
Abstract
Objective:
This study aimed to investigate the association between prepregnancy obesity and disruption of exclusive breastfeeding (EBF) within the first month of life.
Materials and Methods:
This was a prospective cohort study conducted among Brazilian mothers and their babies born between February and December 2017. Research was conducted in all maternity hospitals in Vitória da Conquista, Brazil. Data collection started in the maternity hospitals of the city and, subsequently, an interview was conducted during a home visit on the 30th day of the child's life. Survival analysis was performed using Kaplan–Meier curves and a log rank test was applied to compare the curves. The association between independent variables and the response variable was assessed using Cox regression, following the conceptual model created for the study.
Results:
The study analyzed 329 pairs of mothers and babies. The prevalence of prepregnancy obesity was 12%. The prevalence of EBF disruption in the first month of life was 41.1% in nonobese mothers (confidence interval [95% CI]: 35.3–46.9) and 52.6% in obese mothers (95% CI: 36.3–68.4), with a shorter survival time among mothers with prepregnancy obesity (log rank p < 0.05). The risk of EBF disruption in the first month of life was 83% higher among mothers with prepregnancy obesity, after adjusting for confounding variables—demographic, socioeconomic, prenatal maternal data, and childbirth variables (hazard ratio = 1.84; 95% CI: 1.08–3.11).
Conclusions:
We observed an association between pregestational obesity and disruption of EBF in the first month of life. This finding reinforces the need for a thorough professional approach to the practice of breastfeeding in this population in the prenatal period as well as early puerperium.
Introduction
Over the past decades, the prevalence of overweight and obesity has increased, especially in women. According to the World Health Organization (WHO), 40% of adult women were overweight in 2016. 1 In Brazil, the prevalence of obesity in women increased by 71% between 2006 and 2018, and a significant proportion of those women were of childbearing age. 2
Obese women seem to have less exclusive breastfeeding (EBF) for multiple reasons. 3 Excess body fat is involved in hormonal changes that culminate in delayed lactogenesis and reduced production of breast milk. The physiology of lactogenesis can be affected by maternal obesity through insulin resistance, potentially hampering several stages of lactation, such as possibly blunting mammogenesis in early pregnancy, impairing the development of differentiated lactocytes in late pregnancy, delaying the onset of lactogenesis, and impeding the rate of milk production in mature lactation.4,5 Excess adipose tissue is also related to decrease in the prolactin response to breastfeeding. In addition, anatomical and psychological factors linked to obesity are among difficulties related to EBF in this population.4,6
To promote the practice of breastfeeding, the WHO recommended that breastfeeding should be the exclusive method of feeding until the sixth month of life without incorporation of any other type of food, including water. 7 With this policy of breastfeeding protection, the prevalence of EBF at 6 months of life in Brazil increased from 2.9% in the 1980s to 36.6% in 2013,8,9 which, although still considered reasonable according to WHO parameters, 7 is far from ideal. Data on EBF in the first month of life indicate low prevalence with rates of 52–59.3% in Brazil.10,11 In women with prepregnancy excess weight, the scenario is even more worrying with the prevalence of EBF reported to be <30%.12,13
Early identification of factors that compromise the practice of breastfeeding is crucial since early weaning leads to >500,000 child deaths annually, and is responsible for 8% of the global disease burden. 14 Few studies have investigated the relationship between prepregnancy nutritional status and breastfeeding in the first month of life in Brazil.15–19 This topic warrants urgent attention owing to the rapid increase in the prevalence of obesity and low rates of EBF. Therefore, the aim of this study was to investigate the association between prepregnancy obesity and disruption of EBF within the first month of life.
Materials and Methods
Design
This was a prospective cohort study, which is part of a larger project, entitled “Follow-up on breastfeeding practices and complementary feeding in children under one year of age living in the municipality of Vitória da Conquista.” Cohort data collection took place, initially, in all maternity hospitals in the city and thereafter at 30 days, 6 months, 12 months, and 24 months of the children's lives, through home visits. For this study, the data collected in the maternity hospital and at the 30-day visit were analyzed. There were four maternity health care services—one with exclusive care by the public health system (PHS), another with exclusive private care, and two with both types of services. Of the four services, only one was accredited with the Baby Friendly Hospital Initiative. In 2017, the four hospitals performed 5,541 deliveries. 20
Participants
A representative sample of mothers and their babies who were born in any of the four hospitals between February and December 2017, was selected. The inclusion criteria were mothers and newborns living in the urban area of Vitória da Conquista who did not require intensive care unit admission, and delivered at a gestational age of at least 37 weeks. The exclusion criteria were twin pregnancies, maternal human immunodeficiency virus infection, and children with malformations that compromised breastfeeding, such as cleft palate.
