
Abstract
Background:
Early in the COVID-19 pandemic, many birth hospitals separated SARS-CoV-2-positive mothers from their newborn infants and advised against breastfeeding to decrease postnatal SARS-CoV-2 transmission. Information on how these practices impacted breastfeeding postdischarge is limited.
Objectives:
In a statewide sample of SARS-CoV-2-positive mothers, we aimed to determine the extent to which (1) mother–infant separation and (2) a lack of breastfeeding initiation in-hospital were associated with breast milk feeding postdischarge.
Design/Methods:
From 11 birthing hospitals in Massachusetts, we identified 187 women who tested positive for SARS-CoV-2 from 14 days before to 72 hours after delivery (March 1–July 31, 2020) and their newborn infants. We abstracted chart data from the delivery hospitalization on main exposure variables (mother–infant separation, in-hospital breast milk feeding [expressed milk feeding and/or direct breastfeeding]) and from outpatient visits until 30 days postdischarge. We evaluated associations of in-hospital practices with outcomes up to 30 days postdischarge, adjusting for confounders using multivariable logistic and linear regression.
Results:
Mother–infant separation in-hospital was associated with a shorter duration of any breast milk feeding (regression coefficient estimate
Conclusions:
Perinatal hospital care practices implemented early in the COVID-19 pandemic, specifically mother–infant separation and prevention of breast milk feeding initiation, were associated with adverse effects on breast milk feeding outcomes assessed up to 1 month postdischarge.
Background
With the onset of the COVID-19 pandemic came a wave of uncertainty in health care delivery and implementation of best care practices, fueled by a lack of knowledge regarding this new virus. Initial studies reported concerns about maternal and neonatal outcomes and the risk of perinatal transmission of SARS-CoV-2. These concerns were influenced by prior experience with high rates of obstetric complications seen during previous coronavirus outbreaks (SARS and MERS) 1 as well as during Ebola and Zika outbreaks. 2 This led to uncertainty regarding best practices for newborn care and feeding during the postpartum hospitalization. With the intention of minimizing risk of viral transmission, early recommendations from the American Academy of Pediatrics 3 were to discontinue existing practices known to increase breastfeeding initiation4–8 and continuation, such as skin-to-skin care in the delivery room, rooming in, and in-hospital direct breastfeeding by mothers with known SARS-CoV-2 infection.
Many hospital policies shifted in accordance 9 with these recommendations. Subsequently, evolving evidence demonstrated little to no risk of SARS-CoV-2 transmission through breastfeeding10–13 and guidelines evolved to re-emphasize the importance of physical contact between mother and infant and the establishment of breastfeeding in the immediate postpartum period.
Although many studies4–8 conducted before the COVID-19 pandemic strongly support the positive influence of hospital practices on breastfeeding outcomes, little is known about how mother–infant separation and a lack of in-hospital breastfeeding initiation, early in the COVID-19 pandemic, influenced breastfeeding outcomes. The COVID Mothers' Study 14 utilized an anonymous survey to gather information on SARS-CoV-2-positive mother–infant dyads worldwide and found that infants who did not directly breastfeed, experience skin-to-skin care, or room-in within arms' reach, were significantly less likely to be exclusively breastfed in the first 3 months.
This gap in knowledge has implications not just for the current pandemic, but also for other infectious disease and health crises that may arise in the future. In this study, we aimed to investigate associations of specific hospital practices with respect to breastfeeding outcomes among SARS-CoV-2-positive mother–infant dyads, utilizing chart review methods. We hypothesized that mother–infant separation and a lack of direct breastfeeding during the delivery hospitalization would lead to lower rates of breastfeeding postdischarge and an overall reduction in the duration of breastfeeding postdischarge.
