
Abstract
Background:
Newborns hospitalized in the neonatal intensive care unit are exposed to an average of 10 painful procedures per day. The pain-related experiences of babies can be associated with neurodevelopmental disorders that may affect them throughout their lives.
Aim/Objective:
The purpose of this study was to summarize and analyze the analgesic effects of breastfeeding alone, expressed breast milk, and breast milk smell on newborns and present stronger evidence that would guide clinical practice and future studies.
Methods:
We searched articles published between 2000 and 2021 on the CINAHL, Cochrane Central, Web of Science, PubMed, Scopus, Science Direct, Eric, and OVID databases. Nine full texts that met the inclusion criteria (Population: Newborn term or preterm babies, Intervention: Implementing breastfeeding, expressed breast milk, breast milk taste, or breast milk smell alone or in combinations in the intervention groups, Comparison: Making comparisons to the standard care of the clinic where the study was conducted, Outcomes: Including at least one pain-related criterion, Study design: Randomized-controlled trials) were included in this systematic review and meta-analysis. The nine randomized controlled studies in total that were included in this study were carried out between 2004 and 2021 with 33–130 newborns in their samples. The total number of newborns was 720. The effects of these interventions on pain scale scores, heart rate, and oxygen saturation were also analyzed.
Results:
According to the results of this systematic review and meta-analysis, the breastfeeding, breast milk smell, or breast milk taste interventions had large effect sizes in terms of pain management during and after the procedures. These interventions had medium effect sizes in terms of heart rate during the procedures and large effect sizes after the procedures. In terms of oxygen saturation, they had large effect sizes during the procedures and medium effect sizes after the procedures.
Conclusion:
Breastfeeding and breast milk interventions are significantly effective nonpharmacological alternatives for painful procedures.
Introduction
Pain is defined as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage.”1,2 Any person with the ability to speak can express the pain. However, the assessment of pain in babies is a highly complex process for health care professionals. 3 Studies conducted on pain in babies, who cannot verbally express their pain, have assisted the development of various scales that enabled the objective assessment of pain.1–3 Currently, there are several pain scales for the clinical assessment of pain in newborns. Recent technological improvements, fundamental and clinical studies, and an increase in the awareness of pain problems in all age groups have led to improvements in the assessment, reduction, and prevention of pain.4,5 Pharmacological and nonpharmacological methods have been shown to be effective in reducing pain in newborns.5,6 Various nonpharmacological techniques can be beneficial in reducing pain and pain-related anxiety when they are used alone or in combination with other methods.7–9
The expression of pain varies greatly depending on the cognitive development level of babies. Therefore, pain may be considered a complex and multidimensional experience with sensory, emotional, cognitive, and interpersonal components. 10 Whereas the cardiovascular effects of pain include increased heart rate, higher blood pressure, and more oxygen consumption, physiological situations such as crying and the responses of the extremities to pain may also occur.11,12 Prevention and alleviation of pain in neonates, especially preterm ones, is important not only because it is ethical, but also because of the known short- and long-term effects of repeated exposure to painful stimuli on the development of undesirable neurodevelopmental sequelae.10,13,14 The pain experience of babies can show differences even when they are exposed to the stimulus causing the same form of pain at another time. Thus, pain management techniques should be used as much as possible before any painful interventions. 13
The description of breast milk, which has had anthropological significance throughout history, as “white gold” is an indicator of how important breast milk is for the baby. 15 From an evolutional perspective, breast milk is not only a biological norm that is used to feed the baby, but studies have also shown in time that it strengthens maternal attachment, and breast milk may be used as an intervention to reduce the procedural pain by breastfeeding, dripping it into the mouth of the baby or being given to the baby to smell.3,15 It is known that breast milk and its smell release chemosensory substances that can regulate the behavioral responses of babies. 15 It has been stated that especially the behavior of the baby turning toward the mother's breast, who has the ability to suck milk right after birth, is caused by the chemosensory properties of breast milk.3,15
Furthermore, many randomized controlled trials (RCTs) have discussed the analgesic effects of breast milk and its smell on newborns during painful procedures and compared their results with other alternatives (e.g., amniotic fluid smell, mother's smell, and sucrose).7–9,11,12,16 However, to the best of our knowledge, there is no systematic review and meta-analysis study in the literature that has examined outcomes related to breastfeeding alone, expressed milk, and breast milk smell in helping to reduce the procedural pain in newborns.
