
Abstract
Aim:
Cesarean section often translates to negative impacts on breastfeeding rates. This study aims to evaluate the effect of a mobile application on breastfeeding outcomes among mothers who had cesarean sections using a randomized controlled trial in Vietnam in 2020–2022.
Methods:
A triple-blinded randomized trial of a mobile application was conducted. The mobile application was tailored to a Vietnamese cultural context with two separate versions, one for the intervention and one for the control. The intervention group version auto-generated three messages per week and linked with the information in the application's library content to improve breastfeeding practices. In contrast, the control group's version of the application sent messages on related general maternal and child health care. Pregnant mothers were recruited during their antenatal visits and randomly assigned to one of the two groups. Outcomes of interest included early initiation of breastfeeding and exclusive breastfeeding rates.
Results:
A total of 293 in the intervention group and 275 mothers in the control who had undergone cesarean sections were included in the analyses. Significant increases were observed in the intervention group for early initiated breastfeeding within 2 hours (adjusted odds ratio [aOR] = 1.50, 95% confidence interval [CI]: 1.01–2.24) and exclusive breastfeeding during hospital stay (aOR = 1.60, 95% CI: 1.03–2.48).
Conclusion:
Our results support the use of a theory-based and designed mobile phone application as a part of a promising intervention to improve breastfeeding outcomes among mothers who have cesarean sections.
Key Notes
Although cesarean sections have been reported to have negative impacts on breastfeeding rates, evidence of the effectiveness of the smartphone application intervention on this group has not been reported. Our results suggest that installing a smartphone application, which automatically generates three messages per week linking detailed support information from the application's library during pregnancy is a promising tool for increasing breastfeeding rates among mothers who have cesarean sections.
Introduction
A
As mothers are the most influential decision-makers on breastfeeding practices, 8 the increasing accessibility of mobile phones may offer an effective and sustainable intervention solution at a relatively low cost. Mobile phone-based interventions have the potential to improve breastfeeding outcomes and reduce infant health problems among mothers in general.9–11 Despite the rising cesarean delivery rate among women in most countries worldwide, trials addressing the effect of a mobile breastfeeding application in this population could not be found in the literature.
To address this gap, we developed a mobile application and conducted a two-arm parallel triple-blinded randomized controlled trial among mothers who have cesarean sections in two hospitals in Hanoi, Vietnam. Vietnam is a low-middle income country with low exclusive breastfeeding rates 12 and a high cesarean delivery prevalence (∼40–50% in urban areas). 13 The mobile application was developed using the Behavioral Intervention Technology Model 14 to provide notifications and information encouraging exclusive breastfeeding in the intervention group and on maternal and child health care in the control group.
The messages sent to the intervention group included information on the benefits of and mothers' ability to initiate breastfeeding soon after birth, and exclusively breastfeed regardless the mode of delivery. This study aims to report the effect of the mobile application in improving breastfeeding rates (early initiation of breastfeeding, exclusive breastfeeding rates at 1, 4, and 6 months postpartum) among cesarean births. The hypothesis is that mothers in this population who received specific information on promoting breastfeeding were expected to have higher breastfeeding rates than those who only received general information on maternal and child health care.
Methods
A two-arm parallel allocation ratio 1:1 triple-blinded randomized controlled trial (clinical registration number: ACTRN12619000531112) was conducted between 2020 and 2021 in two hospitals in Hanoi, Vietnam. The protocol was approved by the Ethical Review Boards (reference HRE2019-0143-03 and 28/2019/YTCC-HD3) and has been published in 2020. 15
Participants
The study targeted mothers who delivered by a cesarean section. As the mobile application was installed during the prenatal period and the mode of delivery (i.e., whether the mother would deliver by cesarean section) was not yet known, we recruited all mothers who visited two selected hospitals for antenatal care (the Hanoi Obstetrics & Gynecology Hospital and Dong Anh General Hospital). Both hospitals are located in urban areas where 85% of residents own a smartphone. We selected Hanoi city because it has lower breastfeeding outcomes and higher cesarean delivery prevalence (50%) than the national average and the internet remains the second most popular source of information on infant feeding. 16
Inclusion criteria were being at 24–36 weeks of gestation, having an intention to deliver in one of the selected hospitals, owning a smartphone, and carrying a single fetus. Mothers under high-risk pregnancy treatments were excluded. The high-risk pregnancies exclusion criteria were defined as mothers who were referred from lower-level hospitals for antenatal visits and follow-up; had been advised by health care providers not to breastfeed, and were at risk of premature birth. During the trial, the application was inactivated for mothers who had a stillbirth or a newborn death and excluded them from the analysis.