Methods
Study design, study sites, and population
This study leveraged data collected by the American Academy of Pediatrics as a prospective longitudinal cohort study from 11 Massachusetts birth hospitals that serve an ethnically, culturally, and socially diverse population, capturing 52% of the annual births within the state. 15 As described previously 16 we used local COVID-19 surveillance and infection control systems to identify all infants born to mothers who had a positive nasopharyngeal polymerase chain reaction test for SARS-CoV-2 from 14 days before to 72 hours after delivery (n = 255), a criteria developed by the American Academy of Pediatrics National Registry for the Surveillance and Epidemiology of Perinatal SARS-CoV-2 Infection. 17
For the present analysis, we included 187 mother–infant dyads delivered and discharged between March 1 and July 31, 2020 who had outpatient follow-up encounters documented in the electronic medical record (EMR) within 30 days postinfant discharge, containing information about postdischarge breast milk feeding, however, the number of encounters and oldest infant age at last follow-up varied by dyad within the 30-day window. The study was approved by the Institutional Review Board of each individual participating hospital.
Data collection and management
All data were abstracted by hospital-based teams' EMRs using a standardized case report form developed by the National Registry for the Surveillance and Epidemiology of Perinatal SARS-CoV-2 Infection. 17 This form was expanded by our research team to include information from the outpatient encounters. Data were entered into a central REDCap®18,19 database, which served as our electronic data capture system.
Exposures: in-hospital separation and breast milk feeding
Our three exposure variables during the postpartum period and infants' hospitalization were (1) mother–infant separation; (2) direct breast milk feeding in-hospital; and (3) any breast milk feeding in hospital. Regarding separation, we collected data on infant location (mother's room, neonatal intensive care unit [NICU], and/or nursery), and rooming in (any or none). Dyads with infants in the NICU, infants in the nursery, or with indication of “none” for rooming in were categorized as “any separation” and dyads who had both any rooming in recorded and “mother's room” for infant location were categorized as “no separation.” Regarding breastfeeding, we collected data on both expressed milk feeding and direct breastfeeding.
We categorized women with direct breastfeeding or expressed milk feeding as “any breast milk feeding” and those with no direct breastfeeding and no expressed milk feeding as “no breast milk feeding.” Those mothers with infants who were fed with pasteurized donor human milk were included in the “no breast milk feeding” category as this study measured only maternal milk feeding. A third, nonmutually exclusive category included women with any documented direct breastfeeding. The comparison group for “direct breastfeeding” was “no direct breastfeeding.”
Outcomes: postdischarge feeding
We reviewed all available EMR notes from obstetric and pediatric encounters in the 30 days following hospital discharge and recorded whether there was documentation of any breast milk feeding postdischarge, including mention of direct breastfeeding and/or expressed milk feeding. We also recorded day of life of last breast milk feeding documented in the EMR, from which we derived a variable to indicate breast milk feeding duration through 30 days postdischarge.
Covariates
We collected EMR data on maternal characteristics (age, race/ethnicity, primary language, occupation, and zip code of primary residence), severity of maternal COVID-19 illness (symptomatic or asymptomatic), pregnancy and delivery characteristics (gravidity, route of delivery), and infant characteristics (gestational age, birth weight, infant sex, newborn SARS-CoV-2 test result, duration of neonatal hospitalization, infant age at last follow-up). We used the mother's zip code to calculate the social vulnerability index (SVI), a measure developed by the Centers for Disease Control and Prevention that uses 15 U.S. census variables to identify socially vulnerable populations, 20 as we reported previously.16*
Statistical analysis
Beginning with a bivariate analysis, we compared the median duration of breast milk feeding across exposure groups using the Mann–Whitney U test, and compared report of any breast milk feeding postdischarge, and direct breastfeeding postdischarge across exposure groups using Chi squared tests for independence (χ 2 tests). We also used χ 2 tests to evaluate the association between the exposure variables (hospital practices). We tabulated the unadjusted associations between all mentioned covariates and the outcomes and exposures, and then ran t-tests (for continuous covariates with categorical outcomes and exposures), χ 2 tests (for categorical covariates with categorical outcomes and exposures), and Spearman correlation tests (for all covariates with continuous outcomes and exposures). We used a priori hypotheses, associations observed in unadjusted analyses, and results of the above tests to determine which covariates to adjust for in our multivariate analysis.
