
Abstract
Objective:
To determine intention to breastfeed (ITBF) rates among mothers exclusively using marijuana (eMJ) compared with electronic cigarettes (eEcig), tobacco products (eTob), or multisubstances (MS), nonusers (NU), and the influence of paternal presence and paternal substance use.
Study Design:
Cross-sectional study of parental survey responses merged with electronic birth certificates. Accounting for clinical and social determinants of health, analyses of ITBF included (1) all mothers, (2) single mothers, and (3) mothers with fathers.
Results:
Among all mothers (n = 1,073), eMJ, eTob, and MS users had lower odds of ITBF compared with NU. Only eMJ users had lower odds of ITBF for those without paternal presence. However, in those mothers with a paternal presence, odds of ITBF were similar to NU for eMJ, eTob, and MS users when accounting for paternal factors, including paternal substance use.
Conclusion:
Women exclusively using MJ have lower ITBF compared with NU. However, paternal presence mitigated this effect, independent of parental MJ use. The presence of fathers may represent a unique predictor for increased ITBF in MJ using mothers.
Introduction
Prenatal intention to breastfeed (ITBF) is closely associated with postpartum initiation and duration of breastfeeding. 1 Various maternal socioeconomic, biologic, and cultural variables influence ITBF and breastfeeding at birth.2,3 For instance, higher rates of ITBF are seen in older mothers and those with higher education.2,3 The presence of medical, psychiatric, or pregnancy-related complications are associated with decreased ITBF. 2 The impact of adverse life events and absence of social support systems, such as homelessness and intimate partner violence around the time of pregnancy, have also been recently linked with reduced ITBF.4,5
The use of tobacco around pregnancy is associated with reduced ITBF and lower duration of breastfeeding due to the perceived harmful effects.2,3,6 Although the use of substances such as alcohol and tobacco during pregnancy has steadily declined, an increasing number of pregnant women report electronic cigarette and marijuana (MJ) use.7,8 Higher MJ use has been attributed to legalization and a related perception of safety during pregnancy. 9 Approximately 3–5% of pregnant women nationally use MJ to self-medicate for nausea and vomiting or relieve anxiety.10–13 Furthermore, a recent study from Colorado showed that 5% of all women that ever-breastfed reported MJ use postnatally. 14 In addition, the overall duration of breastfeeding was shorter in women who reported any MJ use compared with those that did not. 14
The use of MJ while breastfeeding is concerning because MJ metabolites are detected in the breast milk for up to 6 weeks after intake, suggesting potential infant exposure. 15 Increasing evidence suggests risk of low-birthweight, preterm birth, small for gestational age, and neonatal intensive care unit admissions for infants born to mothers with antenatal MJ use.16,17 Assessment of outcomes of MJ exposure through breast milk has, however, been challenging due to prenatal use as well as the use of other substances. Given the concerns of MJ exposure through breast milk, multiple national organizations strongly discourage but do not recommend MJ use an absolute contraindication to breastfeeding.18–20 Furthermore, there is wide variation in the counseling provided by health care professionals to MJ-using mothers on the acceptability of breastfeeding.21,22
There is however, a paucity of studies looking at demographic factors influencing ITBF in this growing population of pregnant MJ users. Among adolescents with any MJ use before pregnancy, Sipsma et al. found reduced odds of maternal ITBF with any MJ use. 5 However, no study has looked at maternal ITBF with exclusive MJ use around the time of pregnancy in a broader maternal age range, or in conjunction with paternal sociodemographic factors and paternal MJ use.
