
Abstract
Introduction:
Given the known relationships between breastfeeding and hypertension, and between hypertension and stroke, we examined the association between breastfeeding a child and stroke later in life. We hypothesized a history of breastfeeding is associated with lower prevalence of stroke.
Methods:
Our study population included parous females 20 years and older. Potential confounders included family income-to-poverty ratio, education, smoking status, parity, and age at first live birth. Potential effect measure modifiers included race/ethnicity and age at survey. Multivariable logistic regression models were used to estimate crude and adjusted prevalence odds ratios (ORs) and 95% confidence intervals (CIs) for the association between breastfeeding and stroke.
Results:
The odds of stroke among those who ever breastfed were lower than those who never breastfed (OR = 0.68, 95% CI: 0.55–0.86; p < 0.01). Adjusting for education decreased the strength of the association (OR = 0.80, 95% CI: 0.63–1.01; p = 0.06). In analyses stratified by age, the inverse association between breastfeeding status was significant among those ages 20–64 years (OR = 0.69, 95% CI: 0.47–1.00) but not among those 65 years and older (OR = 0.99, 95% CI: 0.73–1.34).
Conclusions:
Ever breastfeeding a child was associated with lower prevalence of stroke in a nationally representative U.S. sample of parous females 20 years and older. Results were strongest among those <65 years old.
Introduction
Stroke is the third leading cause of death for women in the United States, killing twice as many women as does breast cancer (51.4 versus 25.4 deaths per 100,000 females in 2019). 1 For females ages 55–75, the lifetime risk of stroke is one in five. 2 The risk of stroke increases with age, and, as women on average live longer than men, their risk is increased. Additionally, due to social and economic disadvantages rooted in discrimination, the risk of stroke is unequal across racial and ethnic groups in the United States, with Black populations having a higher incidence of stroke than white populations. Compounding this disparity, the incidence of ischemic stroke is declining in white populations but has remained stable in Black populations. 3
There is a known biological relationship between hypertension and stroke and between breastfeeding and hypertension. Hypertension causes stroke through a variety of mechanisms. High blood pressure increases stress on blood vessel endothelium, leading to increased permeability and vessel damage. This can induce thrombi formation, which can embolize to the brain. Additionally, hypertension can accelerate the atherosclerotic process within cerebral vasculature, increasing the likelihood of ischemic stroke. 4 Although exact mechanisms have not been elucidated, breastfeeding a child has been associated with a decreased prevalence of hypertension, with those who breastfeed more children or for a longer duration having lower odds of hypertension compared with those who breastfeed fewer children or for a shorter duration. 5 Breastfeeding has also been associated with a lower prevalence of hyperlipidemia and diabetes, 6 both of which increase stroke risk. 7
To our knowledge, two prior studies have shown an association between breastfeeding and reduced risk of stroke. The first study examined a cohort of women 30–79 years of age in China, where breastfeeding practices may be more common than in the United States. 8 The second study examined a cohort in the United States but only included postmenopausal women. 9 The purpose of this study is to evaluate whether a causal association exists between a history of breastfeeding and stroke later in life among parous females 20 years of age or older in the United States. We hypothesized that there is an inverse association between breastfeeding and stroke, evidenced by a decreased prevalence of stroke in individuals who have a history of ever breastfeeding a child compared with those who have never breastfed any children. We hypothesize this association will be stronger in those ages 65 years and older than in those younger than 65, given the increased incidence of stroke later in life. 10 We also hypothesize the association will be stronger among Black women due to increased stroke incidence among this population. 11
Materials and Methods
Participants
We used publicly available data from the U.S. National Health and Nutrition Examination Survey (NHANES) to perform the analysis. NHANES is a set of nationally representative cross-sectional surveys collected on 2-year cycles by the National Center for Health Statistics. 12 Approximately 5,000 participants are surveyed annually and are nationally representative of the U.S. population that is noninstitutionalized, which excludes individuals in, “…correctional facilities, nursing and skilled nursing facilities, inpatient hospice facilities, mental health or psychiatric hospitals, and group homes and residential treatment centers for juveniles.” 13 The focus of the surveys changes slightly over time to address specific groups or meet emerging needs. Interview questionnaires include information on demographics, diet, social concerns, and medical conditions and are completed in the home or at the NHANES Mobile Examination Center using a computer-assisted personal interviewing system.