Intervention
The mobile application was designed and developed using a mixed-methods approach with formative research, testing, and iterations. Information from relevant studies, 22 in-depth interviews with mothers, and 49 self-administered interviews were used to identify the main themes and construct the application's features. We developed a simple and user-friendly interface with text notifications that carried behavior change messages and suggestions for further resources in the application's library.
The application auto-generated notifications three times per week during pregnancy and twice per week after delivery. The notifications were developed to appear on the phone's locked screen and notification center to convey the messages and encourage mothers to use the application. When mothers tapped on a notification, it opened the related page in the application's library content. Mothers could reread and search for information in the application. The application worked without internet access after installation was complete.
During pregnancy, 3 messages were auto-generated weekly, and 12 key messages were repeated after 4 weeks. The messages for the intervention group were carefully developed and tested following steps on “developing and pretesting text messages for health behavior change.” 14 The set of 12 key messages targeted at both mothers and family members were developed based on target behaviors, key determinants, and improving breastfeeding self-efficacy theories, 17 and were delivered during the prenatal period. Four themes of the messages had been identified, including (1) believing breast milk is the best option for newborns until 6 months; (2) believing mothers have enough milk and can breastfeed early including those who have cesarean sections; (3) planning for breastfeeding exclusively; and (4) involving the husband and family members in preparing for exclusive breastfeeding.
Eight of the 12 messages targeted mothers who have had cesarean sections, either in the messages or in the application's library contents. Information focused on the importance, benefits, and ability of mothers to initiate breastfeeding early and to exclusively breastfeed regardless of whether they had a vaginal or cesarean delivery. Mothers were encouraged to involve health care providers and family members to support early and exclusive breastfeeding in the case of either vaginal or cesarean delivery. Examples of messages and information from the application's library are presented in Appendix Table A1.
Each message was connected with a relevant entry in the application's library, which would then present three to five paragraphs explaining or demonstrating the message contents. Pictures were also included to illustrate or highlighted the message's content or highlight it with relevant visual cues, alongside references, and links for further reading. The 12 key messages were sent repeatedly, but the detailed information linked in the application's library changed based on gestational age during pregnancy and the child's age to retain mothers' use of the application.
Another 48 messages were developed to send twice per week after delivery. Messages emphasizing the importance of breastfeeding exclusively were reinforced at 1 and 4 months. Some of the messages sent after birth addressed common breastfeeding problems, including sore nipples, breast engorgement, low milk supply, and mastitis. Other messages addressed needs identified by mothers in the formative phase of the study, such as diet and physical activities for breastfeeding mothers, dealing with child's crying, and child's weight.
Eligible mothers who agreed to participate in and signed the consent form had the application installed on their mobile phones. Face-to-face interviews were used at baseline and phone calls for follow-up data collection. Research Electronic Data Capture (REDCap) 18 software was used to capture interview data. The administrator assigned and activated the application as either the intervention or control version. Whereas the intervention received the 12 key messages and linked entries in the application library related to improving breastfeeding outcomes, the control group received the information on maternal and child health care in general.
Outcomes
The primary outcome of the study was exclusive breastfeeding during the hospital stay. Secondary outcomes of interest included early initiation of breastfeeding within 2 hours and exclusive breastfeeding at 1, 4, and 6 months postpartum. Women were contacted and interviewed by phone calls at discharge, 1, 4, and 6 months after delivery by trained public health assistants. Early initiation of breastfeeding was assessed using the question “How long after delivery did you breastfeed your baby for the first time?” and recoded into within 2 hours and beyond 2 hours. Exclusive breastfeeding during hospital stay was defined by two questions “How did you feed your baby during hospital stay?” and “What else did you feed your baby?” If a mother fed her newborn with breast milk only (either by breastfeeding or by spoon/bottle) and nothing else except vitamins, and oral rehydration salts, she was classified as exclusive breastfeeding during hospital stay according to the definition of the World Health Organization. 19
Similarly, exclusive breastfeeding at 1, 4, and 6 months postpartum was defined from the two questions “How did you feed your baby since the last interview?” “What else did you feed your baby since the last interview?” and the exclusive breastfeeding status from the previous interview.