A growing body of evidence has shown the importance of fathers in affecting maternal intention, initiation, and duration of breastfeeding.23,24 Expectant fathers influence maternal choice to exclusively breastfeed by providing emotional support, financial aid, as well as practical help.25,26 However, fathers' influence has been predominantly studied in the context of available administrative data as a proxy of paternal presence, or solely using marital status as primarily reported by mothers.27–29 There is also paucity of data surrounding paternal social determinants of health and substance use in relation to maternal breastfeeding. In fact, about 40% of all neonates born in the United States are to unmarried women. 30 Since marriage is not the only way for mothers to receive support from their partners, the assessment of paternal presence may be more relevant to study due to increasing cohabitation rates.27,30,31
Therefore, we sought to determine factors associated with ITBF in pregnant mothers exclusively using marijuana (eMJ), compared with those exclusively using electronic cigarettes (eEcig), tobacco products (eTob), multisubstance users (MS), and nonusers (NU), taking into account parental self-reported social determinants of health. In addition, we examined subgroups of mothers with and without paternal presence (outside of marital status) to ascertain the influence of fathers in the immediate postpartum period. Finally, we evaluated mothers with fathers to determine whether paternal characteristics, including paternal MJ use affected maternal ITBF.
Materials and Methods
Study population
This was a cross-sectional study of self-administered survey data collected from parents of all live-born singleton infants born at Maria Fareri Children's Hospital (MFCH) at Westchester Medical Center (Valhalla, NY), and six affiliate birthing hospitals in the Hudson Valley Region of NY. Data were collected between June 2016 and July 2020. The NY Medical College Institutional Review Board for the Protection of Human Subjects approved the study.
Inclusion/exclusion criteria
Inclusion criteria were consented English- and/or Spanish-speaking parents ≥18 years of age of all live-born singleton births. Exclusion criteria included non-English- or Spanish-speaking parents, pregnancies with multiple gestations, still births, or extramural deliveries. Mothers with missing self-reported data on substance use or ITBF were also excluded. Same-sex couples were excluded from the study due to small numbers (n = 2). Mothers who had a corresponding completed paternal survey were included as having “paternal presence,” irrespective of their marital status. Paternal survey responses were only included if a corresponding maternal survey was completed. The question that defined lack of paternal presence was, “What was your marital status?” Choices included, “Single, never married; Married or domestic partnership; Separated; Divorced; and Widowed.” Mothers who responded as being “single, never married”; AND a paternal survey was not completed were categorized as single mothers.
Regardless of marital status, if a paternal survey was completed, those mothers were categorized as mothers with fathers. Therefore, mothers who self-reported as “married or in a domestic partnership, widowed, separated, or divorced” without a corresponding paternal survey were excluded from subgroup analysis. This was done to prevent underestimating paternal impact due to only having maternal data and not the corresponding fathers. 27
Data collection
Two validated survey tools were used for this study (maternal and paternal survey). These tools described in detail by Wanasinghe et al. assessed a broad set of questions related to social determinants of health, substance use, adverse life events, and lifestyle behaviors.32–37 Survey data were merged with data from electronic birth certificate, from which information on receipt of prenatal care, foreign-born status, maternal- and pregnancy-related conditions were obtained. 27
Variable definitions
Exposure groups classified mothers with exclusive use before or during pregnancy, of MJ (eMJ: MJ, pot, bud, hashish, K2), eEcig, eTob (hookah, smokeless tobacco, snus pouches, cigarettes, and cigars), MS (use of two or more of: electronic cigarettes, MJ, or tobacco products), and non users (absence of use of electronic cigarettes, MJ, and tobacco products). eMJ was defined as any use 1 month before or during pregnancy.27,32,33 eEcig was defined as any use 12 months before or during pregnancy.27,32,34 eTob was defined as any use 3 months before or during pregnancy.27,32,34
The primary outcome assessed was ITBF. ITBF was determined based on response to the question, “During this pregnancy, what did you think about breastfeeding your new baby?” “Yes” was defined as “I knew I would breastfeed,” or “I thought I might breastfeed.” “No” was defined as “I knew I would not breastfeed,” or “I didn't know what to do about breastfeeding.” 32