Our cross-sectional analysis included questions from the NHANES Demographics, Reproductive Health, Smoking—Cigarette/Tobacco Use—Adult, Medical Conditions, and Blood Pressure and Cholesterol questionnaires from seven NHANES survey cycles (1999–2012). The use of publicly available deidentified NHANES data published by the National Center for Health Statistics did not require Institutional Review Board approval. Our study population included NHANES participants who identified their gender (per NHANES wording) as female, were ages 20 years or older (the ages questioned by NHANES for breastfeeding history), and with a history of at least one live birth. Exclusion criteria included missing data for breastfeeding or stroke history. Participants who had a stroke before age at last live birth were also excluded, in an attempt to remove strokes that occurred before breastfeeding exposure.
Measures
Exposure
Breastfeeding history was asked on the Reproductive Health questionnaire in slightly different forms from 1999 to 2012. From 1999 to 2006, participants who identified themselves as female were asked if they breastfed any of their children. From 2007 to 2012, participants who identified themselves as female were asked if they breastfed any of their children for at least one month. Data across these cycles were combined with responses divided into categories of never versus ever breastfed, with never breastfeeding serving as the referent group.
Outcome
Stroke history was consistently asked to participants 20 years of age or older on the Medical Conditions questionnaire from 1999 to 2012 through the question, “Has a doctor or other health professional ever told you that you had a stroke?” The variable was categorized as never versus ever having a stroke. Self-reported stroke has been found to be a valid proxy for stroke diagnosis in other datasets.14–16
Covariates
Potential confounders were identified based on literature review and NHANES data availability and included family income-to-poverty ratio (PIR), education, parity, smoking status, and age at first live birth. PIR was obtained from the Demographics questionnaire and categorized as below (PIR <1) or at or above (PIR ≥1) the federal poverty line. Education was measured across five categories (<9th Grade, 9–11th Grade, High School Graduate/general educational development, Some College or Associate in Arts degree, and College Graduate or above). Smoking status was categorized as smoking less than or greater than 99 cigarettes in their lifetime. Parity was obtained from the Reproductive Health questionnaire, which inquired about the number of deliveries resulting in a live birth and categorized as 1, 2, 3, or 4+ live births. Age at first live birth was utilized as a continuous variable. Due to a skip pattern in the questionnaire that reported age at first live birth under the question for age at last live birth in those with just one live birth, these data were combined to create a new continuous age at first live birth variable.
Potential effect measure modifiers of interest included race/ethnicity and age. Participants self-reported race/ethnicity with the options of Mexican American, Other Hispanic, Non-Hispanic white, non-Hispanic Black, and other. Due to changes in NHANES design sampling by race and Hispanic origin in 2007, effect measure modification analysis was limited to non-Hispanic white and non-Hispanic Black participants. Age at the time of survey was categorized into less than or greater than/equal to 65 years of age.
Hypertension was considered a potential mediator of interest. Hypertension history was self-reported on the Blood Pressure and Cholesterol questionnaire, which asks if a health care professional has ever told a participant they have hypertension or high blood pressure. Self-reported hypertension has previously been found to be a valid proxy for hypertension in NHANES. 17
Analytic sample
The analytic sample included an original total of 71,916 individuals (Fig. 1). From this, males (n = 35,441) and nonparous females (n = 22,782) were excluded. Next, individuals who had a stroke at an earlier age than their age at their last live birth were excluded (n = 43). Finally, individuals with missing data for either breastfeeding or stroke were removed (n = 500). This resulted in a final analytic sample of 13,150 individuals.