Therefore, the purpose of this study was to summarize and analyze the analgesic effects of breastfeeding alone, expressed milk, and breast milk smell on newborns and present evidence that would guide clinical practice and future studies.
Methods
Aim
This systematic review and meta-analysis study, including RCTs only, was carried out to investigate the effects of interventions performed with breastfeeding or breast milk on pain in newborns (term and preterm).
The research questions were:
How do interventions perform with breastfeeding or breast milk affect pain in newborns?
How has breast milk been used to reduce pain in newborns?
What kinds of procedures have previous studies used in interventions with breastfeeding or breast milk to reduce pain in newborns?
What were the variables that have been used by previous studies to investigate pain in newborns?
Design
In this systematic review and meta-analysis study, the procedure of the Cochrane Handbook for Systematic Reviews of Interventions version 6.017 was followed, and the results were reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement 18 (Fig. 1).
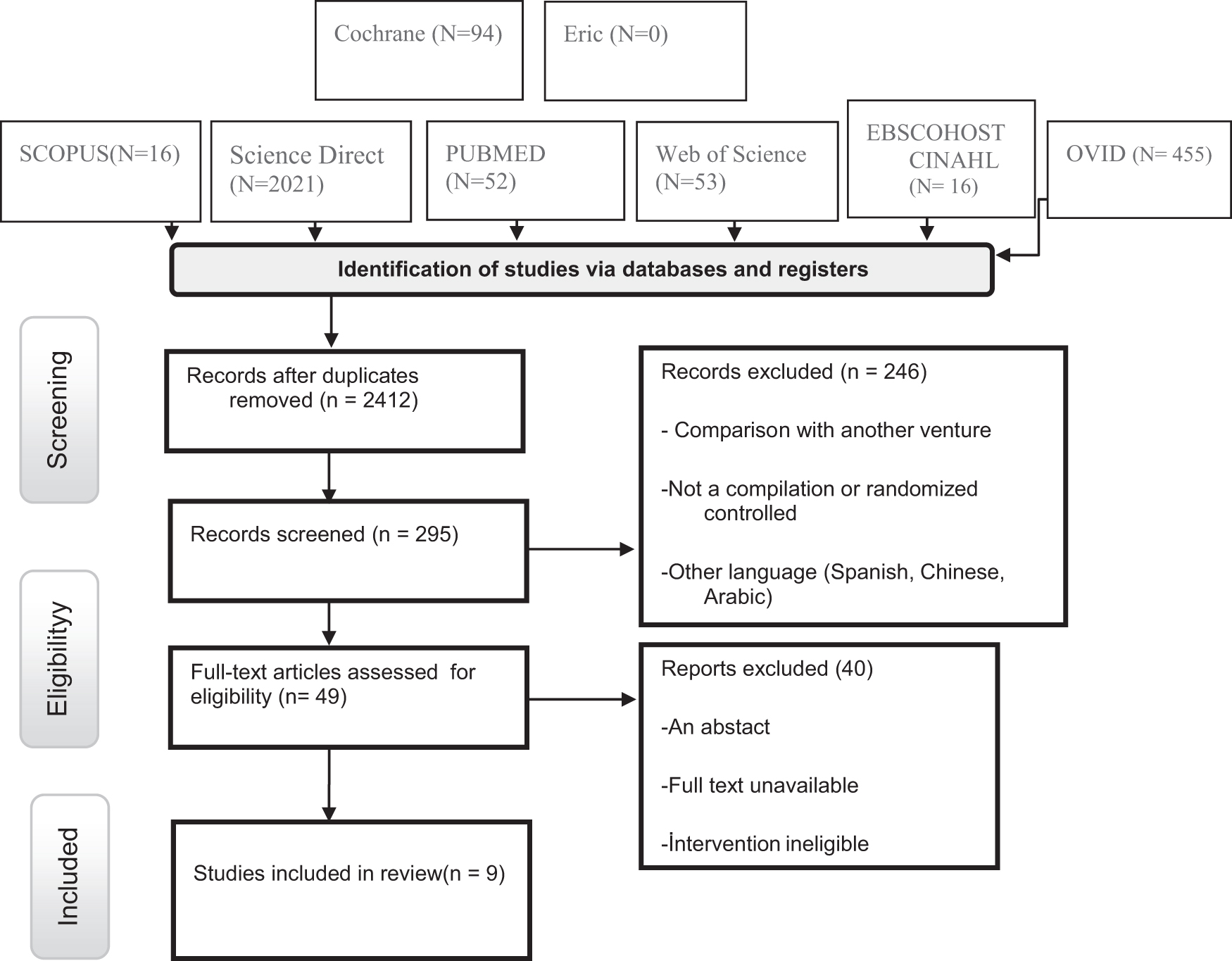
Flow diagram of study retention process for the meta-analysis and systematic review.
Search methods
Articles published in English between 2000 and 2021 were searched on the CINAHL, Cochrane Central, Web of Science, PubMed, Scopus, Science Direct, Eric, and OVID databases. Combinations created with keywords in the Medical Subject Headings and those in previous articles were used as the search terms. To understand whether the searched studies met the inclusion criteria of this study, their titles and abstracts were examined before their full texts. In contrast, studies with suitable titles and abstracts whose full texts could not be accessed were excluded. Publications were included in this study based on the population–intervention–comparison–outcomes–study design criteria. 19
Inclusion criteria
Population: Newborn term or preterm babies.
Intervention: Implementing breastfeeding, expressed breast milk, breast milk taste, or breast milk smell alone or in combinations in the intervention group.
