
Abstract
Objectives:
The study was intended to verify the association between the gestational age of newborns classified as term and the success of breastfeeding in babies born by elective cesarean section. Also, to analyze how the variability of gestational age within the term influences breastfeeding.
Materials and Methods:
Retrospective study of a cohort, which included full-term newborns and their mothers, whose deliveries occurred by elective cesarean section. Among the inclusion criteria are delivery due to elective cesarean section and minimum gestational age of 37 weeks. The database consisted of medical birth information and interviews with mothers.
Results:
This study included 954 full-term newborns born by elective cesarean section. Exclusive breastfeeding at 3 months and being breastfed at 6 months showed a statistically significant association in the correlation with the variability of gestational age. There was a statistically significant association between exclusive breastfeeding at 3 months and breastfeeding at 6 months in the correlation between early term and full term. The trend test showed a significant progressive in the breastfeeding curve versus gestational age.
Conclusion:
Full-term newborns show better results of exclusive breastfeeding at 3 months and continued breastfeeding at 6 months, compared with those born at early term. Gestational age, even in term, has an influence on the success of breastfeeding in newborns undergoing elective cesarean delivery.
Introduction
Breast milk is the best source of nutrition for children and provides benefits that extend over the entire development process.1–3 Studies indicate that breastfeeding protects against infant mortality and can be used as a preventive measure against infant morbidity.4,5 Recent meta-analyses have shown that children who are breastfed have higher performance in intelligence tests and are less likely to be overweight or develop diabetes.1,5,6
Breastfeeding has multifactorial determinants. 7 Studies addressing the influence of mode of delivery on breastfeeding and duration of exclusive breastfeeding have produced conflicting results.8–10 Particularly in elective cesarean sections, not preceded by labor, delayed onset of lactation may increase the chances of offering infant formula by interpreting this delay as a need for another feeding source, comfort, or risk of dehydration. 11
In recent years, studies have shown differences between term infants. The literature has increasingly recognized the vulnerability of early-term infants (born between 37 weeks and 38 weeks 6 days of gestation).12,13 Fetal maturity occurs along a spectrum, and thus is not attained at a distinct point in time.14,15 Early-term infants may be more likely to have breastfeeding difficulties because of inadequate maternal lactation or unrecognized immaturity.16–18
The aim of this study was to determine the influence of gestational age on breastfeeding outcomes in term infants delivered by elective cesarean section.
Methods
This was a retrospective cohort study, based on a quantitative analysis, of term infants and their mothers undergoing elective cesarean delivery at Moinhos de Vento Hospital in Porto Alegre, southern Brazil. The study site is a private hospital with high rates of cesarean delivery.
The study covered the deliveries occurring from October 2011 to April 2013. Inclusion criteria were elective cesarean delivery (i.e., previously scheduled for any reason), minimum gestational age of 37 weeks, mother without previous breast surgery (breast implant or breast reduction), HIV-seronegative mother, newborn infant without congenital malformations, 5-minute Apgar score >6, and no need for oxygen supplementation or admission to the neonatal intensive care unit (NICU).
The database consisted of initial data obtained from the newborns' medical records and from interviews with mothers in the recovery room after delivery. Follow-up data were obtained by telephone contact with mothers at the end of 2 weeks, 3 months, and 6 months after childbirth. Infant weight at 10 days, 3 months, and 6 months was reported by the mothers by telephone. The records of contacts with postdischarge mothers were performed by maternity nurses trained to assess the condition of breastfeeding. We used a standard questionnaire to all mothers contacted in the study.
The study variables were as follows: maternal age; maternal occupation; gestational age recorded in completed weeks; infant sex; 1- and 5-minute Apgar score; birth weight recorded in grams; weight at 10 days, 3 months, and 6 months of age; have formula in the prescription; formula feeding within 24 hours of birth; formula feeding after 24 hours of birth; and breastfeeding at 3 and at 6 months.