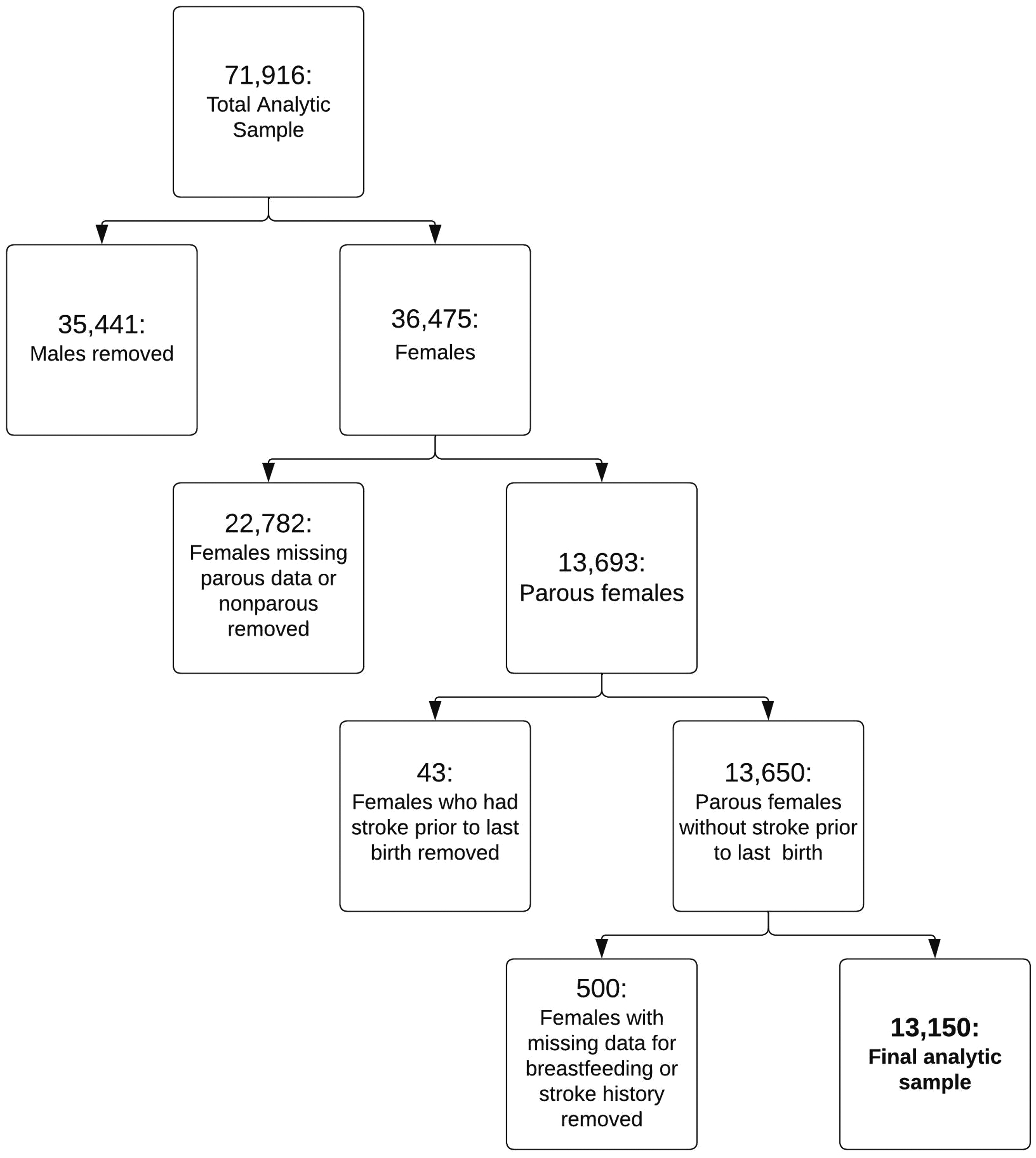
Analytic sample creation for parous females ≥20 years old from National Health and Nutrition Examination Survey 1999 to 2012.
Statistical analyses
Statistical analyses were conducted using Stata version 16.1. Sampling weights were constructed according to NHANES Analytic Guidelines for combining the utilized survey cycles to account for complex survey design. 18 Descriptive analyses were conducted to compare the distribution of covariates in those ever breastfed versus never breastfed. Covariates with >10% missing data across the analytic sample were excluded from further analyses. The distribution of covariates was also examined among individuals with missing breastfeeding or stroke history to determine the similarity of excluded participants to the analytic sample. Multivariable logistic regression models were used to estimate the crude and adjusted prevalence odds ratios (ORs) and 95% confidence intervals (CIs) for the association between breastfeeding and stroke.