Covariates included social determinants of health such as self-reported parental race/ethnicity, education, exercise, employment status, adverse life event score, alcohol or illicit drug use, primary payor at delivery (Medicaid or Child Health Plus), foreign born status, prenatal care, and high-risk pregnancy conditions in mother. Self-reported race/ethnicity was classified into Non-Hispanic White, Non-Hispanic black, Hispanic, and Others. 34 Education was dichotomized as less than or equal to high school completion and greater than high school completion, and served as a proxy for socioeconomic status, as income was not assessed due to lower likelihood of being disclosed. 34
Adverse life event score was calculated based on the presence of ≥3 of 14 factors, including homelessness, trouble paying rent or other bills, family sickness, partner incarceration, unwanted pregnancy, military deployment, partner separation, partner discord, a death of close relative/friend, presence of excessive alcohol or drug use in close family member/friend, and reduced or loss of employment.32–34 Exercise was defined as physical activity ≥3 days per week or <3 days per week during the 12 months before the pregnancy.32,33
Alcohol or illicit drug use was defined as any use 3 months before or during the pregnancy.32–34 Mothers with high-risk pregnancy conditions were defined as either <20 or >34 years 38 ; or with diagnosis of prepregnancy or gestational diabetes or hypertension, previous preterm/low-birthweight, abruption/vaginal bleeding, eclampsia, body mass index >30, other chronic illnesses. Receipt of prenatal care was defined as any prenatal care received (yes/no). High-risk-age fathers were defined as age <20 or >39 years. 39 Additional paternal variables were defined similarly to the maternal factors. 37 We also assessed father's perception of their influence on maternal ITBF, based on response to the question, “During your partner's pregnancy with this baby, did you think you had a role in your partner's decision to breastfeed? “Yes” was defined as “Yes,” or “Somewhat.” “No” was defined as “No,” or “Don't know.” 32
Statistical analysis
ITBF and demographics were compared by exclusive use (eMJ, eEcig, eTob, MS, NU) in bivariate analysis using chi-square or Fisher's exact tests. ITBF in conjunction with substance use was first analyzed among all mothers. Two subgroup analyses subsequently assessed ITBF in relation to substance use among (1) single mothers and (2) mothers with fathers. Percentages were calculated based on the number of responses to each question.
Multiple logistic regression models were used to determine the association between maternal eMJ use and maternal ITBF after controlling for covariates. Covariates were selected if they had a p-value of ≤0.1 in the bivariate analysis, or were known to be associated with outcome of ITBF. Final models controlled for race/ethnicity, education, adverse life event score, foreign-born status, high-risk pregnancy conditions, alcohol or illicit drug use, prenatal care received, and primary payor. As employment is collinear with education and did not change the results, it was not included in the final model. Our primary model included ITBF in all mothers. Subgroup multivariate analyses examined eMJ and ITBF among mothers based on the presence or absence of father, and controlled for same factors noted above in the model with all mothers. The model for mothers with fathers and ITBF adjusted for the maternal characteristics noted above and paternal characteristics, including high-risk age, adverse life event score, alcohol or illicit drug use, education, foreign-born status, and paternal substance use (eMJ, eEcig, eTob, MS, and NU).
Receiver Operator curves with concordance index (C-statistic) were generated to assess predictive accuracy of models. Statistical significance was determined by a p-value <0.05. Analyses were performed using Stata version 16.0 (StataCorp. 2019. Stata Statistical Software: Release 16; StataCorp LLC, College Station, TX).
Results
Study population
A total of 2,060 mothers and 955 fathers were approached of which 1,154 mothers and 344 fathers consented for the study (consent rates among mothers and paternals surveyed were 56% and 36%, respectively; Fig. 1). Of the consenting mothers, 50 had incomplete consent forms and 2 withdrew consent. Additionally, 29 mothers were excluded because of incomplete or missing survey data on substance use or ITBF. A total of 1,073 mothers were included in the final analysis. Three hundred forty-four mothers had a corresponding paternal survey. Seven paternal surveys were eliminated due to missing data. Overall, we had 337 mothers with fathers (completed paternal survey regardless of marital status), and 327 single mothers (single/never married AND no paternal survey). There were 409 mothers who did not meet criteria to fall in either subgroup (i.e., had any marital status other than single/never married, AND no paternal survey), and were excluded from the subgroup analysis.
