
Abstract
Objective:
To study breastfeeding initiation, duration, and associated factors in patients with systemic lupus erythematosus (SLE), a cross-sectional study comparing with SLE and non-SLE mothers was conducted.
Methods:
Thirty patients with SLE who had pregnancy outcomes from September 2018 to December 2020 and 120 non-SLE patients (excluding mothers with other immune system diseases) were included in the study. Data on sociodemographic, obstetric, and SLE clinical information were collected. Breastfeeding initiation, breastfeeding duration, and reasons for not initiating breastfeeding were investigated via telephone.
Results:
The rate in breastfeeding of SLE group was significantly lower than non-SLE group (36.7% versus 86.7%, respectively, p < 0.001; odds ratio 0.059; 95% confidence interval 0.015–0.241). Non-SLE mothers had a longer duration of breastfeeding than mothers with SLE (log-rank p = 0.001). Fearing of the adverse effects of drugs on babies is the main reason (68.4%) for not initiating breastfeeding in SLE group. Infants with high weight and Apgar scores, primipara women, and having a college degree were significantly associated with breastfeeding among patients with SLE.
Conclusion:
SLE women showed a lower breastfeeding rate and shorter breastfeeding duration. Postpartum medications are safe for lactation in most patients with SLE. Targeted intervention programs that enhance breastfeeding consultations are required for this group.
Introduction
Systemic lupus erythematosus (SLE) is a systemic autoimmune disease that primarily affects women of childbearing age. 1 With the improvement in SLE diagnosis and treatment ability, an increasing number of women with SLE are facing fertility problems. Due to changes in hormone levels, patients with SLE may have a recurrence or aggravation of the disease during pregnancy. Meanwhile, the incidence of premature delivery, fetal growth retardation, and preeclampsia in pregnant women with SLE is high, which endanger the safety of the fetus and pregnant women. 2
Therefore, an increasing number of studies have focused on the management of pregnancy in SLE patients. However, little attention has been paid to postpartum breastfeeding of SLE patients. Reports on breastfeeding in patients with SLE are rare, with small studies performed in Argentina, the United States, and Italy,3–5 and only a few patients are included. No reports of Chinese population on breastfeeding of SLE patients have been seen so far.
In this study, we aimed to investigate the initiation and duration of postpartum breastfeeding in Chinese SLE patients, identify common reasons for not breastfeeding, and analyze relevant influencing factors, to provide evidence for promoting postpartum breastfeeding in patients with SLE.
Methods
Study design
A cross-sectional study comparing mothers with SLE and non-SLE was conducted in a large teaching hospital located in Xuzhou, in the central part of China. Patients with SLE who had singleton pregnancy outcome from September 2018 to December 2020 were incorporated in the study. All of them met the 2012 Systemic Lupus International Collaborating Clinics criteria for SLE. 6 Patients with early or middle pregnancy termination, aged younger than 18 years, diagnosed with mental illness, or unwilling to cooperate with telephone follow-up were excluded from this study. In this study, 45 pregnant women with SLE were identified, 3 patients had early and second trimester abortion or iatrogenic termination of pregnancy, 11 patients could not be contacted during telephone follow-up investigation, and 1 eligible patient rejected participation.
Finally, 30 SLE women met the criteria and agreed to participate in the survey. According to the principle of 1:4, 120 non-SLE pregnant women who give birth at the same time with SLE women were included, excluding mothers with other immune system disease. This study was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University.
Study factors
Clinical data were extracted from the electronic medical record system, including age of the pregnant woman (at delivery), education level, parity, gestational age of delivery, perinatal complications (including gestational diabetes, preeclampsia, postpartum hemorrhage, premature rupture of membrane, thyroid dysfunction, intrahepatic cholestasis of pregnancy, premature delivery, fetal growth retardation, and oligohydramnios), delivery mode, whether the mother was admitted to intensive care unit (ICU), newborn weight, newborn sex, Apgar scores, whether admitted to neonatal intensive care unit (NICU), the course of SLE, and postpartum anti-SLE drugs. Breastfeeding initiation, breastfeeding duration, and reasons for not initiating breastfeeding were investigated by telephone. Based on postpartum lactation, those who were either exclusively breastfeeding or breastfeeding and supplementing with formula were classified as “breastfeeding.”
Statistical analysis
Descriptive statistics were used for the general analysis. Continuous variables were expressed as averages ± standard deviation of the mean or medians (md), defined by Shapiro–Wilk normality test. Categorical variables were described by absolute frequencies (n) and percent (%). Student's t tests were applied to compare means, Mann–Whitney tests to compare medians as appropriate. Categorical variables were analyzed by means of either chi-square or the Fisher's exact test as applicable. Univariate and multivariate logistic regression analysis of breastfeeding between SLE and non-SLE mothers was performed. Effect estimates are reported along with odds ratio (OR) value, confidence interval (95% CI), and p-value. With the purpose of exploring survival curves for two groups, Kaplan–Meier curves and the log-rank test were utilized. A p < 0.05 was deemed statistically significant in the two-tailed test. SPSS software (version 23.0) and GraphPad 8.0 were used for the statistical analysis.