Confounding assessment was performed using a selection approach. 19 Confounders that produced the greatest change in the OR for the association between breastfeeding and stroke were sequentially retained in the model until no additions resulted in at least a 10% change in the OR. The crude and final adjusted models were then stratified by age at the time of survey, as well as race/ethnicity. Cross-product interaction terms were created by multiplying the breastfeeding and age at the time of survey or race/ethnicity variables. These terms were individually included in both crude and adjusted models and partial F tests were used to test significance (α = 0.10) of the interaction term for both variables.
Potential mediation through history of hypertension was assessed by including hypertension history in the final adjusted model and calculating the percent change in OR between breastfeeding and stroke.
Results
History of stroke is not distributed evenly across those who ever versus never breastfed (Table 1). There is a higher percentage of individuals with stroke in those who never breastfed (4.0%) compared with those who ever breastfed (2.8%). Participants who had and had not breastfed were similar regarding family PIR, parity, and age at first live birth. However, differences between the exposed and unexposed groups are apparent in categories of education, race/ethnicity, smoking status, and hypertension. Participants who ever breast fed proportionally more often attended some college or had a college degree, or were Mexican American, but were less often non-Hispanic Black or had smoked, compared with those who never breast fed. Lastly there was a higher prevalence of hypertension in those who never breastfed.
Characteristics of Parous Females ≥20 Years Old from National Health and Nutrition Examination Survey 1999 to 2012, by Breastfeeding Status
Italics were used to distinguish missing counts from non-missing counts.
CI, confidence interval; GED, general educational development; SE, standard error.
Assessment of the distribution of covariates among NHANES participants excluded from the analytic samples suggests that those excluded due to lack of breastfeeding data were proportionally more likely to be below the federal poverty line, have had only one live birth, be Mexican American, be missing smoking data, or be younger than those included in the study, but less likely to have a history of hypertension. Those missing stroke also had a lower age at first live birth compared with those included in the study (Supplementary Table S1).
Table 2 shows the results of the crude and adjusted models. The odds of stroke among those who ever breastfed were 0.68 (95% CI: 0.55–0.86) times the odds among those who never breastfed. This indicates that those who breastfed had 32% lower odds of stroke than those who never breastfed. Education was the only covariate that met confounding criteria. Adjusting for education decreased the strength of the association (OR = 0.80, 95% CI: 0.63–1.01). The direction of the association in both models was weakly inverse. The crude model was statistically significant (p < 0.01) but the adjusted model was not (p = 0.06).
Odds Ratios of Stroke According to Breastfeeding Status Among Parous Females ≥20 Years Old
Adjusted for education.
CI, confidence interval; OR, odds ratio.
Table 3 shows the crude and adjusted models stratified by age and race/ethnicity. In those <65 years old, the odds of stroke among those who breastfed were 0.69 (95% CI: 0.47–1.00) times the odds of those who never breastfed, while the odds were 0.99 (95% CI: 0.73–1.34) in those ≥65 years old. The OR for those <65 years old is consistent with a weak inverse association between breastfeeding history and stroke prevalence, while the OR for those age 65 years and older is consistent with a null association between breastfeeding history and stroke prevalence. The interaction term for age was statistically significant in the crude model (p = 0.02) but not in the adjusted model (p = 0.10). When the analytic sample was stratified by race/ethnicity, in non-Hispanic Black females, the OR of stroke among those who breastfed were 0.60 (95% CI: 0.40–0.90) times the odds of those who never breastfed, while in non-Hispanic white females, the odds were 0.96 (95% CI: 0.72–1.27).
Stratified Odds Ratios of Stroke According to Breastfeeding Status Among Parous Females ≥20 Years Old
Adjusted for education.
CI, confidence interval; OR, odds ratio.
The OR for non-Hispanic Black females is consistent with a moderate inverse association between breastfeeding history and stroke prevalence, while the OR among non-Hispanic white females is consistent with a null association between breastfeeding history and stroke prevalence. However, interaction term for race/ethnicity was not statistically significant in the crude (p = 0.59) or adjusted models (p = 0.25).