Data collection and quality assurance
All interviews were checked by a field supervisor for completeness and verified and endorsed by the administrator using the REDCap system. Data were collected from May 2020 to July 2021 when there were some sporadic COVID-19 cases in the city. The final follow-up survey was completed before the fourth wave of the COVID-19 outbreak became severe in Vietnam. The study conducted all follow-up interviews by phone due to the long periods of “lock-down” and disruption to physical contacts during the COVID-19 pandemic. The data collection procedure was approved by the participating hospitals as consistent with COVID-19 protocols.
Data were checked for validity and reliability by extracting information from hospital records. The participants were identified by matching their name, birthdate, address, and telephone number. Three variables selected for comparison with hospital records were the child's sex, birth weight, and mode of delivery. The selection was based on available data in the two hospitals' records and recommendations from the previous studies on the validity and reliability of self-reporting in maternal and child health indicators. 20
Sample size
A total of 1,266 mothers were consecutively recruited and allocated into either the control or intervention group. The two hospitals had cesarean rates of ∼50% of deliveries. We expected to have about 500 mothers having cesarean sections after accounting for a maximum of 20% of loss of follow-up at 6 months. 21 Mothers were allocated to the intervention or control group with an enrollment ratio of 1:1. As exclusive breastfeeding during the hospital stay was selected as the primary outcome, assuming the incidence would increase from 6.7% 22 to 15% in the intervention group, the required sample size was 438 (219 per group) with 80% power at a 5% level of significance.
Randomization
Permuted-block randomization with block sizes of 2, 4, and 6 was undertaken and stratified by maternal age (≤30 or >30 years), education level (under tertiary educational level or above), and parity (primiparous or multiparous) to achieve a 1:1 ratio in each treatment group. 23 These are high-impact factors of breastfeeding outcomes reported in the previous study. 24 An administrator generated the randomization list using the Stata “ralloc” module (StataCorp, College Station, TX), randomized the participants into intervention or control groups, and activated the application remotely. Participants, data collectors, and data analysts were all blinded to the group assignment.
Statistical methods
Kappa statistic was applied to test the inter-rater reliability of data collected and extracting information from hospital records. We used an “intention-to-treat analysis” that included all mothers who had undergone cesarean sections in the study for the analysis. 25 Sociodemographic characteristics of the participants were compared between intervention and control groups, and between the loss to follow-up and the final sample retained in the study. Continuous and categorical variables were reported as mean (standard deviation) and frequency (%), respectively. The differences between groups were assessed using a Pearson's χ 2 test (categorical variables) or an independent samples t test (continuous variables). The breastfeeding rates (%) at each time point alongside their perspective 95% confidence interval (CI) were calculated for each group. Differences between the two groups were statistically significant at p-values <0.05.
Effects of the intervention on breastfeeding outcomes at each time point were assessed using a Pearson's χ 2 test and measured by odd ratios and 95% CIs. The effects were then adjusted for other independent variables, including age, education level, parity, prepregnancy body mass index, gestational age at the time of enrollment, and exclusive breastfeeding intention using multiple logistic regression analysis. These independent variables were chosen from a review of the existing literature and current studies on early essential newborn care in Vietnam and collected at the baseline survey in the hospitals.24,26,27
Exclusive breastfeeding intention was defined as the mother “intending to breastfeed her child and not give any liquid or food until 6 months.” This variable was collected at the time of enrollment. Prepregnancy body mass index was calculated from the self-reported height and weight of the mother before pregnancy. Prepregnancy body mass index, gestational age at the time of enrollment, and maternal age were included in the multiple logistic regression models as continuous variables, whereas other variables were treated as categorical.