Results
Sociodemographic and obstetric characteristics of SLE and non-SLE mothers were described (Table 1). There was a statistical difference in maternal age (p = 0.012) and maternal education level (p = 0.003) between two groups. SLE group was more likely to have preterm birth than non-SLE group (30.0% versus 13.3%, p = 0.028). The number of primiparas in SLE mothers were more than non-SLE mothers (76.7% versus 49.2%, p = 0.007).
Sociodemographic and Obstetric Characteristics of Systemic Lupus Erythematosus and Nonsystemic Lupus Erythematosus Mothers
ICU, intensive care unit; NICU, neonatal intensive care unit; SLE, systemic lupus erythematosus.
SLE group showed lower neonatal weight (2,685 [2,125–3077.5] versus 3,255 [2,925–3,560], p < 0.001) and Apgar scores (8.00 [7.50–9.00] versus 9.00 [8.00–9.00] at 1 minute, p = 0.002; 9.00 [8.75–10.00] versus 10.00 [9.00–10.00] at 5 minutes, p < 0.001). The newborns of SLE group were more likely admitted to NICU (36.7% versus 16.7%, p = 0.016). Both groups were similar regarding mode of delivery, maternal admitted to ICU, sex of newborns, perinatal complications.
Median SLE duration was 4.00 (2.75–9.25) years, with minimum and maximum duration being 1 month and 20 years, respectively. Hydroxychloroquine (HCQ) was taken postpartum by 86.7% of SLE mothers, while glucocorticoid by 96.7%. Thirty percent of the SLE mothers took immunosuppressants, including azathioprine (n = 1), cyclosporine (n = 3), mycophenolate mofetil (n = 3), leflunomide (n = 1), and tacrolimus (n = 1).
The rate of breastfeeding of SLE group was significantly lower than non-SLE group ([11/30, 36.7%] versus [104/120, 86.7%], respectively, p < 0.001; OR 0.089; 95% CI 0.036–0.221). Even after adjusting for multiple confounders, breastfeeding rates were significantly lower in SLE women than non-SLE women (p < 0.001; OR 0.059; 95% CI 0.015–0.241) (Table 2). Non-SLE mothers showed longer duration of breastfeeding than SLE mothers (log-rank p = 0.001) (Fig. 1). The rate of breastfeeding <3 months in SLE group was higher than non-SLE group ([5/11, 45.5%] versus [0/104, 0%], p < 0.001), conversely, the rate of breastfeeding >12 months in SLE group was significantly lower ([3/11, 27.3%] versus [61/104, 58.7%], p < 0.001).