Comparison: Making comparisons with the standard care of the clinic where the study was conducted.
Outcomes: Including at least one pain-related criterion.
Study design: RCTs.
Exclusion criteria
Studies comparing breastfeeding and breast milk-related interventions with other interventions, those with no outcomes related to pain, those that were not RCTs, those that were not performed with newborn babies, and those that were in the conference abstract, review, or editorial form were excluded.
Search results
At first, duplicate studies, then, studies with unsuitable titles and/or abstracts were removed during the search. Finally, considering that a study with an effect size >14 as a result of analyses could be misleading in the results of the systematic review and meta-analysis, such studies were removed. Nine full texts that met the inclusion criteria were included in this study (Fig. 1).
Risk of bias and quality appraisal
The assessment of the bias in these nine studies was independently performed by two researchers based on the Cochrane Collaboration's tool for assessing the risk of bias in randomized trials. This tool allows researchers to evaluate randomized trials using 12 criteria. Each criterion was scored as low, unclear, or high in this study. The evaluations of the two researchers were discussed and combined afterward. In the case of a disagreement, discussions were carried out regarding the relevant criterion until a mutual decision has been reached. 17
Data extraction and synthesis
Two researchers independently extracted the data of the studies that met the inclusion criteria and recorded them on the standard form created for the groups. The data recorded on the form included information on the first author, year of publication, country, number of participants (intervention/control), procedures regarding breastfeeding or other practices, measures, and outcomes. Studies to be included should have assessed pain as the main variable. Besides the pain, variables such as heart rate and oxygen saturation were also extracted and included in the analysis. Studies that did not use a scale to measure pain and those that did not report mean and standard deviation values were excluded.