We hypothesized that the following variables would affect successful breastfeeding initiation and duration postdischarge: gestational age, maternal illness severity, delivery route, duration of infant hospitalization, and infant age at last follow-up. The statistical tests supported our hypothesis as they found significant associations between these covariates and either the outcome or exposure variables. We originally hypothesized that SVI may confound our analysis, but because adjusting for this did not substantially change beta estimates (<10% change), we did not include it in the final model. We adjusted for the appropriate covariates in our multivariable logistic and linear regression models. Logistic regression models were run over a binomial distribution and reported adjusted odds ratios (AORs) with 95% confidence intervals (CIs). Linear regression models were run over a normal distribution and reported regression coefficient estimate (beta estimates) with 95% CI.
All regression models were run using a complete case approach in which observations were dropped due to missing data. We also repeated the same regression analysis stratified by NICU admission status. Additional survival analysis models were run to assess the relationship between the three in-hospital practices of interest and duration of breastfeeding postdischarge, which included Kaplan–Meier Analysis to compare median durations of breast milk feeding across exposure groups, and log-rank tests were used to assess for significant differences between medians. We used R (R version 4.0.4 [2021-02-15]) for all analyses. Two-sided p < 0.05 was considered statistically significant.
Results
Characteristics of the study sample (n = 187), including covariates, exposure variables, and outcome variables are described in Table 1. Unadjusted analysis of in-hospital exposures and postdischarge breast milk feeding outcomes showed significant associations between all in-hospital exposures and all postdischarge breast milk feeding outcomes (Supplementary Table S1). We also found significant associations between in-hospital practices: any hospital breast milk feeding and separation (p < 0.001) and direct in-hospital breastfeeding and separation (p < 0.001) (Supplementary Table S2).
Characteristics of 187 Mother–Infant Dyads with Maternal Peripartum Positive SARS-CoV-2 Testing Who Delivered Between March 1, 2020 to July 31, 2020 in Massachusetts and Had Any Follow-Up Encounters