Based on Vieira's incidence of EBF of 59.3% at the end of the first month among Brazilian mothers, 11 a relative risk of 1.2, power of 80%, and confidence level of 95%, the required sample size was a minimum of 252. With an additional 30% to account for losses, the minimum sample size included 328 mother–baby pairs. To define the number of pairs required in each institution, the proportion of live births in 2016 at the respective institution was considered along with the proportional number of births in private care and the PHS.
Data collection
The first interview, which constituted the cohort's baseline, was conducted in the maternity wards. The researchers identified births in the preceding 24 hours and checked the participant's eligibility criteria through the medical records. Thereafter, mothers and babies were selected through a random draw to choose three mother–baby pairs per maternity hospital per day, to enable follow-up of participants according to the number of researchers available. If there were only three pairs, or less, who met the inclusion criteria, all were invited. The mothers were included in the study after signing the Informed Consent Form. Subsequently, a questionnaire was administered to obtain sociodemographic and maternal information related to childbirth and postpartum features.
The second interview was conducted 30 days after birth in a home visit scheduled by telephone. Some mothers were visited later than scheduled, depending on the mothers' availability for an interview. In this visit, a new questionnaire was used to collect information about childcare, breastfeeding, introduction of other foods, use of pacifiers and bottles, and the child's health condition.
Both questionnaires were semistructured and were built from the review of research collection instruments already consolidated in Brazil.21–26
Measures
Demographic, socioeconomic, and prenatal maternal data
The demographic, socioeconomic, and maternal variables used as independent adjusters were the following: maternal skin color (white/yellow and black/brown); maternal age (<20, 20–30, and >30 years); maternal educational level (0–4; 5–8; 9–11; and ≥12 years of study); family income (less than minimum wage, 1–7 times minimum wage, and >7 times minimum wage); maternal marital status (married or unmarried); number of children (one child and two or more children); smoking in pregnancy (no, yes); gestational hypertension (no, yes); gestational diabetes (no, yes); gestational thyroid disease (no, yes); gestational depression, previous breast surgery (no/yes); and previous breastfeeding experience (no/yes).
Exclusive breastfeeding
We collected data on disruption of EBF at the child's 30th day of life, asking the mother if any liquid or food other than breast milk was offered during the period and on which day this occurred. EBF was defined as exclusive consumption of breast milk without any other liquid and/or solid foods except drops or syrups of vitamins, oral rehydration, minerals, or medications. 7
Nutritional status
Prepregnancy body mass index (BMI) was calculated using prepregnancy weight and height reported in the maternity ward. BMI was used as the main independent variable, and those with BMI <30 kg/m2 were classified as nonobese, whereas those with BMI ≥30 kg/m2 were classified as obese according to the WHO criteria. 27
Childbirth variables
Childbirth variables included the following: route of birth (vaginal delivery/caesarean section); childbirth performed in a Baby Friendly Hospital (no/yes); breastfeeding in the first hour of life (no/yes); received artificial milk at the hospital (no/yes); and joint accommodation of mother and baby (no/yes).
Statistical analysis
Analyses were conducted using Stata v14.0. Descriptive data are presented as means and standard deviations for continuous variables and frequencies and percentages for categorical variables. The survival time of EBF in both groups of mothers (obese and no obese) was analyzed using Kaplan–Meier survival functions and the log rank statistic was used to compare the curves.
The Cox regression model was used to assess the association (hazard ratio [HR] and 95% confidence interval [CI]) between prepregnancy obesity and disruption of breastfeeding in the first month of life. Bivariate analysis was initially performed between various factors and the outcome. Variables with p < 0.20 were organized into blocks for inclusion in the multivariate analysis, with only those variables with p ≤ 0.05 remaining in the final model. The variables were organized as follows: Block 1 (demographic, socioeconomic, and maternal variables); Block 2 (variables related to childbirth) (Fig. 1). To verify whether the predictors were dependent on the time monitored, proportionality assumptions were established using the Hausman Test. When observing the interaction with the natural logarithm of time, the variables with p < 0.05 were removed from the final model for violating the assumptions of proportional risk.