All analyses were performed using SPSS (IBM Corp. Released 2017; IBM SPSS Statistics for Windows, Version 25.0; IBM Corp, Armonk, NY).
Results
Participant characteristics
A total of 1,691 eligible pregnant mothers were screened, of which 425 were excluded due either to declining consent or application installation failure. Of 1,266 total eligible mothers after the exclusion, 632 and 634 mothers were assigned to the intervention and control groups, respectively (Fig. 1). A total of 174 participants were lost during follow-up (14.0%). The highest rate of loss of follow-up was at the discharge interview (13.1%). Contact was lost with another four mothers who delivered by cesarean sections in the intervention group (one at the 1-month interview, three at the 6-month interview), and one in the control group (at the 6-month interview). Reasons for loss-of follow-up included declining to continue (7.8%), failure to contact due to wrong or unavailable phone numbers (5.4%), and stillbirth or neonatal death (0.5%).
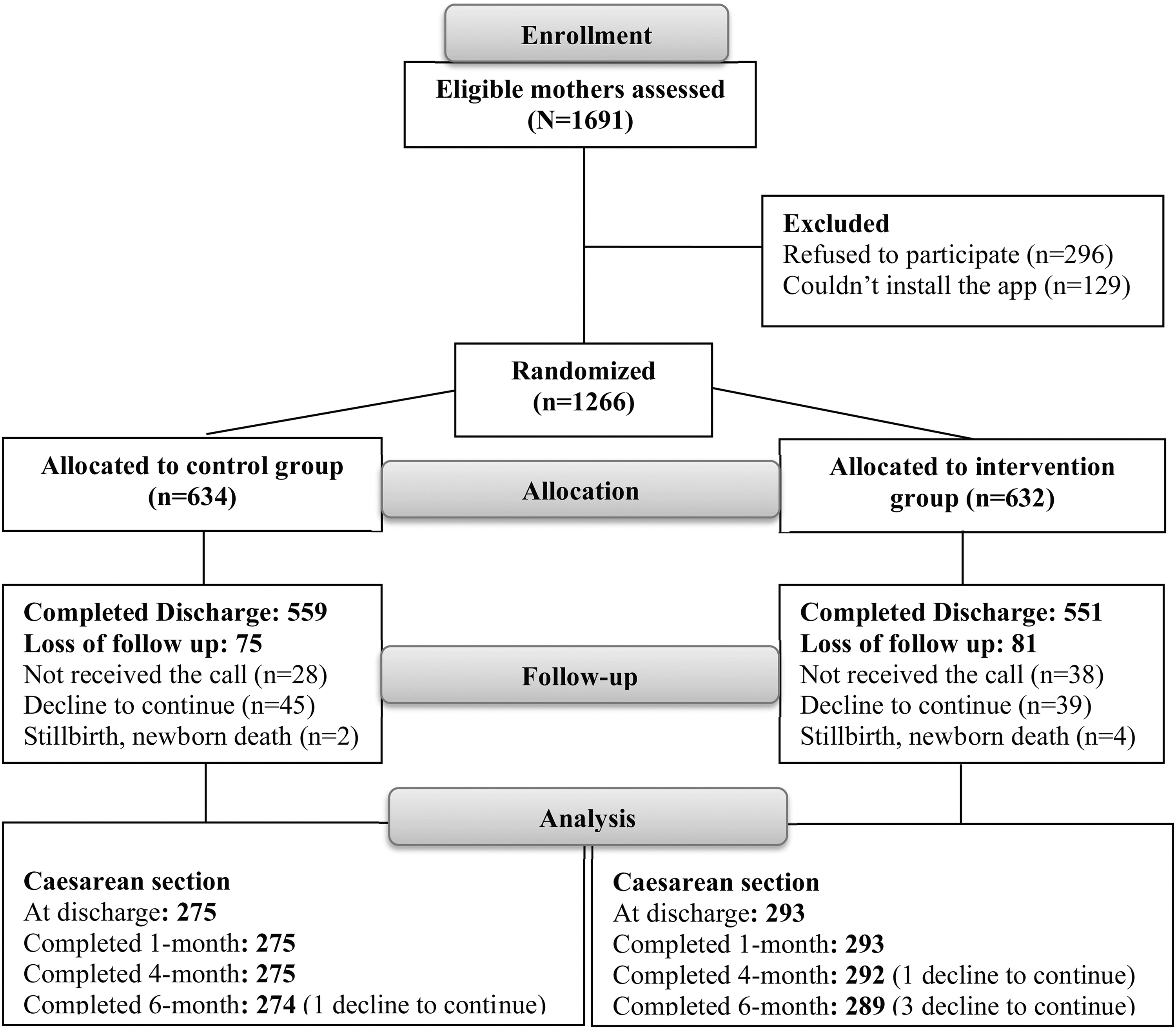
The trial flow diagram.