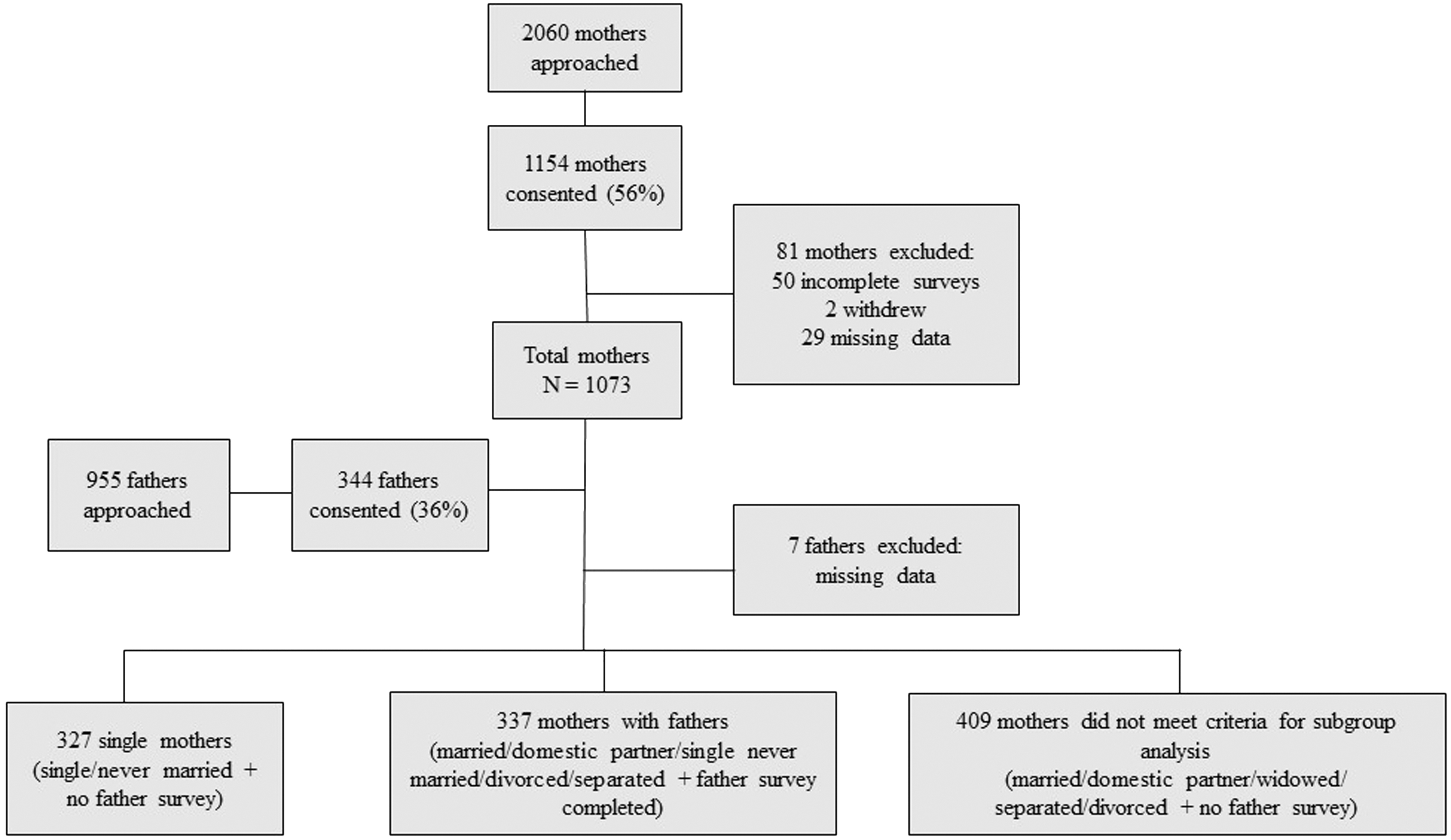
Flowchart of subjects approached, consented, and included in final analysis. A total of 2,060 mothers and 955 fathers approached, of which 1,154 mothers and 344 fathers consented. Final sample size included 1,073 mothers, categorized as 327 single mothers and 337 mothers with fathers.