A best estimate of gestational age was recorded, determined according to the following hierarchy: obstetric calculation based on the date of last menstruation or in vitro fertilization; obstetric ultrasound parameters described in the mother's medical record; and evaluation of the newborn physical examination.
The outcomes assessed were exclusive breastfeeding at 3 months and at 6 months, and breastfeeding at 6 months.
For this study, assuming a power of 80% and a ≤ 5% significance level, we calculated that a sample size of 752 participants would be required to estimate a 95% confidence interval (CI) to verify breastfeeding proportions between gestational ages. Sample size was calculated using WinPepi, version 11.36, to study the prevalence of the proportion of exclusively breastfed infants.
The variables are reported as descriptive measures of central tendency and dispersion or as frequencies and proportions, depending on their classification. Intervening variables, such as gestational age and formula feeding, were analyzed by logistic regression to determine whether they interfered with the physician's first prescription of formula. Qualitative variables, such as maternal occupation, formula prescribed at first prescription, and formula feeding, were assessed by a chi-square test of association. The same tests were used to analyze the effect of intervening variables on the possibility of an infant being breastfed. Data were analyzed using SPSS, version 21.0.
The study was approved by the Research Ethics Committee of Pontificia Universidade Catolica do Rio Grande do Sul and by the Research Ethics Committee and Scientific Committee of Moinhos de Vento Hospital Education and Research Institute (approval number: CAAE 81455717.0.0000.5336).
Results
During the study period, 1,109 infants delivered by elective cesarean section were eligible. Of these, 155 were excluded because their mothers had undergone breast implant surgery or breast reduction surgery. A total of 954 term infants delivered by elective cesarean section were included in this study.
Most infants included in the study had a gestational age of 38 − 39 weeks. The characteristics of the study population are shown in Table 1. All mothers in the study received prenatal care. None of the infants required NICU admission. All mothers stayed with their babies in a rooming-in facility.
Maternal and Neonatal Clinical Characteristics
Frequency analysis.
EBF, exclusive breastfeeding; NS, no statistical significance; SD, standard deviation.
The analyses were performed according to gestational ages of term birth. The term infants were then categorized into the following gestational ages for analysis: 37, 38, 39, and 40 weeks. No infant with gestational age >40 weeks was delivered by elective cesarean section during the study period.
Figures 1 and 2 show the results of the assessment of gestational age variation in relation to exclusive breastfeeding at 3 months and nonexclusive breastfeeding at 6 months. An increasing linear trend was observed toward breastfeeding continuation as a function of gestational age, indicating that the higher the gestational age, starting at 37 weeks, the greater the success of breastfeeding.