Variable n < 187 indicates missing data.
Percentages for “All Participants” are calculated as n divided by variable n.
Percentages for exposure groups are calculated as n divided by total n for given exposure group, even if we are missing data for the covariate.
Social vulnerability index uses 15 US census variables derived from zip codes and was derived by the Centers of Disease Control and Prevention; higher numbers indicate greater vulnerability.
NICU, neonatal intensive care unit; SD, standard deviation.
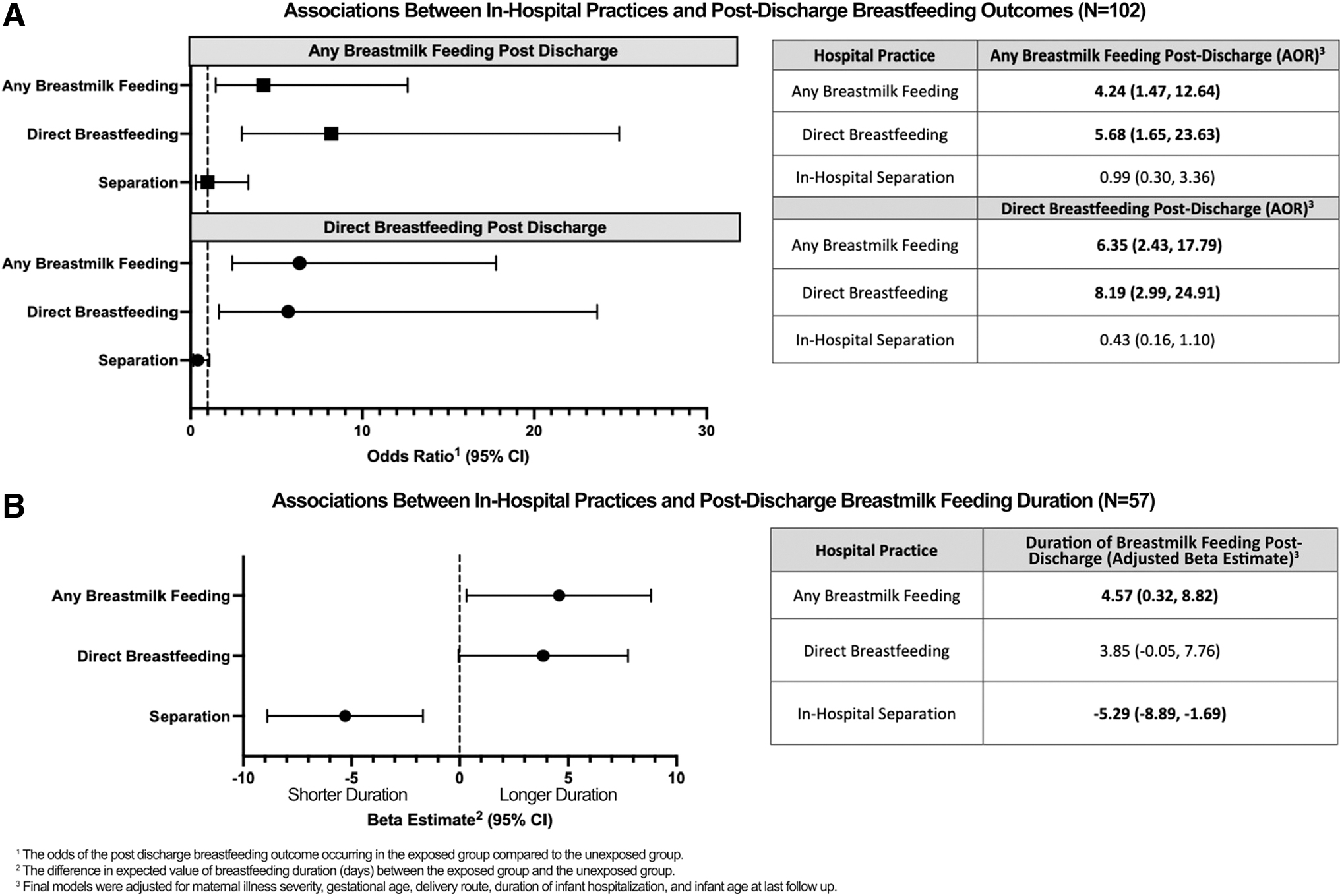
The adjusted results of the logistic and linear regression analysis are reported in Figure 1 and Supplementary Table S3, and summarized below. Analyses stratified by NICU or non-NICU status yielded results that were generally consistent, although precision of estimates was limited by sample size (Supplementary Table S5).
Any in-hospital breast milk feeding
Among mothers who provided any breast milk in-hospital, the adjusted odds of practicing any breast milk feeding was 4.24 times higher (95% CI: 1.47–12.64) and adjusted odds of practicing direct breastfeeding was 6.35 times higher (95% CI: 2.43–17.79) in the 1-month postdischarge period compared with mothers who did not provide any breast milk in-hospital (Fig. 1A). Breast milk feeding duration in the 1-month postpartum follow-up period was also significantly longer by 4.57 days on average (95% CI: 0.32–8.82) for mothers who provided any breast milk in-hospital compared with mothers who did not (Fig. 1B). The Kaplan–Meier analysis also yielded a significant relationship (p < 0.01) between any in-hospital breast milk feeding and duration of breast milk feeding postdischarge (Supplementary Table S4).
Direct in-hospital breastfeeding
Among mothers who practiced direct breastfeeding in-hospital, the adjusted odds of practicing any breast milk feeding was 5.68 times higher (95% CI: 1.65–23.63) and adjusted odds of practicing direct breastfeeding was 8.19 times higher (95% CI: 2.99–24.91) in the 1-month postdischarge period compared with mothers who did not practice direct breastfeeding in-hospital (Fig. 1A). While not statistically significant, there was a trend toward longer breastfeeding duration by 3.85 days on average (95% CI: −0.053 to 7.76) within 30 days after hospital discharge for mother–infant dyads who had direct breastfeeding experience in the hospital compared with those who did not (Fig. 1B).