All mothers across exposure groups
Overall, 73% of women had a positive ITBF. Among all mothers, exposure groups included 2.9% eMJ, 1.6% eEcig, 9% eTob, 8.6% MS, and 77.9% NU (Table 1). Mothers using eMJ, eTob, and MS had significantly lower ITBF compared with NU. Mothers who were NU were more likely to be older, educated, employed, and foreign born. Mothers with MS use were more likely to report adverse life events and alcohol/illicit drug use. Mothers using eEcig had increased rates of high-risk pregnancies. Controlling for maternal race/ethnicity, education, adverse life event score, foreign-born status, high-risk pregnancy conditions, alcohol or illicit drug use, receipt of prenatal care, and primary payor for delivery, eMJ users exhibited lower odds of ITBF compared with NU (odds ratio [OR] 0.41, confidence interval [CI] 0.19–0.92). Similarly, eTob (OR 0.56, CI 0.34–0.92) and MS (OR 0.44, CI 0.26–0.76) users had lower odds of ITBF compared with NU. Additionally, eEcig users did not differ from NU. This model assessing substances compared with NU accurately predicted 64% of ITBF (C-statistic = 0.64).
Differences in Sociodemographic Characteristics by Substance Use Among All Mothers Sampled
eMJ users had significantly lower ITBF compared with NU among all mothers.
Mothers <20 or >34 years or with medical conditions, including prepregnancy or gestational diabetes or hypertension, previous preterm/low-birthweight, abruption/vaginal bleeding, eclampsia, BMI >30, other chronic illnesses.
Alcohol use 3 months before or during pregnancy, illicit substance use 1 month before or during pregnancy.
Bold and * designates p < 0.05.
BMI, body mass index; eEcig, exclusive e-cigarette use; eMJ, exclusive marijuana use (pot, bud, hashish, K2); eTob, exclusive tobacco product use (hookah, smokeless tobacco, snus pouches, cigarettes, and cigars); ITBF, intention to breastfeed; MS, multi-substance: use of ≥2 of: e-cigarette, marijuana, or tobacco products; NU, no substance users (neither marijuana, e-cigarette, and tobacco products); SD, standard deviation.
Mothers without paternal presence and ITBF (single mothers)
Single mothers exhibited the following patterns of substance use: 4.3% eMJ, 2.1% eEcig, 15.3% eTob, 15.3% MS, and 63% NU (Table 2). Single mothers that were NU were more likely to be employed, while eEcig users were more likely foreign born. MS-using mothers were younger, and reported higher adverse life events and alcohol or illicit drug use. Adjusting for the same factors as above, single mothers using eMJ had lower odds of ITBF compared with NU (OR 0.16, CI 0.04–0.57). Other substances (eEcig, eTob, MS) did not differ from NU. This model correctly predicted 72% of ITBF (C-statistic = 0.72).
Differences in Sociodemographic Characteristics by Substance Use Among Single Mothers
No significant difference in ITBF across exposure groups in single mothers.
Mothers <20 or >34 years or with medical conditions, including prepregnancy or gestational diabetes or hypertension, previous preterm/low-birthweight, abruption/vaginal bleeding, eclampsia, BMI >30, other chronic illnesses.
Alcohol use 3 months before or during pregnancy, illicit substance use 1 month before or during pregnancy.
Bold and * designates p < 0.05.