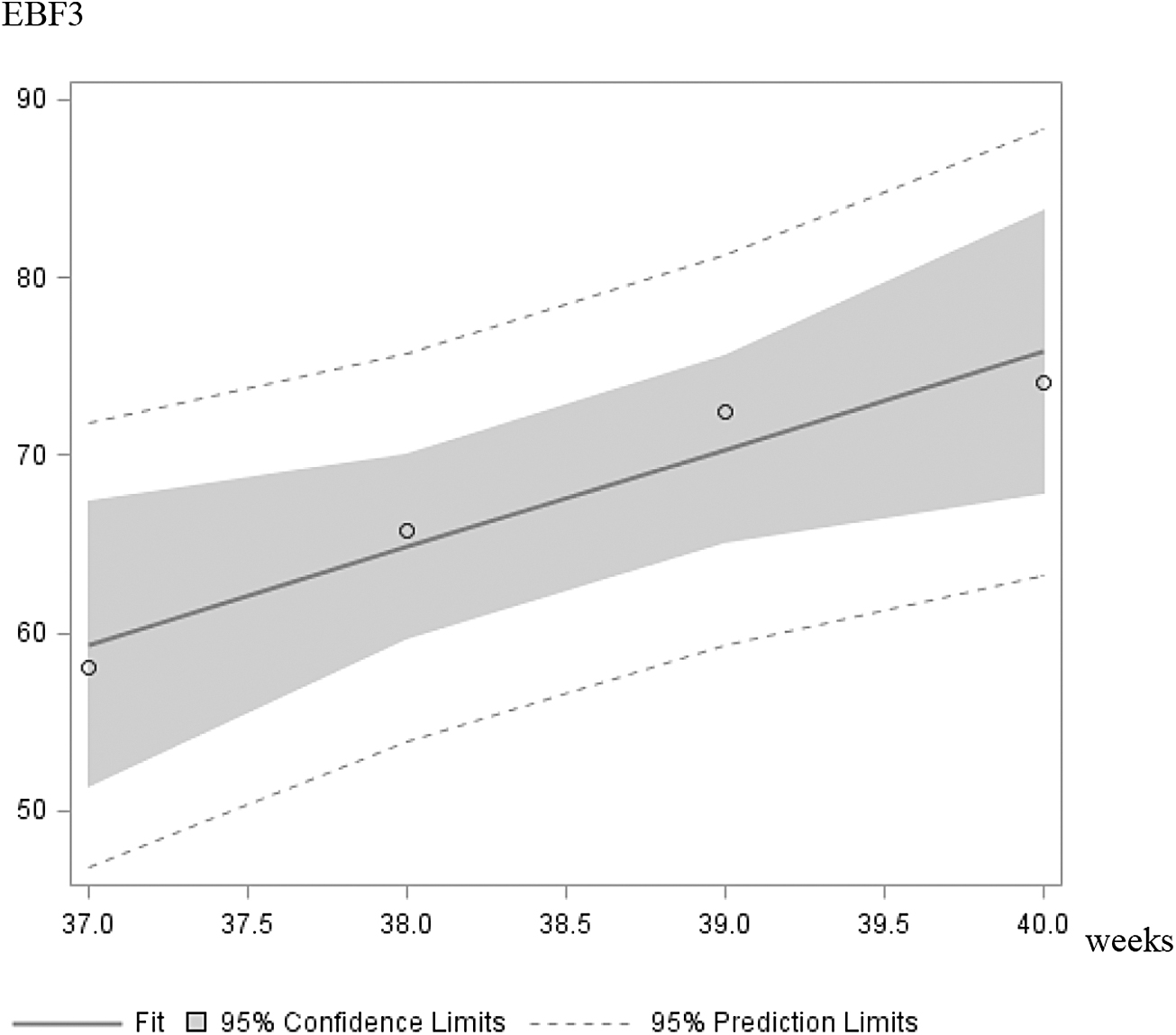
Gestational age and breastfeeding outcomes at 3 months. EBF3, exclusive breastfeeding at 3 months.
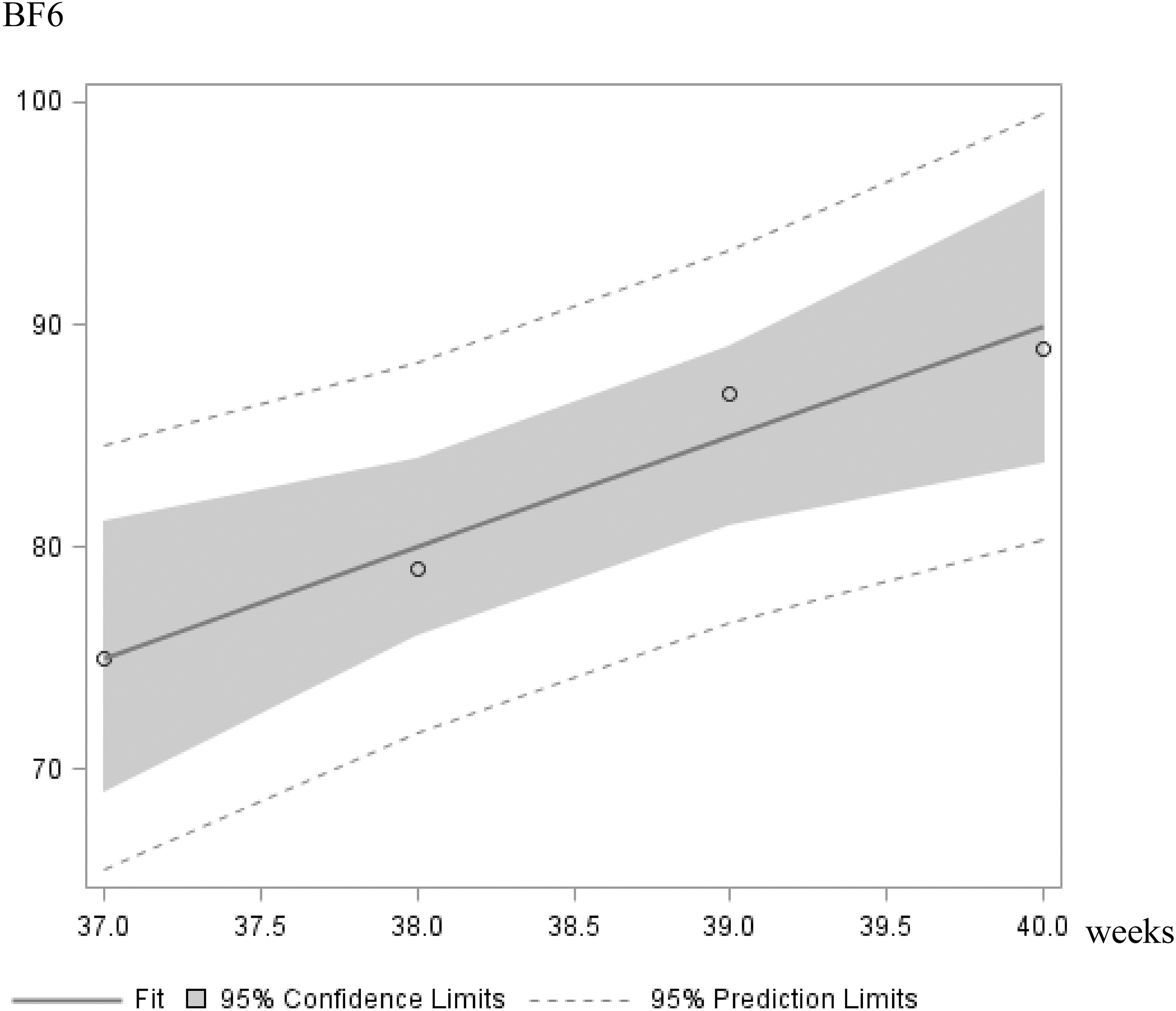
Gestational age and breastfeeding outcomes at 6 months. BF6, breastfeeding at 6 months.
In a parallel analysis, breastfeeding outcomes were assessed with the infants divided into early term (born at 37–38 weeks 6 days) and full term (born at 39–40 weeks 6 days). The results showed a favorable statistical significance for full-term infants regarding exclusive breastfeeding at 3 months (p = 0.008) and nonexclusive breastfeeding at 6 months (p = 0.001) (Table 2).
Early-Term and Full-Term Breastfeeding Outcomes
p < 0.05. Chi-square test. Continuity correction.
EBF, exclusive breastfeeding.
In the multivariable analysis of intervening factors associated with breastfeeding in term infants delivered by elective cesarean section, the presence of formula at first prescription was negatively correlated with a gestational age of 38 weeks. Statistical significance was found in exclusive breastfeeding at 3 months (p = 0.006) and in breastfeeding at 6 months (p = 0.014).
A logistic regression analysis demonstrated that gestational age (p = 0.011; odds ratio: 1.282; 95% CI: 1.058–1.552) and formula at first prescription (p = 0.002; odds ratio: 0.513; 95% CI: 0.333–0.790) were independent risk variables for exclusive breastfeeding outcomes at 3 months. Formula at first prescription was negatively associated with exclusive breastfeeding outcomes at 3 months, regardless of gestational age.