In-hospital separation
In adjusted models, we found that among mother–infant dyads who were fully separated during the birth hospitalization, breastfeeding duration after hospital discharge was, on average, 5.29 days (95% CI: −8.89 to −1.69) shorter compared with mother–infant dyads with no in-hospital separation. In-hospital separation was not significantly associated with the odds of any breast milk feeding (AOR 0.99 [0.30, 3.36]) or direct breastfeeding (AOR 0.43 [0.16, 1.10]) during the 30-day postdischarge period.
Discussion
The impact of the COVID-19 pandemic on health care delivery was particularly marked in the perinatal setting where many beneficial best practices were initially disrupted and replaced with isolation practices such as maternal and infant separation and avoidance of breast milk feedings, due to lack of evidence and guidance. Due to the well-documented beneficial effects of breastfeeding on both mothers and infants,4–8 it is critical to examine the lasting impact these early COVID-19 practices had on maternal breastfeeding behaviors.
In this study, we found that maternal and infant separation generally had a negative impact on the rates and duration of breastfeeding postdischarge, however, separation was not associated with significant reductions in any breastfeeding postdischarge, this finding may speak to there being more power to detect an association with a continuous outcome rather than a categorical one. Additionally, direct breastfeeding in the hospital increased the odds of any breast milk feeding and direct breastfeeding postdischarge. Lastly, any breast milk feeding in the hospital had positive associations with breastfeeding behavior, including both direct and any breast milk feeding postdischarge and increased duration of breastfeeding postdischarge.
Overall, our results support and extend the existing literature on the importance of physical closeness between mother and infant for initiating and maintaining breastfeeding.21–24 Additionally, our findings add to accumulating evidence regarding the harms of early COVID-19-driven perinatal hospital practices on breastfeeding-related outcomes, as well as on maternal and infant well-being more generally. Bartick et al. 14 found a significant decrease in likelihood of exclusive breastfeeding in the first 3 months among infants who did not directly breastfeed, experience skin-to-skin care, or who did not room-in within arms' reach. Similarly, Zanardo et al. 25 in their study of a cohort in Northeastern Italy, found that those who gave birth during the COVID-19 pandemic presented significantly lower exclusive breastfeeding rates than those who gave birth the previous year, likely due to increased formula feeding practices during COVID-19.
Salvatore et al. 26 examined the risks and benefits of breastfeeding for SARS-CoV-2-positive mother–infant dyads and found that with appropriate precautions (such as the use of closed incubators, distanced rooming in, hand hygiene, use of surgical masks, breast cleansing), perinatal transmission of COVID-19 is unlikely to occur, even during direct breastfeeding. The results of this study along with our findings regarding the harms of mother–infant separation and lack of in-hospital breastfeeding illustrate the importance of identifying and implementing alternative safety procedures for SARS-CoV-2-positive mother–infant dyads that do not include total separation.
Our study taken together with previous studies suggests that COVID-19 hospital practices, notably mother–infant separation, had a detrimental effect on postdischarge breastfeeding initiation, establishment, and duration. Additionally, while our study did not examine the effects of COVID-19 hospital practices on maternal mental health, previous studies14,25 have found that these practices, notably mother–infant separation, resulted in increased feelings of distress and postpartum depression related to inability to breastfeed after separation. Considering these detrimental effects on maternal mental health in the context of existing literature,27,28 which emphasizes the importance of mothers retaining a sense of personal achievement and control through active decision making during childbirth, we are reminded of the importance of prioritizing patient autonomy, and a shared decision-making model especially in times of uncertain risks.