Concordance was calculated using percentage agreement and the kappa statistic. The percentage agreement ranged from 88.5% to 99.0%. The level of agreement for the kappa statistics was “substantial” for the child's sex and mode of delivery with respective scores of 0.76 and 0.79. It was an “almost perfect” agreement for birthweight, score at 0.87. 28 Data that were inconsistent between telephone interviews and hospital records were corrected through phone calls with the subjects.
Mothers included in the final analysis were those who completed all the interviews and answered the questions on infant feeding status. Among mothers who completed the discharge interview, cesarean section rates were 53.9% in the intervention group and 49.5% in the control group. A total of 568 mothers who underwent cesarean sections (293 in the intervention group and 275 in the control) were included in the analysis. There were no significant differences regarding maternal age, educational level, parity, prepregnancy body mass index, gestational age at the time of enrollment, and exclusive breastfeeding intention between the two groups at the discharge interview (Table 1).
Characteristics of Mothers with Cesarean Deliveries by Group Assignment at Discharge Interview (N = 568)
Based on the χ 2 test for percentages, independent samples t test for means.
BMI, body mass index; SD, standard deviation.
Breastfeeding outcomes by group assignment
During the hospital stay, the early initiation of breastfeeding rate was 29.6% in the intervention group, significantly higher than the 22.0% in the control group (Fig. 2). During the hospital stay, the exclusive breastfeeding rate in the intervention group 21.5% was significantly higher than in the control group 14.5%.

Breastfeeding rates among women who had cesarean sections at discharge, 1-, 4-, and 6-month interviews. *Statistically significant difference at p < 0.05. CI, confident interval; EBF, exclusive breastfeeding; EIB, early initiation of breastfeeding.
The exclusive breastfeeding rates in the intervention group were also higher than those in the control at 1 month (17.4% versus 12.7%), 4 months (15.1% versus 11.6%), and 6 months (6.6% versus 5.1%), respectively; however, the differences were not statistically significant.
After adjusting for maternal age, maternal education, prepregnancy body mass index, parity, gestational age at the time of enrollment, and exclusive breastfeeding intention, the multivariable logistic regression yielded similar results (Table 2). Compared with the control group, the adjusted odds ratio (aOR) of early initiation of breastfeeding (aOR = 1.50, 95% CI: 1.01–2.24) and exclusive breastfeeding during the hospital stay in the intervention group (aOR = 1.60, 95% CI: 1.03–2.48) increased significantly by 50% and 60%, respectively. Mothers in the intervention group who underwent cesarean deliveries were 1.46 times (95% CI: 0.91–2.34), 1.33 times (95% CI: 0.81–2.12), and 1.33 times (95% CI: 0.65–2.72) more likely to exclusively breastfeed their infants at 1, 4, and 6 months postpartum, respectively, compared with their counterparts in the control group. However, there were no statistically significant differences between the two groups.
Breastfeeding Outcomes Among Mothers Who Had Cesarean Sections (Intention-to-Treat Analysis n = 568)
Bold values are significant differences.
Based on the χ 2 test.
Multivariable logistic regression model adjusted for maternal age, maternal education, prepregnancy BMI, parity, maternal gestational age at enrolment, and EBF intention.
C, control group; EBF, exclusive breastfeeding; EIB, early initiation of breastfeeding; I, intervention group; OR, odds ratio of breastfeeding comparing intervention with control group.
