shipping frozen milk, which was frequently contaminated upon arrival. 34 Conversely, not-for-profit milk sharing was often facilitated through internet-based networks but exchanged in person, which may decrease the time milk is exposed to improper storage conditions.23,24 Without further studies, for-profit and not-for-profit milk sharing remains an important distinction, as the former may involve dilution with cow's milk. An arguably equally important distinction for the clinician is whether the milk is exchanged in person or shipped, since there is evidence of potential harm of bacterial contamination with shipping milk. Furthermore, anonymous milk sharing may preclude the ability to screen donors for infections or medications.
Health care professionals have an opportunity to affirm milk sharing relationships and engage in shared decision making to counsel families about risk mitigation strategies such as donor medical screening and safe milk handling practices. Unfortunately, there is limited research on milk quality and the potential risks of this practice by examining milk samples, and no research on infant health outcomes. Consequently, the lack of clinical research may inadequately quantify the health and safety of this practice. Additional research is imperative to inform public health policy, but recruitment will require overcoming the secrecy and nondisclosure to health care professionals. Future collaborations with organizations that promote milk sharing may be beneficial.
Footnotes
Acknowledgment
The authors thank Rosie Frasso, PhD, MSc, MSc, CPH, Jefferson College of Population Health, for her support with study conception.
Authors' Contributions
K.C.K., L.F.W., and A.C.A. contributed to study conception, study design, data collection, and data interpretation. K.C.K. had primary responsibility for writing the article. All authors reviewed, edited, read, and approved the article.
Disclosure Statement
L.F.W. serves as the Associate Editor of Breastfeeding Medicine. K.C.K. and A.C.A. have no conflicts of interest to report.
Funding Information
No funding was received for this article.