The existing literature today, including our study, provides evidence for the continuation of established evidence-based best practices in the perinatal setting during the COVID-19 pandemic, and highlights the importance of flexibility in the creation of protective strategies in times of crisis and future pandemics. Rooming-in and breastfeeding under a standardized protocol minimized postnatal transmission of SARS-CoV-2 from infected mothers to their neonates during the height of the COVID-19 pandemic. 29
Current literature does not only provide evidence of an extremely low risk of mother–infant transmission of SARS-CoV-2 through breastfeeding and breast milk provision, 30 but also suggests a potential protective effect against infant infection through SARS-CoV-2-specific IgA and IgG antibodies found in breast milk of both women infected with COVID-1930–32 and women vaccinated against COVID-19.33,34 The direct immune protective effects of breast milk are also supported by the finding of significantly increased SARS-CoV-2 spike protein-specific salivary IgA antibodies in infants fed breast milk versus infants fed an exclusive formula diet (p = 0.01). 35 Taken together, the above evidence and our results support the continuation of breast milk feeding during COVID-19 surges in the perinatal setting.
A major strength of this study was the size and diversity of the study population. We included 11 academic and community hospitals, representing more than 50% of all births in the state of Massachusetts. Racial and ethnic diversity of the study population was proportional to the population of pregnant women in the United States (U.S.) with SARS-CoV-2 infection as reported by the Centers for Disease Control and Prevention. 36 This suggests generalizability to other U.S. perinatal populations.
Although some maternity practices related to infant feeding may not have changed at the start of the pandemic, our collective clinical experience indicates that practices such as strict mother–infant separation were previously extremely rare. While there are hospitals who do not practice the 10 steps, we do know from 2020 survey data 37 that adherence to 10 steps, particularly in Massachusetts, is relatively high. We are limited by the lack of data on the reason or reasons for mother–infant separation. We also do not have information regarding the reason for NICU admission, including whether infants were admitted to the NICU to facilitate separation from the mother and/or for medical or administrative indications.
It is possible that underlying reasons for NICU admission, specifically infant illness, directly contributed to the observed differences in breastfeeding outcomes. There may also be other relevant covariates that were excluded from the analysis due to data availability and data collection methods. Additionally, there was variability within the follow-up period as per mother–infant dyad. While the follow-up period did span over 30 days providing insightful information regarding postdischarge breastfeeding reports, some mothers only had one encounter early in the follow-up period and therefore their reported durations may not capture the true duration of their breastfeeding. The follow-up period was constrained to 30 days by available data in the EMR, which may not accurately represent future breastfeeding experiences, although there is evidence to suggest that the first 4 weeks of breastfeeding are a significant predictor of breastfeeding at 6 and 12 months of age. 38
Lastly, this analysis was intended to capture differences on the dyad level and not serve as a hospital policy analysis. Therefore, the analysis focused on the entire dataset without including detailed information on each hospital policy, although we do recognize that hospital policies changed throughout the course of the pandemic. 39
Conclusion
We conclude that perinatal hospital care practices implemented at the start of the COVID-19 pandemic, including mother–infant separation and the prevention of direct breastfeeding in the hospital, were associated with substantially poorer postdischarge breastfeeding outcomes. These findings reaffirm the importance of physical contact between mother and infant and the early initiation of direct breastfeeding for longer-term breastfeeding success. In times of crises such as the recent global COVID-19 pandemic, we are reminded of the influential role health care providers and institutions have as leaders in the communities they serve. We hope that the findings from our study will help provide context and guidance if similar crises arise in the future and ultimately aid in the identification of clear policy recommendations and best practices.
Footnotes
Acknowledgment
The authors wish to thank all the participating teams and state stakeholders.
Authors' Contributions
M.B.B. and L.R. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: L.R. and M.B.B. Acquisition, analysis, or interpretation of data: L.R., M.B.B., and P.R.M. Drafting of the article: L.R. Critical revision of the article for important intellectual content: all authors. Statistical analysis: L.R. and P.R.M. Obtained funding: M.G.P. Supervision: M.B.B.
Disclosure Statement
No competing financial interests exist.
Funding Information
This was supported in part by W.K. Kellogg Foundation (PI M.G.P.; P0131665). The funder/sponsor did not participate in this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.