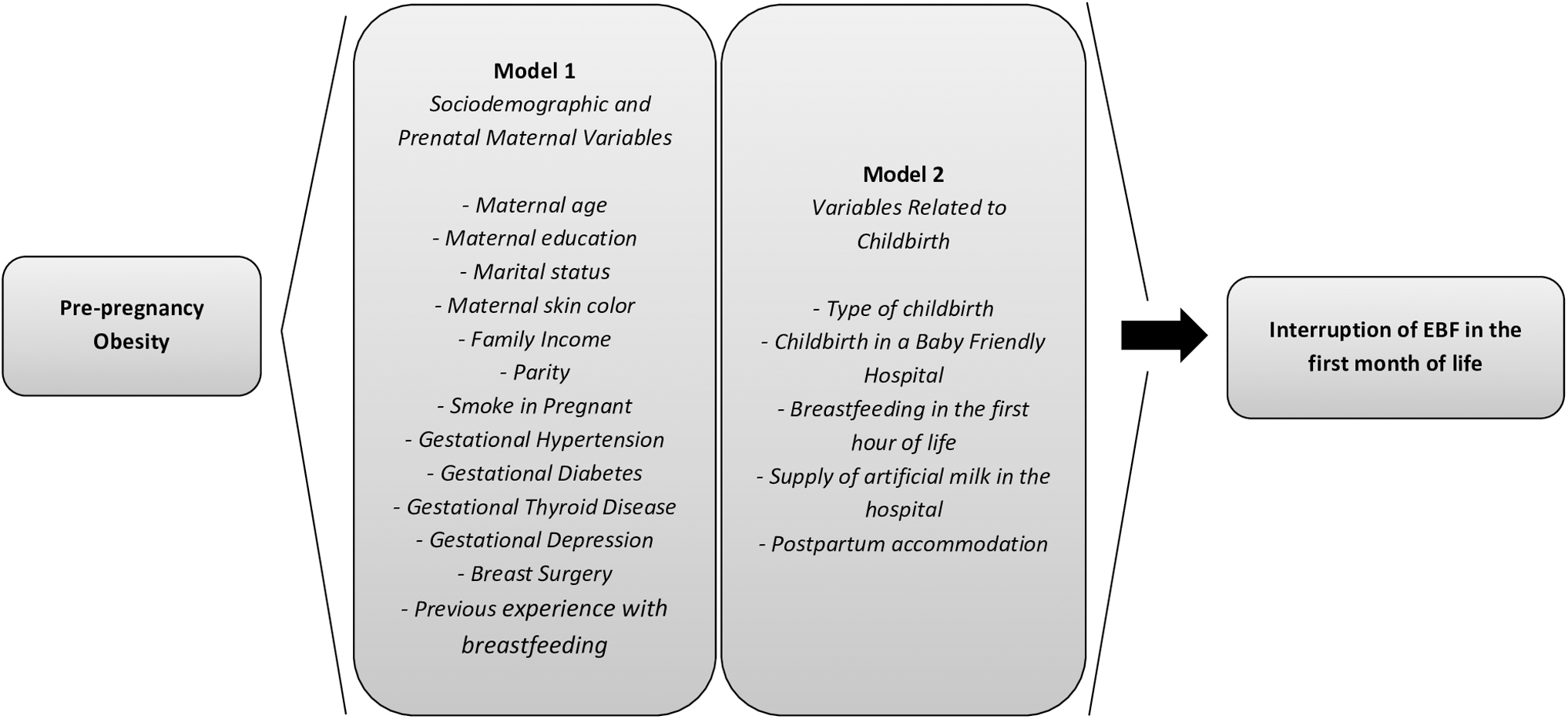
Conceptual model of possible confounding factors for the association between prepregnancy obesity and disruption of EBF in the first month of life. EBF, exclusive breast feeding.