BMI, body mass index; eEcig, exclusive e-cigarette use; eMJ, exclusive marijuana use (pot, bud, hashish, K2); eTob, exclusive tobacco product use (hookah, smokeless tobacco, snus pouches, cigarettes, and cigars); ITBF, intention to breastfeed; MS, multisubstance: use of ≥2 of: e-cigarette, marijuana, or tobacco products; NU, no substance users (neither marijuana, e-cigarette, and tobacco products); SD, standard deviation.
Mothers with paternal presence and ITBF (mother–father dyads)
Maternal rates of substance use among mothers with a father present were 3% eMJ, 1% eEcig, 8% eTob, 7% MS, and 81% NU (Table 3). ITBF did not differ across exposure groups. NU mothers were more likely to be educated and foreign born. MS users were more likely to report adverse life events and alcohol/illicit drug use.
Differences in Sociodemographic Characteristics by Substance Use Among Mothers with Corresponding Paternals Survey Completed
No significant difference in ITBF across exposure groups in mothers with fathers.
Mothers <20 or >34 years or with medical conditions, including prepregnancy or gestational diabetes or hypertension, previous preterm/low-birthweight, abruption/vaginal bleeding, eclampsia, BMI >30, other chronic illnesses.
Alcohol use 3 months before or during pregnancy, illicit substance use 1 month before or during pregnancy.
Bold and * designates p < 0.05.
BMI, body mass index; eEcig, exclusive e-cigarette use; eMJ, exclusive marijuana use (pot, bud, hashish, K2); eTob, exclusive tobacco product use (hookah, smokeless tobacco, snus pouches, cigarettes, and cigars); ITBF, intention to breastfeed; MS, multisubstance: use of ≥2 of: e-cigarette, marijuana, or tobacco products; NU, no substance users (neither marijuana, e-cigarette, and tobacco products); SD, standard deviation.
Table 4 shows characteristics of fathers by their substance use. Rates of use among fathers were 5.4% eMJ, 1.5% eEcig, 16.4% eTob, 15.7% MS, and 61% NU (Table 4). A larger proportion of eMJ fathers were Hispanic. This group also reported higher alcohol or illicit drug use. Fathers using MS were more likely to have adverse life events, whereas NU were more likely foreign born.
Demographic Characteristics of Fathers Compared by Substance Use
Demographic characteristics of fathers compared by substance use differed by race, adverse life event score, foreign-born status, and alcohol or illicit drug use.
One father had missing data on substance use.
Alcohol use 3 months before or during pregnancy, illicit substance use 1 month before or during pregnancy.
Father's age <20 or >39 years.
Bold and * designates p < 0.05.
eEcig, exclusive e-cigarette use; eMJ, exclusive marijuana use (pot, bud, hashish, K2); eTob, exclusive tobacco product use (hookah, smokeless tobacco, snus pouches, cigarettes, and cigars); MS, multisubstance: use of ≥2 of: e-cigarette, marijuana, or tobacco products; NU, no substance users (neither marijuana, e-cigarette, and tobacco products); SD, standard deviation.
After adjusting for maternal covariates, mothers with paternal presence were as likely to breastfeed as NU (OR 2.0, CI 0.39–10.39). Results were similar (OR 1.71, CI 0.29–9.86) even after controlling for paternal factors (race/ethnicity, high-risk age, adverse life event score, alcohol or illicit drug use, education, foreign-born status, paternal use of eEcig, eMJ, eTob, MS, or NU) in addition to aforementioned maternal factors. This model, which took into account both maternal and paternal factors correctly predicted 73% of ITBF (C-statistic = 0.73). Both models (paternal presence only and with additional paternal demographics and substance use) showed no difference in ITBF in eTob and MS users. Of note, due to small numbers of eEcig users among mother–father dyads, ITBF was not able to be assessed in these subgroup analyses.