Discussion
This study evaluated the effect of the mobile application intervention on the early initiation and exclusive breastfeeding rates among women who delivered by a cesarean section. Before the study small pool of interventions, particularly focused on parent education, had been studied to increase early initiation and exclusive breastfeeding in this population. 29 To the best of our knowledge, this was the first study to test the effect of installing a mobile application on a cellphone in this group.
Installing the mobile application, which auto-generated three messages per week and linked resources from the application's library information since the prenatal period, was a promising method for improving early initiation of breastfeeding and exclusive breastfeeding rates at discharge among mothers who had cesarean deliveries. Relevant and timely text messages were important for engaging mothers in the intervention. 30 The effectiveness of text messages through mobile phones for increasing breastfeeding outcomes among mothers, regardless of delivery type, has previously been documented across studies in low-and middle-income countries. 30 The combination of text messages and links to additional information in the application's library can further improve rates, compared with text messages alone. Our results support previous findings on the effectiveness of the simple mHealth interventions in improving breastfeeding outcomes. 31
Although there appeared to be a favorable trend in longer-term exclusive breastfeeding rates at 1, 4, and 6 months, the differences were not statistically significant, possibly due to the smaller sample size after excluding mothers who did not deliver by a cesarean section. Keeping exclusive breastfeeding high over a longer duration becomes increasingly challenging. A recent study with almost the same study design targeted low-income mothers and found a trend toward higher breastfeeding rates but not significant among mothers who already had exclusive breastfeeding intention. 32
Exclusive breastfeeding rates have multifactorial determinants, including the sociocultural and market context, settings (health systems and services, family and community, workplace, and employment level), and individual levels. 33 To improve exclusive breastfeeding rates, a comprehensive approach targeting all three levels is vital. Interventions at the structural level, including legislation, policy, media, and social mobilization to change social attitudes and practices, are key needs to be addressed. 34 Effective hospital interventions, such as the Baby-Friendly Hospital Initiative and early essential newborn care, also need to be monitored and scaled up nationwide.5,6,35
At the individual level, this randomized controlled trial provides support for the use of a mobile application, a low-cost and widely accessible intervention, starting during the antenatal period to improve the early initiation of breastfeeding and exclusive breastfeeding during the hospital stay. A previous study found that one-third of mothers underwent cesarean sections by choice in Hanoi. 36 The application, therefore, should be tailored to integrate information on reducing unnecessary cesarean sections that contribute to improving breastfeeding rates. 36 Based on our experience the application could also be tailored to be repeated in different social settings. Whereas this study was conducted in an urban area, future investigations should repeat it in other diverse areas and populations.
After delivery, lactation telehealth, a feasible and highly satisfying intervention, should be considered to increase exclusive breastfeeding rates. 37 Future research should assess how a similar intervention would be effective at improving breastfeeding rates in later stages.
Strengths and limitations
Strengths of the study include the implementation of a triple randomized controlled trial design, a mobile application development process built on behavior change theories, and careful selection of the application's features based on relevant literature. The data's quality was verified at several stages during collection. Furthermore, despite the impact of the COVID-19 pandemic's onset after the study's commencement, the follow-up rate remained acceptable, 38 at 86%, and the reasons for the loss of follow-up were similar to prepandemic phone surveys among mothers in Vietnam. 39 Despite the possible effect of attrition bias, a high follow-up rate was a key strength of the study—especially in light of challenging pandemic-related circumstances.
Some limitations should be considered concerning generalizing the results of the study. Pregnant women were enrolled at 24–36 weeks of gestation for feasibility and to adapt to the COVID-19 context. To overcome the differences in gestational age, investigators developed a set of 12 key messages that were repeated every 4 weeks. Pregnant women were anticipated to receive those key messages at least once before delivery. Gestational age at the time of enrollment was also considered a potentially associated factor and was included in the multivariate analysis. However, differences in the total length of exposure to the intervention may affect the results and are a limitation of the study. In addition to long periods of lockdown, social media was also saturated with conflicting information on infant feeding during the pandemic. 40 This may have influenced breastfeeding rates negatively as during at least one-period extensive misinformation about COVID-19 and breastfeeding was circulating across media sources.
Conclusions
This study contributes supportive evidence for the growing number of mHealth interventions for improving infant feeding. The theory-based and designed mobile application implemented in the study could also increase the early initiation and continued breastfeeding exclusivity among mothers who undergo cesarean sections.