Ethical considerations
Informed consent was obtained from the patients. The study was approved by Ethics Committee of the Multidisciplinary Health Institute, Federal University of Bahia.
Results
Of the original 388 mother–baby pairs, only 329 (84.8%) were available for follow-up at the end of the first month of life because of change in contact details or refusal to participate during the follow-up (Fig. 2). There was no significant differential loss in the variables maternal age, maternal education, and marital status when comparing the group that continued in the study (n = 329) with the group that was lost to follow-up (n = 59).
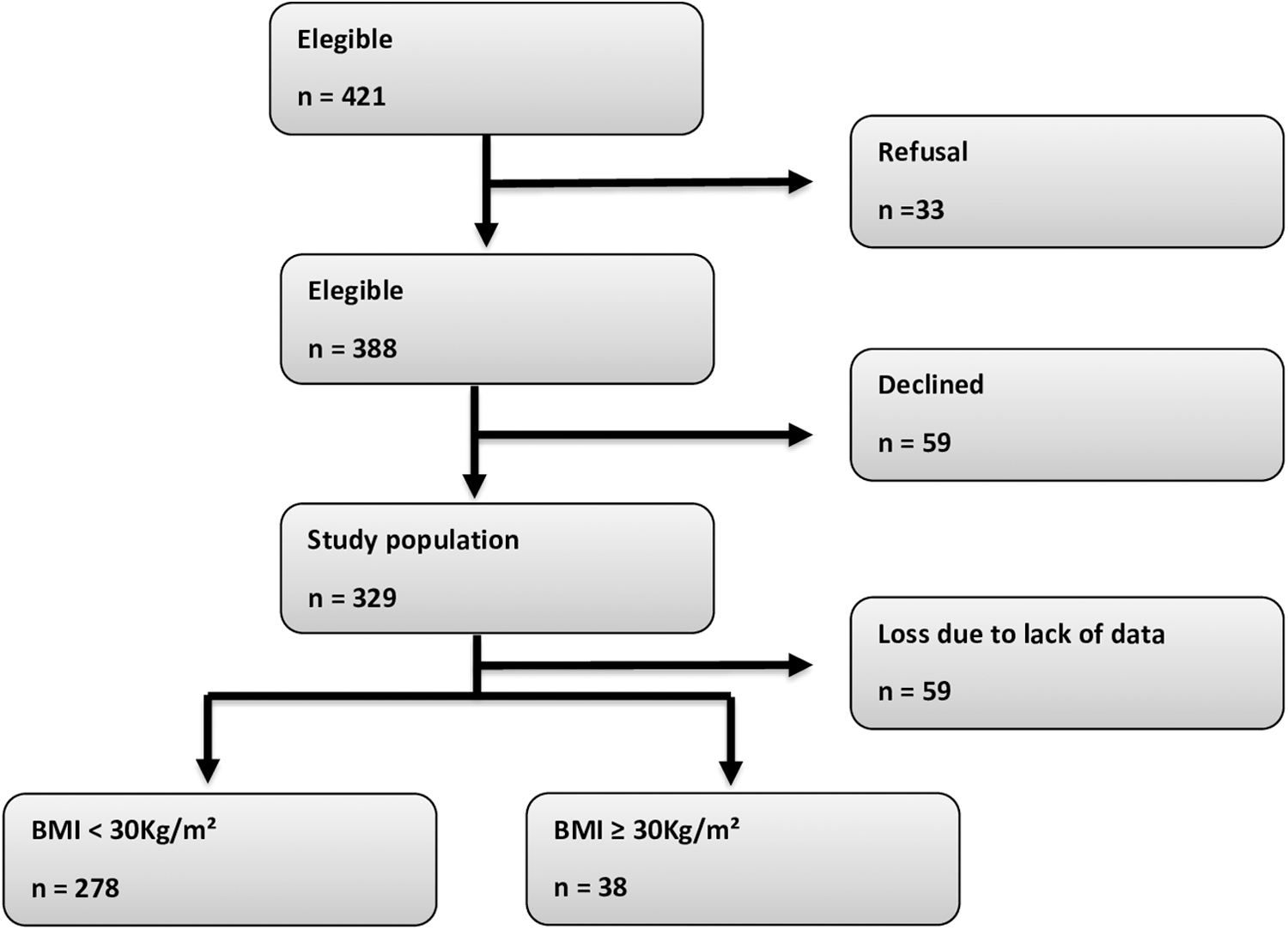
Enrollment of participants. BMI, body mass index.