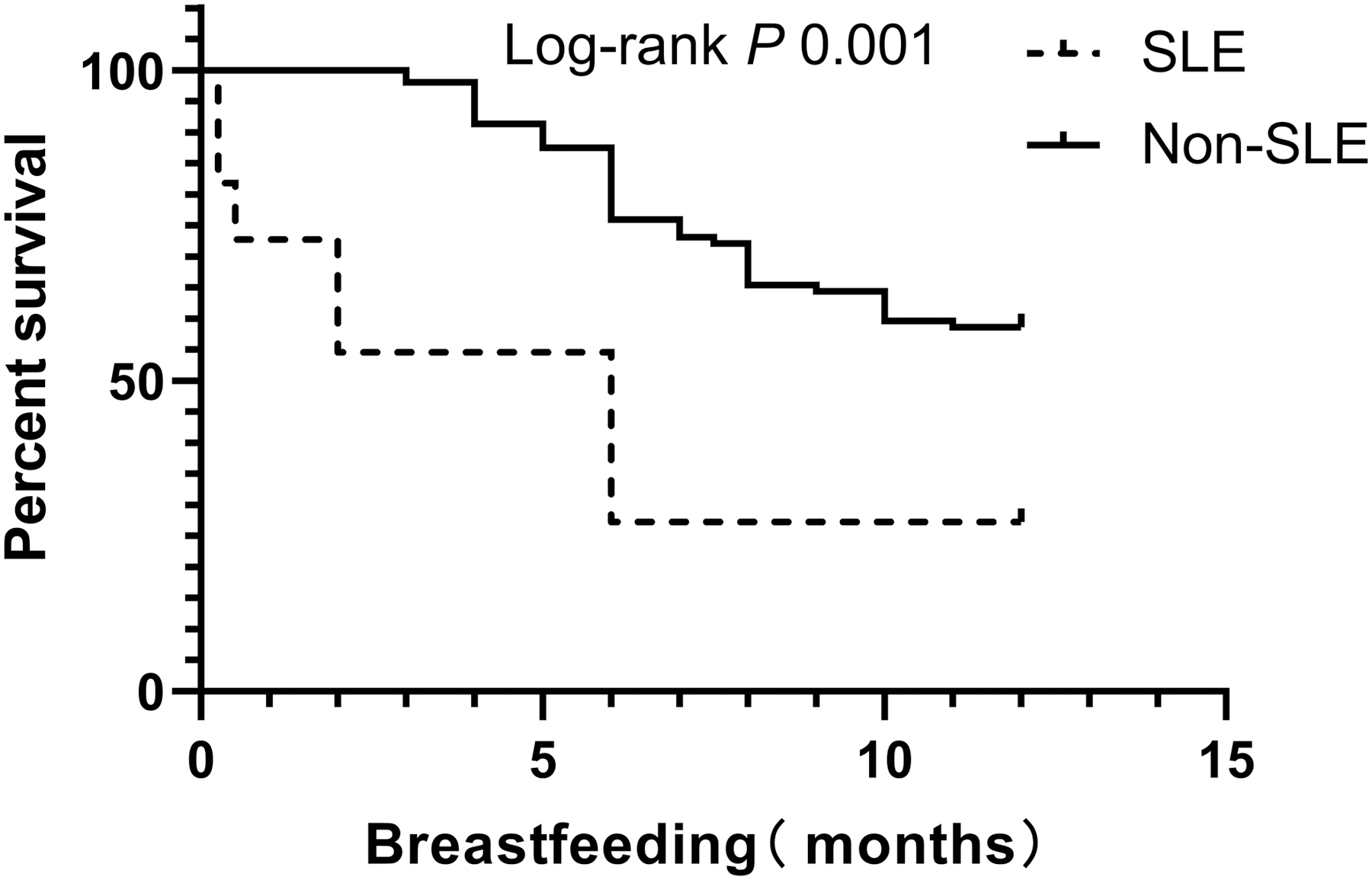
Kaplan–Meier curves of breastfeeding in patients with SLE and non-SLE. SLE, systemic lupus erythematosus.
Univariate and Multivariate Logistics Analysis of Breastfeeding Between Systemic Lupus Erythematosus and Nonsystemic Lupus Erythematosus Mothers
Model 1: univariate logistic analysis.
Model 2: adjusted maternal age and maternal education level.
Model 3: adjusted maternal age, maternal education level and parity.
Model 4: adjusted maternal age, maternal education level, parity, gestational weeks, neonatal weight, Apgar scores and NICU stay.
CI, confidence interval; NICU, neonatal intensive care unit; OR, odds ratio.
The main reason (13/19, 68.4%) for not initiating breastfeeding in SLE group was the concern about the adverse effects of drugs on infants. Two (2/19, 10.5%) feared that breastfeeding would lead to flare of the disease, two (2/19, 10.5%) because of doctors' recommendation of formula feeding, one (1/19, 5.3%) because of insufficient breast milk supply, and one (1/19, 5.3%) refused night breastfeeding.
Data about the comparison between breastfeeding and nonbreastfeeding women in SLE group were summarized (Table 3). Women with a college degree breastfed more frequently (21.1% versus 78.9%, p = 0.047). Infants with higher weight (2,940 [2,530–3,130] versus 2,180 [1,910–2,740], p = 0.027) and higher Apgar scores at 1 and 5 minutes (9 [8–9] versus 8 [6–8] at 1 minute, p = 0.003; 10 [9–10] versus 9 [7–9] at 5 minutes, p = 0.003) were more likely to be breastfed. Multiparas were less likely to breastfeed than primiparas (0% versus 100%, p = 0.029). Maternal age, gestational weeks, delivery mode, whether the mother was admitted to ICU, perinatal complications, sex of newborns, duration of SLE, and whether going to NICU did not statistically affect the initiation of breastfeeding.
Sociodemographic Profile and Factors Influencing Infant Feeding Modality in Systemic Lupus Erythematosus Group
Immunosuppressants include azathioprine, mycophenolate mofetil, leflunomide, cyclosporine, and tacrolimus.
ICU, intensive care unit; NICU, neonatal intensive care unit; SLE, systemic lupus erythematosus.