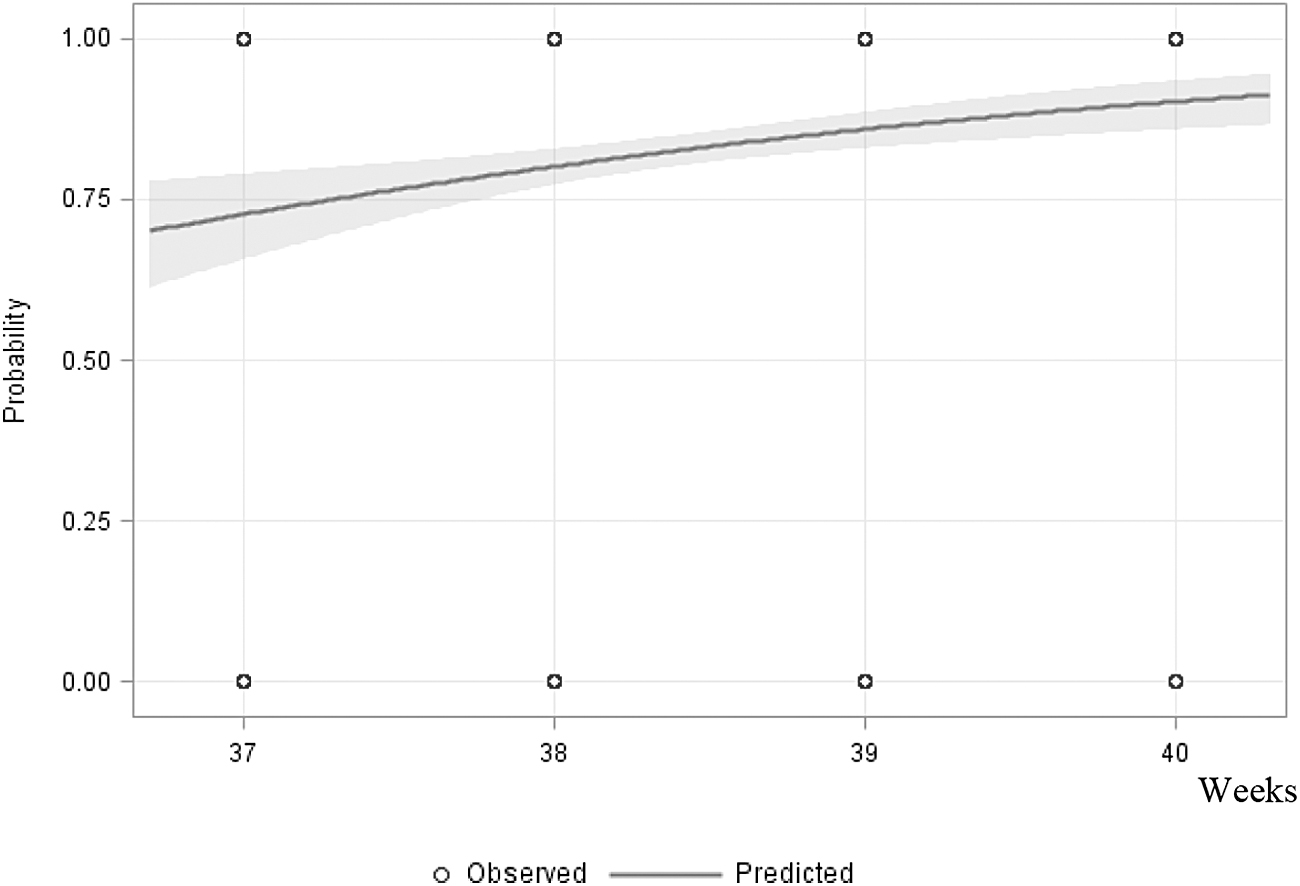
Increasing variations in gestational ages of term birth were positively associated with better breastfeeding outcomes (Table 3). A trend test was performed, with a linear correlation indicating a significant progressive trend of the exclusive breastfeeding curve at 3 months (Fig. 3) and breastfeeding curve at 6 months (Fig. 4) versus gestational age.