The prevalence of prepregnancy obesity was 12% (95% CI: 9.0–16). The prevalence of EBF disruption in the first month of life was 41.1% in nonobese mothers (95% CI: 35.3–46.9) and 52.6% in obese mothers (95% CI: 36.3–68.4).
Table 1 summarizes the sociodemographic and maternal characteristics of the participants with complete available data, according to prepregnancy obesity. With the exception of gestational hypertension, there were no other variables with a statistically significant difference between the groups of obese and nonobese mothers. Among obese mothers, 81.5% were black/brown, 52,6% were 20–30 years, 74.1% had studied for at least 12 years, 77.8% were married, 2.6% smoked during pregnancy, 66.7% had had two or more children, 66.7% underwent caesarean section, and only 44.7% breastfed in the first hour of life. Regarding their comorbidities, 28.9% had gestational hypertension, 2.6% had gestational diabetes, and 2.6% had gestational depression, whereas no thyroid disease was observed among the obese mothers.
Sociodemographic and Prenatal Maternal Characteristics, According to Prepregnancy Obesity, of a Birth Cohort in Vitória da Conquista, Bahia, Brazil, 2017 (N = 316)
Figure 3 provides the estimated EBF survival curve in the first month of life, according to the presence of maternal obesity before pregnancy. The survival time of EBF was 23.3 ± 10.5 days (95% CI: 22.1–24.5) among nonobese mothers, and 20.7 ± 11.8 days (95% CI: 16.9–24.6) among mothers with prepregnancy obesity. There was proportionally shorter EBF survival time in the first month of life in mothers with pregestational obesity, which was significant (log rank p < 0.05). In the Cox regression model (Table 2), which was adjusted for the identified confounding variables (as listed in Fig. 1), the incidence of EBF disruption in the first month of life was 1.84 times higher in mothers with prepregnancy obesity (HR: 1.83; 95% CI: 1.08–3.11) than those without. In other words, compared with women who were not obese before pregnancy, those who were obese before pregnancy had an 83% higher risk of stopping breastfeeding exclusively within the first month of life.
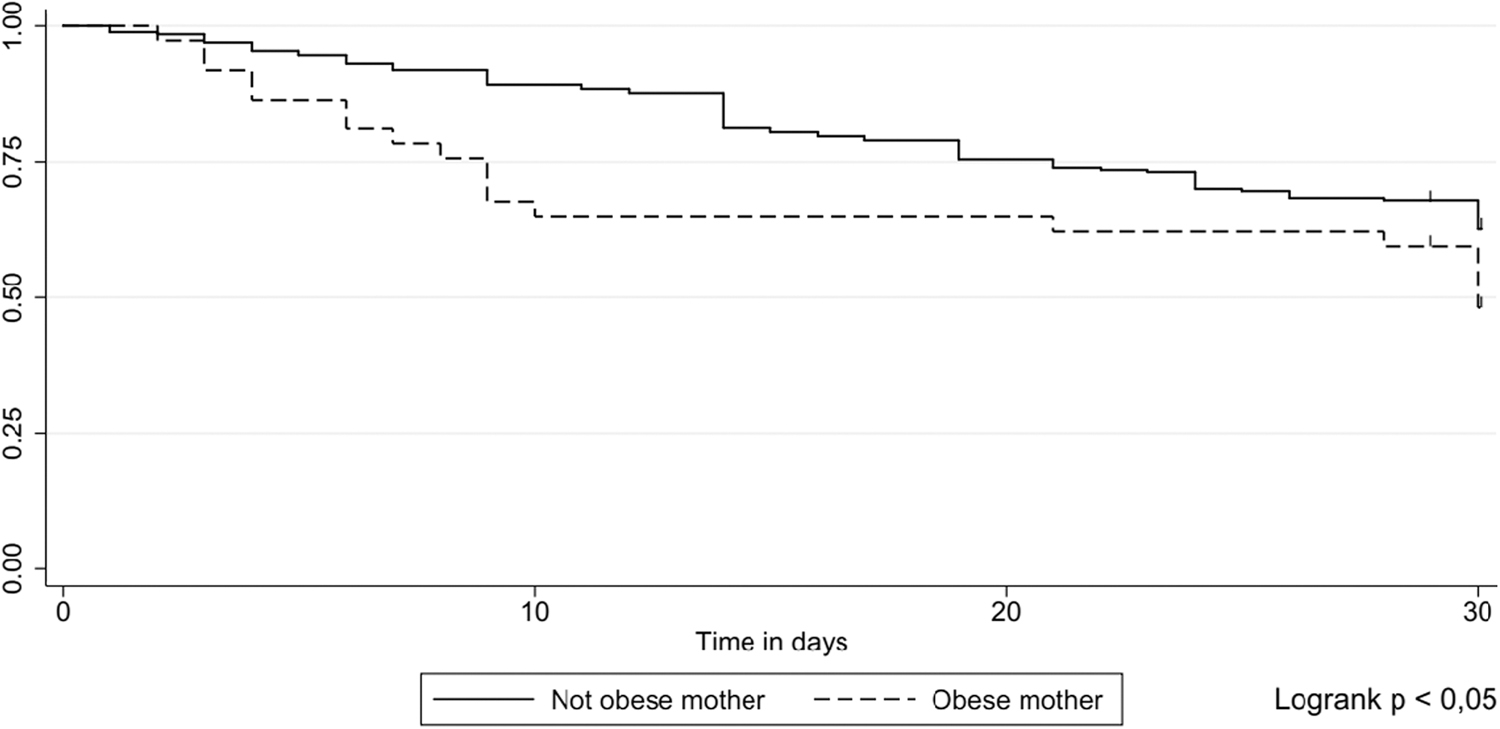
Survival curve following EBF disruption in the first month of life according to prepregnancy obesity, X, 2017 (n = 38). EBF, exclusive breast feeding.
Multivariate Analysis of Prepregnancy Obesity and Disruption of Exclusive Breastfeeding at 30 Days of Life in a Birth Cohort in Vitória da Conquista, Bahia, Brazil, 2017 (N = 316)
Model 1: adjusted between the Block 1 variables (skin color, maternal age and education; family income; marital status; smoking in pregnancy number of children; previous breast surgery; previous breastfeeding experience); gestational hypertension; gestational diabetes; depression in pregnancy; gestational thyroid disease. Model 2: adjusted for the variables of Model 1 as well as Block 2 variables (route of birth; childbirth in a Baby Friendly Hospital; breastfeeding in the first hour of life; received artificial milk at the hospital; and joint accommodation).
CI, confidence interval; HR, hazard ratio.