Discussion
SLE combined with pregnancy is considered high-risk due to potential maternal and fetal complications, such as preterm birth, intrauterine growth restriction, and preeclampsia. In view of this, an increasing number of studies focus on the management of SLE during pregnancy, improving the success rate of SLE patients' pregnancy and reducing maternal and infant mortality. However, much less data are available about postpartum period and the attention paid to breastfeeding is insufficient. In 2016, Acevedo conducted a cross-sectional study, including 36 SLE patients and 36 non-SLE patients, found that the rate of not initiating breastfeeding in SLE patients was higher than that in non-SLE patients (19.5% versus 5.6%, p = 0.07), SLE mothers had a shorter breastfeeding period (6 months) than non-SLE mothers (12 months). 3
In the same year, a study from the United States included 51 SLE patients and half of the SLE patients (n = 25, 49%) chose breastfeeding. 4 In 2020, a study included 57 pregnancies in 43 SLE women showed that 41 (71.9%) choose breastfeeding and the median time of breastfeeding was 3 months. 5
In our study, 30 SLE and 120 non-SLE mothers were included. The rate of breastfeeding of SLE group was significantly lower than non-SLE group (36.7% versus 86.7%, respectively, p < 0.001; OR 0.059; 95% CI 0.015–0.241), which was a lower breastfeeding initiation than the above three studies from Argentina, the United States, and Italy. Duration of breastfeeding in non-SLE mothers is much longer than SLE mothers. The rate of breastfeeding <3 months in SLE group was higher than non-SLE group (45.5% versus 0%, p < 0.001), conversely, the rate of breastfeeding >12 months in SLE group was significantly lower (27.3% versus 58.7%, p = 0.010). The SLE mothers taking immunosuppressors had a trend of not breastfeeding (22.2% versus 77.8%, p = 0.419), but there was no statistical significance in our study, which is different from Noviani's research. 4 This may be related to the small sample size of our study.
We found that the main reason of not breastfeeding in patients with SLE was the concern about the side effects of anti-SLE drugs on babies. In this study, the most common drugs in SLE group who did not breastfeed were HCQ (HCQ, n = 15) and glucocorticoid (n = 18), while a small number of patients used cyclosporine (n = 2), mycophenolate mofetil (n = 3), leflunomide (n = 1), and azathioprine (n = 1). Glucocorticoids, including prednisone, methylprednisolone, and prednisolone, are the most common drugs for the treatment of rheumatoid immune diseases. Two studies have showed that even doses of 1 gram of IV methylprednisolone are not likely to affect the infant.7,8 HCQ is the background drug in SLE patients. 9 Concentrations of HCQ secreted through milk are <1%, 10 which supports the compatibility of HCQ with breastfeeding.11,12
Newborns exposed to azathioprine are theoretically at risk of bone marrow suppression. However, a study involving 10 women who had used azathioprine while breastfeeding found azathioprine and its metabolites were not detected in the blood of 10 nursing infants and there were no clinical or hematological signs of immunosuppression, 13 which was confirmed in another study. 14 Therefore, guideline from European League Against Rheumatism (EULAR), as well as the British Society of Rheumatology (BSR) and British Health Professionals in Rheumatology (BHPR) guideline, pointed out that azathioprine can be used during lactation.11,12 A few reports described that cyclosporine could be excreted through milk, however, serum cyclosporine levels in breastfed infants were undetectable.15–17 Therefore, women should not be prevented from breastfeeding while taking cyclosporine.11,12
At present, there are no data on the excretion of leflunomide into milk and only a little information exists on mycophenolate mofetil, 18 so these two are not recommended for use during lactation. 19 In this survey, the dose or equivalent dose of prednisone did not exceed 20 mg/day. Many of the postpartum medications were safe for lactation, except for four patients who were treated with leflunomide and mycophenolate mofetil.
This study has the following limitations. It is retrospective, so the recollections of SLE patients and non-SLE mothers may be inaccurate. However, this may influence both groups similarly. Another limitation is that this study investigated only whether patients breastfed or not, did not subdivide exclusive breastfeeding and mixed breastfeeding. Meanwhile, as the sample size of this study is small, we could not perform multivariate analysis of factors influencing breastfeeding in SLE group. Besides, this study did not address the effects of disease phenotypes and disease activity on breastfeeding, which we planned to discuss in future prospective studies. Even so, it is the first report on breastfeeding of patients with SLE in China, as far as we know.
In summary, the rate of breastfeeding in SLE mothers was significantly lower than that in non-SLE mothers, and the duration of breastfeeding was shorter. Through further inquiry, we found that concern about the potential effects of drugs on fetus was the main reason for not starting breastfeeding. To improve the breastfeeding status in SLE, risk assessment of lactation medication and breastfeeding consultation are needed for this group.
Footnotes
Acknowledgments
We thank all colleagues assisting in this investigation. The authors also express their appreciation to the women who participated in this study for giving so generously of their time and effort to provide clinical information.
Authors' Contributions
All authors contributed to this article. W.L. conceived and designed the study. T.W. analyzed the data. W.L. and T.W. drafted the article. All authors approved the final article as submitted.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.