Footnotes
Acknowledgments
We thank Dr. Nguyen Xuan Hoai and Dr. Tran Trung Chuyen for developing the technical aspects of the mobile application. Thank you also to the mothers who voluntarily participated in this study, the staff of the hospitals who willingly assisted, and the research assistants who collected the data. Thanks to Ms. Océane Parker, a Fulbright Scholar from Vanderbilt University in the United States, for her English proofreading support.
Authors' Contributions
D.T.T.D. designed the study, designed the data collection instruments, collected data, coordinated and supervised data collection, and data analysis, drafted the initial article, and reviewed and revised the article. C.B. conceptualized and designed the study, designed the data collection instruments, supervised data collection, and critically reviewed and revised the article for important intellectual content. N.M.P. designed the study, designed the data collection instruments, collected data, coordinated and supervised data collection, carried out the initial analyses, and reviewed and revised the article. A.L., Y.Z., D.T.P.H., and B.T.T.H. conceptualized and designed the study, supervised data collection, and critically reviewed the analysis and article. All authors approved the final article as submitted and agree to be accountable for all aspects of the study.
Disclosure Statement
All authors have no conflicts of interest to disclose.
Funding Information
This research was funded by a grant from the Vietnam National Foundation for Science and Technology Development (NAFOSTED) and the National Health and Medical Research Council of Australia under grant number NHMRC.108.03-2018.09. The funders had no role in the design and conduct of the study.
Key Determinants, Messages, and Library Content on Breastfeeding and Cesarean Delivery
| Key determinants | Key messages | Cesarean delivery information in the application's library content | |
|---|---|---|---|
| (1) | Believing breast milk is the best option for newborns until 6 months | Breast milk is the best choice for a newborn. | Breast milk is generated during pregnancy. You should put your baby on to your breast for feeding as soon as possible regardless of whether you had a vaginal or cesarean delivery. Within an hour after delivery is the best. |
| (2) | Breastfeeding helps your child become intelligent. | Your newborn should be put on your breast right after delivery. There is still some milk even if you don't feel it coming in or you have a cesarean delivery. | |
| (3) | Believing mothers have enough milk and can breastfeed early including those have cesarean sections | Mothers who had either vaginal or cesarean deliveries can initiate breastfeeding early. | Once you deliver your baby, your body is ready for breastfeeding and this provides the best nutrients for your baby. Delivery by cesarean section versus a vaginal delivery does not affect the milk-production process. Both mothers who have vaginal or cesarean delivery can put a newborn on the breast right after delivery. |
| (4) | Mothers who had either vaginal or cesarean delivery can produce enough breast milk for the baby. | Mothers who deliver by cesarean section can start breastfeeding early and exclusively. They may have some difficulties, but those can be overcome. Vaginal delivery is the best for both mother and the newborn's health. Only 10–15% of mother's have difficulties in delivery that requires delivery through cesarean section. |
|
| (5) | Planning to breastfeed exclusively | The earlier you breastfeed your baby, the sooner your milk comes in. | Your newborn needs to be breastfed within an hour after delivery, whether you have a vaginal or cesarean section. Ask your health providers to help with putting your child on the breast right after delivery. |
| (6) | The earlier breastfeeding the better, either you have vaginal or cesarean delivery. | If you have had a cesarean section, you can still put your child on your breast right after delivery or right after being awake. Talk to your health care providers for support with skin-to-skin contact and early initiation of breastfeeding, myths and truths about cesarean and breastfeeding, and benefits of early initiation of breastfeeding for mothers who have cesarean section. | |
| (7) | Do not feed your newborn any liquid or food except breast milk. | A newborn only needs breast milk to be full, even if there is very little. Ask your health care providers to help you with breastfeeding as soon as possible, whether you have vaginal or cesarean delivery. | |
| (8) | Involving the husband and family members in preparing for exclusive breastfeeding | The more father takes care of the baby, the more he can love him/her. | Talk with your husband about the mode of delivery. Vaginal delivery is the best for the mother's and child's health. How can your husband support breastfeeding if you have cesarean delivery? |