The data of this study were analyzed using the Review Manager 5.3 and State 16.0 programs. If the measurements in the included studies were repeated at different times, the latest measurement was taken into account. Pre- and postprocedural pain levels were evaluated as the main data in this meta-analysis. Pre- and postprocedural heart rate and oxygen saturation data were also evaluated. The duration of crying, which we considered to be included initially, was excluded from the analysis since this variable was examined in only three studies. Two researchers extracted the data together by using the Microsoft Office Excel program. Cohen's d was used to calculate the effect size of the study. The effect size was interpreted as small if it was 0.2, medium if 0.5, and large if 0.8. 20 Cochran's Q statistic about the heterogeneity of included studies, in other words, whether the studies show the same effect (χ 2 , p < 0.10), can be assessed based on tau, H2, or I2. In this study, heterogeneity was assessed based on I2, whereas other statistics were also calculated.
The random effects model was used when the I2 statistics were >0.50, and the fixed effects model was used when the I2 statistics were <0.50. Publication bias was determined by utilizing funnel plots and Begg's and Egger's tests. The random effects model with the DerSimonian and Laird method was considered in the meta-analysis.21–24
Results
The characteristics of the included studies and information about the used interventions are presented in Table 1. These nine included studies were carried out between 2004 and 2021 with their samples ranging from 33 to 130 newborns.25–27 The total number of newborns was 720. Among the included studies, three were conducted in Iran, two were conducted in India, and the rest were conducted in Canada, Turkey, France, and China. Four studies were carried out with preterm newborns.25,28,29
Study Characteristics of Included Studies (Breastfeeding and Breast Milk Interventions)
BMO, breast milk odor; DAN, Douleur Aiguë du Nouveau-né; DW, distilled water; EBM, expressed breast milk; EBMS, embracing breast milk sucking; HBV, hepatitis B vaccine; MBMO, maternal breast milk odor; NFCS, neonatal facial coding system; NIPS, Neonatal Infant Pain Scale; PIPP, premature ınfant pain profile; ROP, retinopathy of prematurity.
Whereas expressed breast milk (EBM) was used as the intervention in two of the studies,25,26 breast milk smell was used in three studies,25,28 and breastfeeding was used in the remaining four studies.26,27,30,31 In two of the studies that included breast milk smell, the intervention was carried out by pouring 2 mL of breast milk from the baby's mother or another mother on a cotton swab. 28 In the other study, a diffuser was placed under a hood with an airflow rate of 6 L/min, manually switched on 3 minutes before a venipuncture procedure, and switched off 9 minutes after the completion of the procedure. 25
The babies were breastfed by their mothers 5 minutes before, during, and 5 minutes after the procedure in two of the studies with the breastfeeding intervention.30,31 In one of the other studies with the breastfeeding intervention, the intervention group babies were breastfed for 2 minutes before, during, and 2 minutes after the procedure. 26 In the other breastfeeding study, no information was given about the duration of the intervention. 27 In one of the studies where EBM was the intervention, the babies in the intervention group were given 2 mL of EBM orally with a paladai (a small cup traditionally used to feed newborns in India) 2 minutes before the procedure along with standard practice. 29 In the other study, 2 minutes before venipuncture, the babies in the intervention group were given 5 mL of EBM, whereas those in the control group were given 5 mL of distilled water as a placebo. 32
Risk of bias in the included studies
The bias risk assessment results of the included studies are given in Figures 2 and 3. The randomization method used was not explained in only one study; therefore, this study was assessed as unclear. 27 In all other studies, the methods of randomization used by the authors were explained, and these studies were accordingly marked as low risk. There were concerns about allocation concealment in three studies, which had to be marked unclear.27,30,31 All remaining studies were marked as low risk. In the examinations of blinding (performance bias and detection bias), it was determined that four studies had a high risk since they could not apply the blinding.26,27,30,31

Risk of bias graph.

Risk of bias table.