Discussion
Our study is among the first to describe ITBF in pregnant exclusive MJ users, while also accounting for maternal social determinants of health. It is also the first to examine the joint effects of paternal self-reported sociodemographic characteristics and exclusive MJ use on maternal ITBF. Despite an increase in popularity of MJ use during pregnancy, our results show that pregnant MJ users overall, as well as in the absence of fathers, had significantly lower ITBF compared with NU. However, in the presence of fathers, MJ-using mothers were as likely to intend to breastfeed as NU.
The incidence of exclusive antenatal maternal MJ use in our study was 3%, comparable to rates reported in other studies.10–12 Using a limited study population of adolescent couples, Sipsma et al. found lower rates of ITBF in mothers with any (nonexclusive) MJ use before pregnancy. 5 Their study also noted that any paternal MJ use did not affect ITBF, similar to our results. However, our nonadolescent patient population differs in analyzing ITBF among both single mothers as well as mothers with fathers. Although Sipsma et al. adjusted for relationship factors and intimate partner violence, we were able to account for a broader range of antenatal adverse life events such as homelessness, loss of employment, and partner incarceration, as well as foreign-born status.
We used a unique definition of paternal presence as a proxy for paternal involvement to compare mothers with and without a father. This helped us better evaluate paternal impact outside of marital status. Maternal perception of fathers' attitudes is an important factor in mothers' decision to breastfeed. 23 A pregnant unmarried mother cohabiting with the father may still receive emotional, educational, and/or financial support from the father. This assistance might ultimately influence her ITBF, compared with a single pregnant woman. We speculate that fathers' presence may alter overall maternal perception of safety of breastfeeding with MJ use. In other words, in the presence of a father, the perceived benefits of breastfeeding may outweigh the potential apparent risks of MJ exposure through breast milk.
Our study is subject to limitations. Disclosure of substance use can be subject to recall bias. However, as the survey captured use over a short time period, accurate recollection is more likely. Another potential limitation is that of survey-based underreporting as compared with toxicology studies. In the absence of universal screening for MJ, self-reporting during a physician encounter is the standard means of assessment, which would inform counseling regarding MJ use and breastfeeding. Another limitation is the reduced response rate. Increased medical, educational, and practical demands placed on new parents during their postpartum hospitalization stay may affect the time parents can devote to survey completion. Our response rates for self-reported substance use were comparable to those reported by other studies. 40 Although we did not assess receipt of antenatal counseling regarding breastfeeding from health care staff or family friends, many mothers perceive informal help from their spouse or partner to be more important than formal support from health care providers. 23
Our study has several strengths. While past studies have analyzed any MJ use, a variable which can include concomitant use of other substances, our study focused on exclusive MJ use, allowing for better discernment of the individual impact of this specific substance on ITBF. In addition, obtaining self-reported paternal data outside of marital status, including self-reported race, substance use, and adverse life events may provide a more accurate assessment of paternal characteristics compared with traditionally used administrative datasets.28,29 Paternal social factors, including self-reported stressors, have been overlooked as a potential contributor to outcomes related to breastfeeding, necessitating studies like ours.
In the context of greater state-based MJ legalization and overall use, our study has important implications regarding prenatal counseling for mothers and fathers around breastfeeding. In addition to eliciting a history of detailed substance use, clinicians should proactively include the father, irrespective of their marital status in discussions about breastfeeding. Further studies should identify the mechanisms by which paternal support may influence the observed increased ITBF rates in MJ-using mothers with paternal involvement.
Footnotes
Acknowledgment
The authors thank the medical students and research staff who helped them with the study methods and data entry.
Authors' Contributions
N.J. drafted the article and performed the initial analysis. S.S. assisted with analysis, reviewed drafts of articles, and made substantial contributions to draft. D.W., K.D. and A.B. performed preliminary analysis for the project. A.P. assisted in biostatistical analysis. C.G. assisted with Institutional Review Board Applications at participating sites and contributed to data acquisition. H.L.B. conceived the original project, scientific design, analysis plan, and reviewed multiple drafts of the article. All the authors have accepted responsibility for the entire content of this submitted article and approved submission.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.