Trends for exclusive breastfeeding at 3 months with increasing gestational age. Trend test: p = 0.0029.
Trends for breastfeeding at 6 months with increasing gestational age. Trend test: p
Gestational Age and Breastfeeding Outcomes
Chi-square test.
Statistically significant association by the residuals test adjusted to 5% of significance.
EBF, exclusive breastfeeding.
Figure 3 shows the results of predicted probabilities with gestational age. Each additional week in gestational age, starting at 37 weeks, increased the chance of successful exclusive breastfeeding at 3 months by 2.328 times. A logistic regression model adjusted for the data is important to express the relationship between successful breastfeeding and gestational age by the score test.
In Figure 4, the results indicate that each additional week in gestational age, starting at 37 weeks, increased the chance of successful nonexclusive breastfeeding at 6 months by 2.516 times. A logistic regression model adjusted for the data is important to express the relationship between successful breastfeeding and gestational age, which corresponds to the probability value (p) of the Cochran–Armitage trend test.
Discussion
Historically, all infants born within the wide range of gestational ages considered term birth have been treated equally. The particularities and vulnerabilities of the different gestational ages classified as term have long been ignored. Our results suggest that there are differences between term infants in relation to breastfeeding outcomes. Analytically, our results are relatively consistent in showing a trend toward increased breastfeeding success with each additional week of gestation between 37 and 40 weeks. Early-term infants (born between 37 weeks and 38 weeks 6 days) had worse outcomes in exclusive breastfeeding at 3 months and in nonexclusive breastfeeding at 6 months than full-term infants (born between 39 weeks and 40 weeks 6 days).
For the past 5 years, early-term infants have been seen as distinct from full-term infants, with a greater risk of complications related to the onset and maintenance of lactation.12,18,19 The neurodevelopmental stage of term infants born before 39 weeks of gestation, per se, can be a major impediment to successful breastfeeding. 15 Studies have shown that the immaturity of early-term infants related to effective sucking, swallowing, and breathing, which are critical for successful lactation and nutrition, may be similar to that of late-preterm infants (born at 34–36 weeks 6 days). 20 This condition may place early-term newborn infants at risk for breastfeeding difficulties.
Regarding our results according to gestational age stratified into term birth weeks, there was a positive correlation between gestational age and breastfeeding continuation. Among the term gestational ages, there was a statistically significant association for exclusive breastfeeding at 3 months and breastfeeding at 6 months. The odds of successful breastfeeding increased with each additional week in gestational age, starting at 37 weeks. This trend toward success continued to increase from 39 to 40 weeks. This finding demonstrates a difference in impact on better breastfeeding outcomes with increasing gestational age. This may be particularly relevant when indicating an elective cesarean section before 40 weeks of gestation.
Hackman et al. 16 reported that infants born at 37–38 weeks had greater breastfeeding difficulties than those born at 39–41 weeks. All term gestational ages were positively associated with breastfeeding continuation at 1 month after birth. Mode of delivery was not significantly associated with breastfeeding continuation. The premature discontinuation of breastfeeding of early-term infants was attributed to an increased likelihood of delayed breastfeeding initiation. This study did not assess whether infants had been breastfed within the first hour of life.
In the analysis of our data, the linear correlation pointed to a significant progressive trend of the exclusive breastfeeding curve versus gestational age. Goyal et al. 17 reported that early-term infants were more likely to receive a high level of support for breastfeeding than full-term infants. This difference was attributed to a perception of these infants as being more vulnerable than full-term infants. Another interesting observation was the trend toward a lower likelihood of exclusive breastfeeding for early-term than full-term infants. For the outcome of any breastfeeding, surprisingly, this trend was even more pronounced for early-term than full-term infants, possibly because of shorter length of hospital stay and less support after discharge. 17
Our results did not show a higher prevalence of formula prescription in early-term infants. This suggests that there was no greater intervention of a specific practice that may have acted as a determinant of breastfeeding failure in this group.21–23
Hwang et al. 18 reported similar results. Mothers of early-term and late-preterm infants were less likely to initiate and continue breastfeeding than mothers of full-term infants. There was also an increased risk of morbidity and mortality in this population of infants. Also of note is a study in which, based on the range of behaviors of term infants, early-term infants experienced an increased risk of feeding-related hospital readmission compared with full-term infants. 19 Since infants admitted to the NICU were not included in this study, neither were those infants who required readmission after mother–infant discharge.