It is seen that the risk of bias in especially the studies with double-blinding was low. The studies that used single-blinding had better values in bias scoring compared with those that did not provide any information about blinding. Since the blinding (performance bias and detection bias) was not explained appropriately in three of the included studies, they were marked as low risk.25,26,29 There was no information provided regarding the blinding of participants and personnel or randomization in the study conducted by Wu et al, which was rated as high risk. Blinding of outcome assessment (detection bias) was marked as high risk in three of the included studies where there was no blinding in the data collection and analysis phases.27,30,31
Results
Outcomes
As seen in Table 2, when the I2 statistics were not <0.50, the studies did not show the same effect. In this case, it was seen that there were random effects, and the random effects model with the DerSimonian and Laird method was taken as a basis. It is known that the fixed effects model is more suitable to use when the I2 statistics are <0.05. The Cochran's Q test in this study revealed a high level of heterogeneity in the nine studies included in the analysis.
Homogeneity Tests for Intervention and Control Groups
SPO2, oxygen saturation.
Table 3 shows the results of the rank correlation test (Begg's test) and linear regression test (Egger's test) that were performed to determine publication bias. Accordingly, there was no small-study effect.
Begg and Egger Test Results
SPO2, oxygen saturation.
Pain scores during and after the procedure
Nine studies in total that used breastfeeding or breast milk interventions to reduce the pain in newborns were included in this systematic review and meta-analysis study. However, not all studies provided all applicable data. Some studies measured pain during the procedure, whereas some measured it after the procedure. As the pain measurement method, the Premature Infant Pain Profile was used in four studies,25,28,29 the Neonatal Infant Pain Scale was used in two studies.27,30 the Neonatal Facial Coding System was used in two studies,31,32 and the Douleur Aiguë du Nouveau-né scale was used in one study. 26 The upper limits of the 95% confidence interval (CI) for Cohen's d for the pain values during the procedure in six of the included studies and the pain values after the procedure in seven of the included studies were calculated, respectively, as −2.06 and −1.95 based on the data obtained with the random effects model. As a result, the interventions were determined to have favorable effects in the groups they were used, and the “pain” values were generally lower in these groups (z = −3.66, p = 0.000; z = −4.16, p = 0.000) (Figs. 4 and 5).
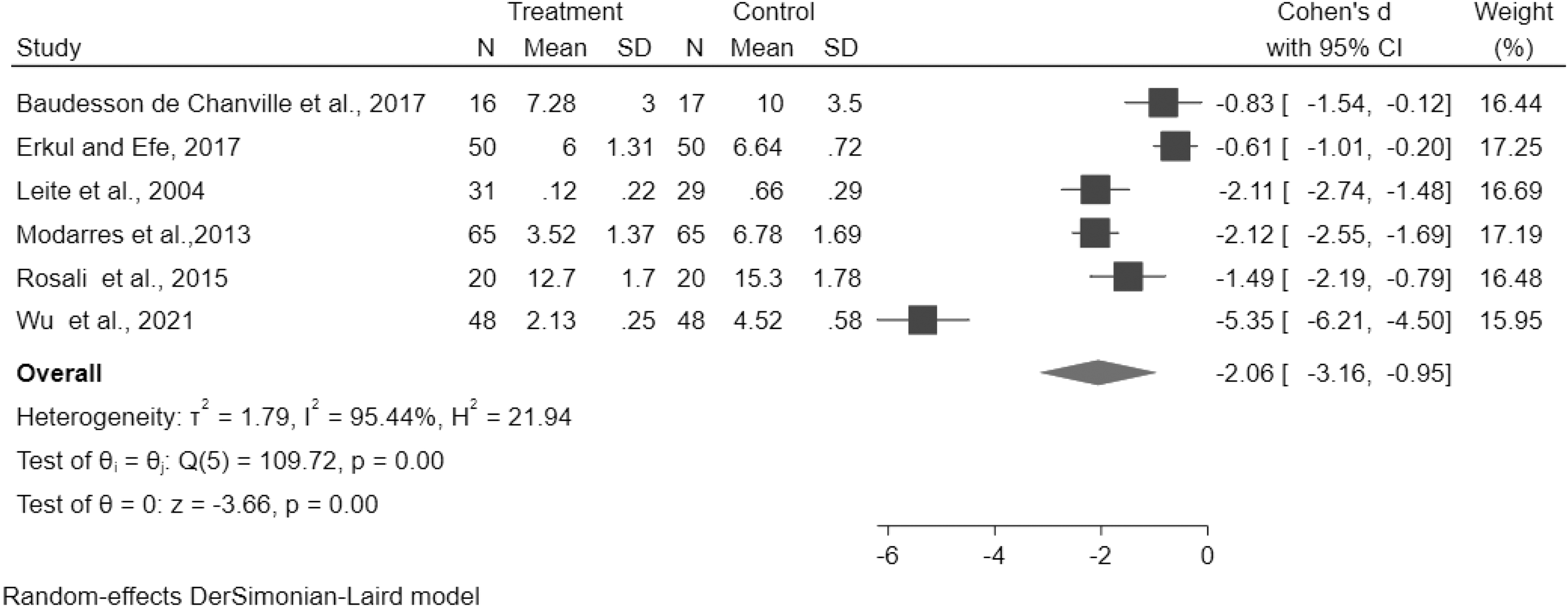
Forest plot showing the effects of breastfeeding or breast milk versus routine care on pain scale scores during the procedures.

