
Abstract
Background:
While breast milk is widely accepted as the best source of nutrients for almost all newborns, breastfeeding can be especially challenging for preterm and low birth weight (LBW) infants. With increased risk of admission to neonatal intensive care units (NICUs) and separation from parents, this population experiences significant barriers to successful breastfeeding. Thus, it is crucial to identify interventions that can optimize breastfeeding for preterm and LBW infants that is continued from birth and admission, through to hospital discharge and beyond.
Objectives:
To identify and analyze evidence-based interventions that promote any and exclusive breastfeeding among preterm and LBW neonates at discharge and/or postdischarge from hospital.
Methods:
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist. Searches were performed in the following databases: MEDLINE Ovid, EMBASE, Web of Science, and Cumulative Index to Nursing and Allied Health (CINAHL).
Results:
From the 42 studies included, 6 groups of intervention types were identified: educational and breastfeeding support programs, early discharge, oral stimulation, artificial teats and cups, kangaroo mother care (KMC), and supportive policies within NICUs. All groupings of interventions were associated with significantly increased rates of any breastfeeding at discharge. All types of interventions except artificial teats/cups and oral stimulation showed statistically significant increases in exclusive breastfeeding at discharge. KMC demonstrated the highest increased odds of breastfeeding at discharge among preterm and LBW infants.
Conclusions:
A variety of effective interventions exist to promote breastfeeding among hospitalized preterm and LBW infants. Hospital settings hold unique opportunities for successful breastfeeding promotion.
PROSPERO registration: CRD42021252610
Introduction
Globally, an estimated 15 million infants are born preterm (before 37 weeks gestation) and 20.5 million infants are born with a birthweight of less than 2,500 g (low birth weight [LBW]), both of which are associated with increased risk of neonatal death and acute and long-term adverse health consequences.1,2 Breast milk is widely accepted as the best source of nutrients for newborns, including preterm and LBW infants, where appropriate nutrition is critical for their health and development. Preterm infants provided with human breast milk are at reduced risk of necrotizing enterocolitis and sepsis, have reduced risk of hospitalization and length of hospital stay, as well as improved mental and psychomotor development, bone health, and long-term cardiovascular outcomes.3,4
To support physical and neurological development, breast milk from mothers who delivered preterm infants contains more protein and bioactive components than milk from mothers who delivered term infants. 3 Therefore, provisioning mother's own breast milk directly or expressed, is recommended as the first choice for feeding preterm and LBW infants.4,5
However, promoting human milk and breastfeeding among preterm and LBW infants can be challenging. Breastfeeding rates are consistently lower in comparison to term infants. For example, data from the United States have shown that rates of breastfeeding among preterm infants ranged from 63.8% to 71.3%, while breastfeeding rates among term infants are 76.5% to 84.6%.6,7 Increased rates of health complications experienced by preterm infants, immature oromotor skills, and suckling abilities, their admission into intensive or high-dependency care and thus a separation from their parents, as well as parental stress, create significant barriers to successful breastfeeding among preterm and LBW infants. 8
Thus, it is important to implement interventions aimed at optimizing breastfeeding for preterm and LBW infants. However, while there are numerous reviews focused on breastfeeding interventions among term infants,9–12 there is a current gap in the literature reviewing breastfeeding interventions in preterm and/or LBW infants. Reviews on breastfeeding interventions have also often focused on interventions that improved breastfeeding initiation but do not evaluate breastfeeding at hospital discharge.13,14 Although improving breastfeeding initiation is crucial, breastfeeding initiation does not guarantee continuation. Successful initiation of breastfeeding does not completely mitigate the challenges and barriers that mothers continue to experience throughout their infants' hospitalization and beyond. Therefore, it is important to identify interventions that improve breastfeeding rates at discharge and follow-up. The purpose of this review is to identify and analyze evidence-based interventions that promote any and exclusive breastfeeding among preterm and LBW infants at discharge and/or postdischarge from hospital.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist 15 (Supplementary Table S1). The review protocol was developed and registered on PROSPERO (CRD42021252610).