Discussion
This research found an association between prepregnancy obesity and shorter survival time of EBF in the first month of life. Only one study evaluated the association between prepregnancy BMI and disruption of EBF at 30 days in Brazil. The authors assessed 592 mothers and reported that those with prepregnancy obesity experienced disruption of EBF 1.14 times more often in the first month of life (p = 0.01) compared with nonobese or overweight mothers. 12 Another study on early weaning in prepregnancy overweight mothers found that among infants from mothers with normal pre-pregnancy BMI, the probability of being weaned at the age of 3 months was, on average, 13% lower than that of infants from obese mothers. 28
The prevalence of obesity found in our study was 12%, lower than the last published Brazilian data, which was 20.3%. 2 Obesity has been considered a pandemic, 29 and the increase in its prevalence among women of childbearing age raises the need for investigations of the impact of excess weight on pregnancy and the puerperium. A nationally representative longitudinal survey with >17,000 families in England and Wales showed that obese prepregnant women had lower rates of EBF in the first week and 4 months of life, compared with healthy mothers. 13
Another longitudinal survey conducted by the U.S. Food and Drug Administration (FDA) and Center for Disease Control and Prevention (CDC), with almost 5,000 women, revealed that overweight and obese mothers were significantly more likely not to breastfeed exclusively. 30 Also in the United States, a longitudinal study with 480 mothers found that obese class II (BMI, 35.0–39.9 kg/m2) women had increased odds of failing to exclusively breastfeed at hospital discharge compared with overweight women. 31 And more recently, a systematic review that included 23 studies also found that overweight and obese mothers have breastfeeding rates below those recommended by the WHO. 32
The literature points to multiple factors related to lower prevalence of EBF in overweight mothers. Biological factors can be explained by delayed or reduced lactogenesis and decreased response to prolactin; excess adipose tissue acting as a storehouse for steroid hormones and higher levels of progesterone, in addition to insulin resistance, which can potentially hamper several stages of lactation; baby's difficulty sucking large breasts, common in obese women; and increased risk of caesarean section, which is a recognized risk factor for late initiation of breastfeeding.4,5,28 Psychological factors, in contrast, are linked to problems with body image, low self-esteem, and embarrassment with body exposure. 33 In addition, sociocultural factors, such as African descent, lower socioeconomic status, and smoking during pregnancy, have been associated with a lower intention to breastfeed in obese women.33,34 It has been observed that many of these difficulties occur in the immediate puerperium and, therefore, compromise the production of breast milk at a crucial moment for the success of EBF because such production is directly related to the stimulus of suckling by the baby.