Forest plot showing the effects of breastfeeding or breast milk versus routine care on pain scale scores after the procedures.
Physiological stability
Heart rate
The upper limits of the 95% CI for Cohen's d for the heart rate values during the procedure in four of the included studies and the heart rate values after the procedure in five of the included studies were calculated, respectively, as −1.62 and −0.53 based on the data obtained with the random effects model. Consequently, although there was no sufficient evidence that the intervention had a favorable effect on the intervention group during the procedure, it was found to have a favorable effect after the procedure (z = −1.84, p = 0.07; z = −4.91, p = 0.000) (Figs. 6 and 7).
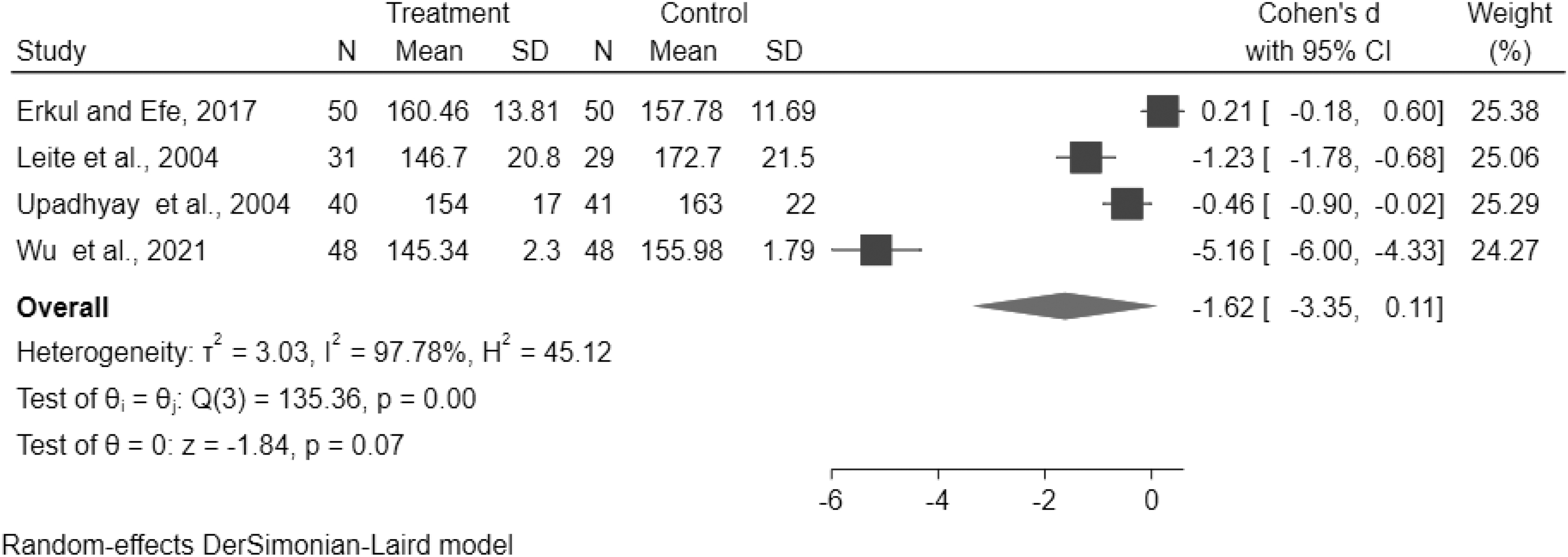
Forest plot showing the effects of breastfeeding or breast milk versus routine care on heart rate during the procedures.