Finally, we assessed the extent to which hypertension mediated the association between breastfeeding and stroke. Adding self-reported history of hypertension to the fully adjusted model attenuated the association by 9.2% (OR = 0.87, 95% CI: 0.69–1.10) and thus did not meet the criterion for meaningful mediation.
Discussion
The results of this study support our hypothesis of an inverse association between ever breastfeeding a child and prevalence of stroke in a nationally representative sample of parous females age 20 and older. Contrary to our hypothesis, when results were stratified by age, we found a stronger inverse association in those <65 years old compared with those 65 years old and older, although significant effect measure modification by age was only found in the crude and not the adjusted model. Furthermore, we did not find evidence to support our hypothesis of significant effect measure modification by race/ethnicity.
The present findings of an inverse association between ever breastfeeding and stroke are consistent with the limited previous research on this association in different populations. A prospective study of parous women in China found a hazard ratio for stroke of 0.92 (95% CI: 0.85–0.99) in those who ever breastfed compared with those who never breastfed, 8 while Jacobson et al. found an adjusted hazard ratio of 0.77 (95% CI: 0.70–0.83) using data from postmenopausal women in the Women's Health Initiative Observational Study. 9 However, Jacobson et al. differed in their findings regarding significant differences in the association by race/ethnicity, which contrasts with our nonsignificant effect measure modifier findings for race/ethnicity. This difference may be a result of the smaller sample size in the present study or the fact that our analysis was limited to only two race/ethnicity categories. Given that any differences by race/ethnicity are socially instead of biologically driven, 20 the lack of findings could also be explained by overadjustment due to inclusion of other socially driven covariates such as education.
On the other hand, the lack of findings could also represent a novel finding that supports a suspected lack of underlying biological difference in the mechanism linking breastfeeding and stroke between socially defined races. Finally, our results demonstrate potential effect measure modification of the association between breastfeeding and stroke by age. This observation is consistent with prior research, which found that the inverse associations of breastfeeding with cardiovascular disease occurrence became weaker with increasing age. 6
A biological mechanism explaining our results is supported by numerous findings linking breastfeeding to a lower risk of hypertension.21,22 However, the present study did not observe strong evidence that hypertension mediates the association between breastfeeding and stroke, suggesting other biological mechanisms may be at play in the observed protective association. Furthermore, the increased magnitude of association for those <65 years of age suggests that breastfeeding may exert a protective effect against stroke by means of more acute mediating factors than hypertension. One hypothesis is that the increases in prolactin and oxytocin that accompany breastfeeding could inhibit blood clotting and thus decrease the risk of stroke in the postpartum period, which could explain the stronger inverse association between breastfeeding and stroke in younger individuals. 23
If a history of breastfeeding is associated with lower prevalence of stroke, then encouraging and supporting breastfeeding can be a novel public health strategy to reduce stroke incidence. As stroke is a leading cause of death for women in the United States, risk reduction through encouragement of breastfeeding during the pregnancy and postpartum period, when individuals often have more contact with the health care system, could have a large public health impact. Furthermore, establishing a wider spectrum of protective effects from breastfeeding could encourage needed reform of both legislation and social norms to better support all individuals who wish to breastfeed.
Limitations
The largest limitation to our results is that the NHANES survey collects cross-sectional data. While we attempted to establish temporality using available data, mainly by removing any strokes that occurred before a person's last live birth, this proxy does not definitively tell us the stroke occurred after breastfeeding. Additionally, other covariates such as socioeconomic status were collected at the time of the survey and are not necessarily the same as at the time of the exposure. We expect that this limitation results in our observed association being underestimated, as socioeconomic status is more likely to increase with age.
Other limitations stem from stroke being a rare outcome. Combining seven NHANES cycles only resulted in about 500 strokes in our analytic sample. Due to these low numbers, we chose to only look at non-Hispanic Black and non-Hispanic white individuals for our race/ethnicity effect measure modification, as these categories had sufficiently large populations to analyze. This limits the ability to generalize these findings to any other racial or ethnic subpopulations represented in NHANES surveys. Prior literature has also examined the number of children breastfed as an effect measure modifier and dose–response indicator. This question was only asked in four of the seven NHANES cycles we compiled, and therefore did not provide sufficient numbers for analysis.