The prepregnancy BMI is a parameter that is easily calculated using the information on the pregnant woman's medical card. It can be useful in directing health services in the postpartum period regarding the promotion of EBF in overweight puerperal women as they belong to a population less likely to initiate and maintain breastfeeding. 13 Adequate professional monitoring can allow the obese mother to overcome the barriers of nutritional status and maintain the practice of EBF.
Our study findings also indicate a high prevalence of EBF disruption at the end of the first month of life and this prevalence is even higher among mothers with pregestational obesity. Studies in Brazil reported a 60% prevalence of EBF at 30 days11,35 but none of them rated these data according to the prepregnancy nutritional status. The WHO has determined that an EBF prevalence of 50–89% is a good indicator at 6 months of life. 7 However, this recommendation was not reached in Brazil even before the sixth month. 36 It is known that EBF reduces infant morbidity and mortality 35 ; therefore, disruption of EBF, especially so early, can damage the health of the mother and child in addition to increasing the costs of the Unified Health System for the treatment and control of diseases. 36
Few studies have controlled for confounders in the analysis of the association between prepregnancy obesity and early weaning, including the demographic, socioeconomic, behavioral, and gestational variables; the measure of effect tends to be even higher when adjusted, which suggests an underestimation of the measure of effect in studies that do not use such an analysis strategy. 33 A strength of the present investigation was the adjustment of the measure of effect according to the sociodemographic, maternal, and perinatal variables; consequently, we observed an increase in the HR from 1.62 to 1.83 in the final model. Therefore, prepregnancy BMI, when adjusted for the mentioned variables, seems to be a predictor of EBF survival time.
As a limitation of this study, it is important to mention that the prepregnancy anthropometric measurements were self-reported, which carries the risk of lack of standardization of measurements, as well as memory bias. As this study was derived from a larger project, the sample size calculation considered only the prevalence of EBF in Brazil, and not the prevalence of maternal obesity. In addition, the investigated city includes rural territorial extensions with locations far from the urban area, which could not be included in the study because of logistic and financial limitations. Therefore, it is not possible to generalize the results to the rural population with different habits and culture that can influence the practice of breastfeeding.
This study found an association between prepregnancy obesity and disruption of EBF in the first month of life. Based on the importance of breastfeeding for maternal and child health and considering that women with obesity in the preconception period constitute a risk group for early weaning, these results reinforce the need for a thorough approach to the practice of EBF in the first 6 months of life, both in prenatal care and in the immediate puerperal period. Based on this type of guidance, obese mothers can face the biological, psychological, and cultural barriers linked to their nutritional status to practice EBF for the recommended time.
Footnotes
Acknowledgments
The authors thank the mothers and the maternity hospitals involved in this study for their helpful contributions to the research.
Authors' Contributions
T.B.A.C.: conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, writing—review and editing. D.d.S.R.: conceptualization, data curation, formal analysis, investigation, methodology, writing—review and editing. M.P.N.: conceptualization, data curation, investigation, methodology, writing—review and editing. V.M.B.: conceptualization, data curation, investigation, methodology, writing—review and editing.
Ethical Approval
Informed consent was obtained from the patients. The study was approved by the Ethics Committee of the Multidisciplinary Health Institute, Federal University of Bahia (1.861.163).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.