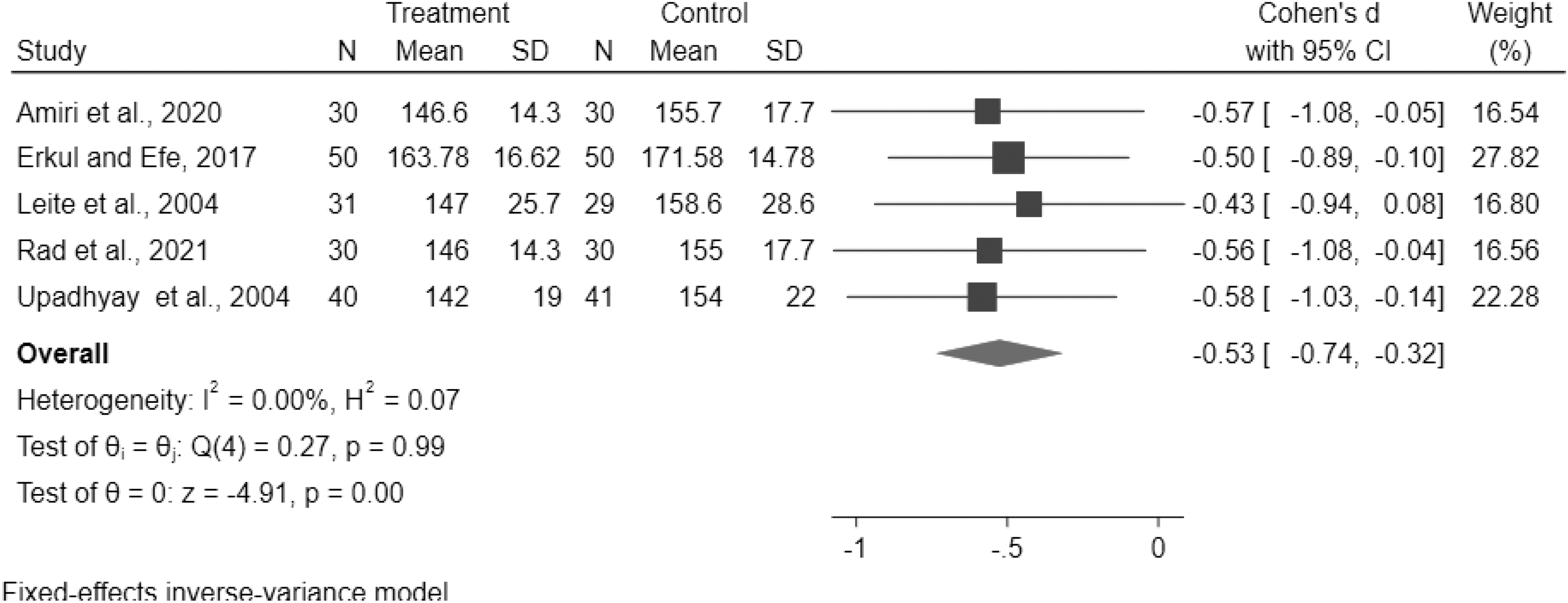
Forest plot showing the effects of breastfeeding or breast milk versus routine care on heart rate after the procedures.