Regarding the results of exclusive breastfeeding at 6 months, recommended by the World Health Organization, no statistically significant difference was found between early-term and full-term infants. The decline in exclusive breastfeeding at 6 months to rates <10% was observed in both early-term and full-term infants. This finding may be attributed to mothers' return to work. In our sample, mean maternal age was >30 years and most mothers had a bachelor's degree or higher. The rate of mothers who had returned to work at 3 months was 7.1%, against 76.2% at 6 months. This could explain the discontinuation of exclusive breastfeeding at 6 months in the different gestational ages. Bai et al., 24 in a study of 1,738 mothers, evaluated breastfeeding continuation after return to work and found that only one-third of mothers continued breastfeeding 2 weeks after returning to work. A study conducted in Spain also found a negative correlation between mothers' return to work and duration of exclusive breastfeeding. 25
In relation to the use of formula supplementation, there are several references on the interference of formula feeding with breastfeeding continuation.26–30 Initially, we were under the impression that formula prescription would correlate with the extremes of term birth. We believed that infants born at 37 weeks of gestation would more likely be prescribed and fed formula, because of the proximity to prematurity, which is interpreted by attending physicians as a potential risk condition for hypoglycemia and dehydration. A similar potential risk was expected for infants born at 40 weeks, with birth weight close to the 90th percentile. None of our results can confirm these speculations.
There is growing evidence that infants born at 37–38 weeks of gestation have greater breastfeeding difficulties and other complications, including intellectual and cognitive development, than those born at 39–41 weeks.31–34 This context suggests a relative physiological immaturity that may have important implications at the population level. This study possibly adds to the literature, as already demonstrated by Noble et al., 35 that a greater provision of attention and support for infants born between 37 and 38 weeks may result in better breastfeeding outcomes.
Limitations of this study include the retrospective nature of data collection and the fact that it was conducted in a private hospital, where the prevalence of cesarean deliveries was high. However, the study sample included only infants delivered by elective cesarean section without medical justification for interrupting pregnancy, thus eliminating cause-of-birth biases and allowing evaluations by specific gestational ages. In addition, our study population has a socioeconomic status different from that of most of the Brazilian population. Also, several data, especially those regarding breastfeeding continuation, were obtained by telephone contact. Therefore, it should not be overlooked that some mothers might have omitted the use of formula supplementation on some occasions, which contradicts the statement of exclusive breastfeeding, or might have even denied the interruption of breastfeeding out of embarrassment.
Currently, the hospital where this study was conducted has been promoting initiatives for humanization of labor, with the purpose of reducing the rate of cesarean deliveries. Future analyses of breastfeeding performance and gestational ages should be extended to compare infants delivered vaginally versus by cesarean section.
Conclusions
Gestational age appears to have an impact on the breastfeeding outcomes of term infants delivered by elective cesarean section. Worse outcomes were observed in early-term infants, compared with full-term infants, for continuation of exclusive breastfeeding at 3 months and breastfeeding at 6 months. It is possible to infer a clear trend toward better breastfeeding outcomes with increasing gestational ages of term birth. We speculate that other aspects of maturity within the term period can influence not only breastfeeding.
Footnotes
Authors' Contributions
Conceptualization, formal analysis, writing, review, and editing by M.F.C.S. Idea and concept, formal analysis (lead), review, and editing by H.H.F. Resources by L.U.M. Supervision by D.F.V.V. Review and editing (supporting) by M.G.O.
Disclosure Statement
The authors report no potential conflicts of interest.
Funding Information
This study did not receive any funding.