Our inability to examine number of children breastfed limits the support we can provide for the protective effect of breastfeeding found, although we hypothesize that the strength of the association would increase with increasing number of children breastfed. Additionally, NHANES only asks questions about pregnancy and breastfeeding to individuals who select female in response to their gender and, therefore, these data do not enable us to assess the association between breastfeeding and stroke in persons who do not identify as female.
An additional limitation is the differential distribution of certain covariates among those excluded due to missing breastfeeding or stroke data compared with those included in the study. In particular, excluded NHANES participants tended to be younger, and, given the present findings that suggest the association is stronger in the younger population, exclusion of more of these individuals may have biased the association toward the null. Additionally, those excluded were less likely to have hypertension and, given that hypertension is a strong risk factor for stroke, this also may have biased the association toward the null. Furthermore, those excluded for lack of breastfeeding data had a lower stroke prevalence compared with those included, and those excluded for lack of stroke data had lower prevalence of ever breastfeeding. Thus, it is possible that exclusion of these participants reduced the number of individuals who never breastfed and have not had strokes, biasing the present findings away from the null.
Finally, there is potential for survival bias when examining stroke prevalence as an outcome given that an estimated 10–20% of strokes result in death, 24 which would preclude inclusion in NHANES surveying. Given that stroke fatalities are reportedly decreasing more in populations <65 years of age than in populations 65 years of age and older, 25 survival bias may more significantly impact the association in the older age group, which could explain the null findings in our stratified analysis. However, we do not suspect stroke fatalities to vary according to breastfeeding status and, thus, this may not be a significant source of bias.
Generalizability
These results, based on data that are nationally representative of the U.S. population that is not institutionalized, are generalizable to parous individuals who self-identify as female and are ages 20 years and older. They suggest that ever breastfeeding has a protective effect against stroke as compared with never breastfeeding, particularly in younger females (under age 65 years). These results do not suggest there is any difference in the strength of association between non-Hispanic Black and non-Hispanic white populations, although these results are more limited due to smaller sample sizes. Furthermore, these results are not generalizable to other racial/ethnic groups or individuals who breastfeed and do not self-identify as female. Additionally, the fact that the distribution of several covariates differed in the 500 participants excluded due to missing breastfeeding or stroke data compared with those included in the study suggests that these results may not be as applicable to individuals below the federal poverty line, Mexican American females, and those who have only had one live birth.
Conclusions
In a nationally representative sample of parous females ages 20 years and older, those who had ever breastfed compared with those who had never breastfed had 20% lower odds of a stroke. This association was stronger in those under age 65 than in those 65 years and older, and stronger among non-Hispanic Black females than non-Hispanic white females. Interaction terms for these stratifications with the final adjusted model were not statistically significant, nor was the mediation by hypertension on the association between breastfeeding and stroke. Further research could elaborate upon the mechanism of the observed protective action of breastfeeding against stroke and whether this protection persists throughout the life course. Overall, our results are consistent with a small body of literature, which suggests that breastfeeding is protective against stroke. This suggests that campaigns to reduce stroke among parous populations could focus on promoting breastfeeding to prevent future cerebrovascular accidents.
Footnotes
Acknowledgments
The authors gratefully acknowledge the feedback from our epidemiology classmates, who helped critique this work in its early development stages, as well as our MD-MPH program directors, Drs. Stull and Foster. Additionally, they are grateful to the NHANES participants, without whom this work would not be possible.
Authors' Contributions
G.M.R. and E.M.: Conceptualization (equal); data curation (equal); methodology (equal); software (equal); writing—original draft (equal); writing—review and editing (equal). K.S.: Methodology (supporting); supervision (supporting); writing—review and editing (equal). L.R.K.: Conceptualization (supporting); supervision (supporting); writing—review and editing (supporting). L.M.M.: Methodology (supporting); supervision (lead); writing—review and editing (supporting).
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Dr. Kair's effort was supported by a Building Interdisciplinary Research Careers in Women's Health award (K12 HD051958, PI Nancy Lane, MD) funded by the National Institute of Child Health and Human Development, Office of Research on Women's Health, Office of Dietary Supplements, and the National Institute of Aging. Dr. Kair's effort was also supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1 TR001860. The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health. The other authors have no funding to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.