Oxygen saturation
The upper limit of the 95% CI for Cohen's d for the oxygen saturation values during the procedure in three of the included studies was calculated as 1.46 based on the data obtained with the random effects model. Moreover, the upper limit of the 95% CI for Cohen's d for the oxygen saturation values after the procedure in four of the included studies was calculated as 0.55 based on the data obtained with the fixed effects model. As a result, the intervention was determined to have a favorable effect on the intervention group, and the “SpO2” values of the intervention group were generally higher (z = −1.59, p = 0.01; z = −4.68, p = 0.000) (Figs. 8 and 9).

Forest plot showing the effects of breastfeeding or breast milk versus routine care on oxygen saturation during the procedures.

Forest plot showing the effects of breastfeeding or breast milk versus routine care on oxygen saturation after the procedures.
Discussion
To the best of our knowledge, this systematic review and meta-analysis study is the first study that investigated the effects of breastfeeding and breast milk interventions on pain in newborns together. Besides the effects of these interventions on pain scale scores, their effects on heart rate and oxygen saturation were also analyzed. According to the results of this systematic review and meta-analysis, the breastfeeding, breast milk smell, or breast milk taste interventions had large effect sizes in terms of pain management during and after the procedures. These interventions had medium effect sizes in terms of heart rate during the procedures and large effect sizes after the procedures. In terms of oxygen saturation, they had large effect sizes during the procedures and medium effect sizes after the procedures.
Babies in the neonatal intensive care unit are exposed to an average of 10 painful procedures per day. The fact that newborns have more pain receptors in comparison with adults leads them to have a lower pain threshold and a lower pain tolerance level.33–35 The pain-related experiences of babies can be associated with neurodevelopmental disorders that may affect them throughout their lives. The American Academy of Pediatrics highlighted the necessity of pharmacological or nonpharmacological methods in the monitoring and management of procedural pain in newborns.36–39 In this study, studies on the effectiveness of breastfeeding, breast milk smell, and breast milk taste, which are among nonpharmacological alternatives, were examined.
In pain management, structures in the brain stem are known to regulate sensory stimuli in the gate control theory. If the baby is exposed to enough sensory stimuli, the brain stem can close the gate and prevent the entry of painful stimuli. 40 Therefore, the negative effects of pain on babies can be prevented by subjecting them to positive haptic, auditory, olfactory, or taste stimuli. Breastfeeding and breast milk can be used in pain management (ameliorates, modifies, and reduces the reaction to painful stimuli) because they are both inexpensive and easily accessible.
Another meta-analysis study examined only the effectiveness of breast milk smell, and the authors reported that breast milk smell did not show a significant improvement in the physiological parameters of newborns compared with amniotic fluid smell and the mother's smell. 41 It was suggested that newborns show highly variable attraction responses to certain maternal bodily fluids, and these human-specific cues can be embedded in not only fluids in the colostrum and fluids produced by the Montgomery glands but also other bodily secretions. 3 These results indicate that exposure to the smell of breast milk and the smell of the mother during breastfeeding could have the same effect.
According to the results of meta-analyses on breastfeeding, similar to our study results, breastfeeding has been found to be significantly effective in improving behavioral parameters and lowering pain scores.3,42,43 Although Harrison et al 44 reported in their meta-analysis study that breastfeeding did not have a consistent effect on heart rate and oxygen saturation values, breastfeeding was determined to be effective on physiological parameters in a Cochrane systematic review on breastfeeding about procedural pain in newborns. 43 In our study, breastfeeding and breast milk interventions were determined to be also effective on heart rate and oxygen saturation values.
Conclusion
Breastfeeding ameliorates, modifies, and reduces the reaction to painful stimuli. In addition to the extraordinary benefit of breast milk in infant feeding, breastfeeding and breast milk interventions are important nonpharmacological alternatives for painful interventions. Therefore, as shown in other studies, we recommend the use of breast milk interventions in painful procedures.
Footnotes
Authors' Contributions
Z.Ç. and Ç.E. performed the searches and wrote the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.