Inclusion and exclusion criteria
Studies were included if the study population comprised preterm (gestational age <37 weeks) and/or LBW infants (birth weight <2,500 g) (Table 1). Studies that only described infants admitted to the neonatal intensive care unit (NICU) without identifying and/or separately analyzing outcomes for preterm or LBW infants or studies comprising only term infants were excluded. This review included studies that examined the effectiveness of interventions that aimed to promote breastfeeding (direct or expressed milk feeding). Our outcomes of interest include breastfeeding rates at discharge (any and exclusive breastfeeding), breastfeeding rates at 3 months postdischarge (any), and breastfeeding rates at 6 months postdischarge (any). Studies that did not report at least one of these outcomes were excluded. All study designs were included. Studies without primary data collection (i.e., reviews, commentaries, letters to the editor, study protocols) and non-English studies were excluded.
Review Framework
LBW, low birth weight.
Search strategy
Searches were undertaken on MEDLINE Ovid, EMBASE, Web of Science, Cumulative Index to Nursing and Allied Health (CINAHL), and Google Scholar, with no filters or limits applied. Searches were supplemented by scanning reference lists of articles included for review and consultation with field experts. Search terms included breastfeeding, breast milk feeding, preterm infant, LBW, intervention, and hospital discharge (Supplementary Table S2
Study selection
Titles and abstracts were screened independently by two reviewers (J.T.S., M.-L.W.K.) according to the prespecified inclusion and exclusion criteria. Discrepancies were resolved by discussion and a third reviewer (D.M.G.) was available to provide a decision should disagreements remain. Full text of these studies was then independently reviewed by the two reviewers (J.T.S., M.-L.W.K.), with the third reviewer (D.M.G.) available to provide an independent assessment in case of disputes regarding eligibility until consensus is reached.
Data extraction
A data extraction sheet was created using Excel (Microsoft, Redmond, WA). The two reviewers (J.T.S., M.-L.W.K.) independently extracted data from included full texts onto the sheet. The extracted details were study design, sample size, country, intervention, comparison, and quantitative data regarding outcomes. Any discrepancies were resolved through discussion between the two reviewers.
Quality assessment
Two reviewers (J.T.S., M.-L.W.K.) assessed the overall quality of included studies using the study quality assessment tools of the National Heart, Lung, and Blood Institute of the National Institutes of Health (NIH). 16 The NIH quality assessment tools are designed for a wide range of study designs, including randomized and nonrandomized controlled trials (RCTs), pre–post, cohort, and cross-sectional studies.
Data analysis
A narrative synthesis was conducted to summarize the characteristics of studies, analyze patterns within grouping of studies in terms of the direction of effects. A meta-analysis was conducted according to Mantel-Haenzel random-effects model using Review Manager (RevMan 5) to examine the effect of interventions on rates of any and exclusive breastfeeding at discharge (primary outcomes), and at 3 and 6 months postpartum (secondary outcomes). Forest plots were generated, and effect sizes were reported as odds ratios (ORs) with 95% confidence intervals (CIs). I2 test was conducted to estimate the extent of unexplained heterogeneity, with I2 > 50% considered high degree of between-study heterogeneity. Estimates of publication bias were considered using funnel plots for outcomes which included more than 10 studies.
Subanalyses explored primary outcomes by intervention type, study location (HICs vs. LMICs), by preterm infants alone, and by LBW infants alone. Sensitivity analyses tested if effect of interventions on any breastfeeding at discharge changed when restricting to only RCTs, studies rated high quality, and studies published in the last 5 years (≥2016).
Results
Characteristics of included studies
Of the 1,613 records identified, 42 studies were included in the review (Fig. 1). One hundred forty-seven full texts were reviewed for eligibility. Of these, 48 did not report an intervention or did not include a breastfeeding intervention, 4 had no comparator group, 16 did not report the outcomes of interest, and 12 did not include or separately analyze outcomes for preterm or LBW infants. In addition, 2 studies without primary data collection, 9 non-English publications, 11 abstracts only, and a further 3 duplicate studies were excluded.
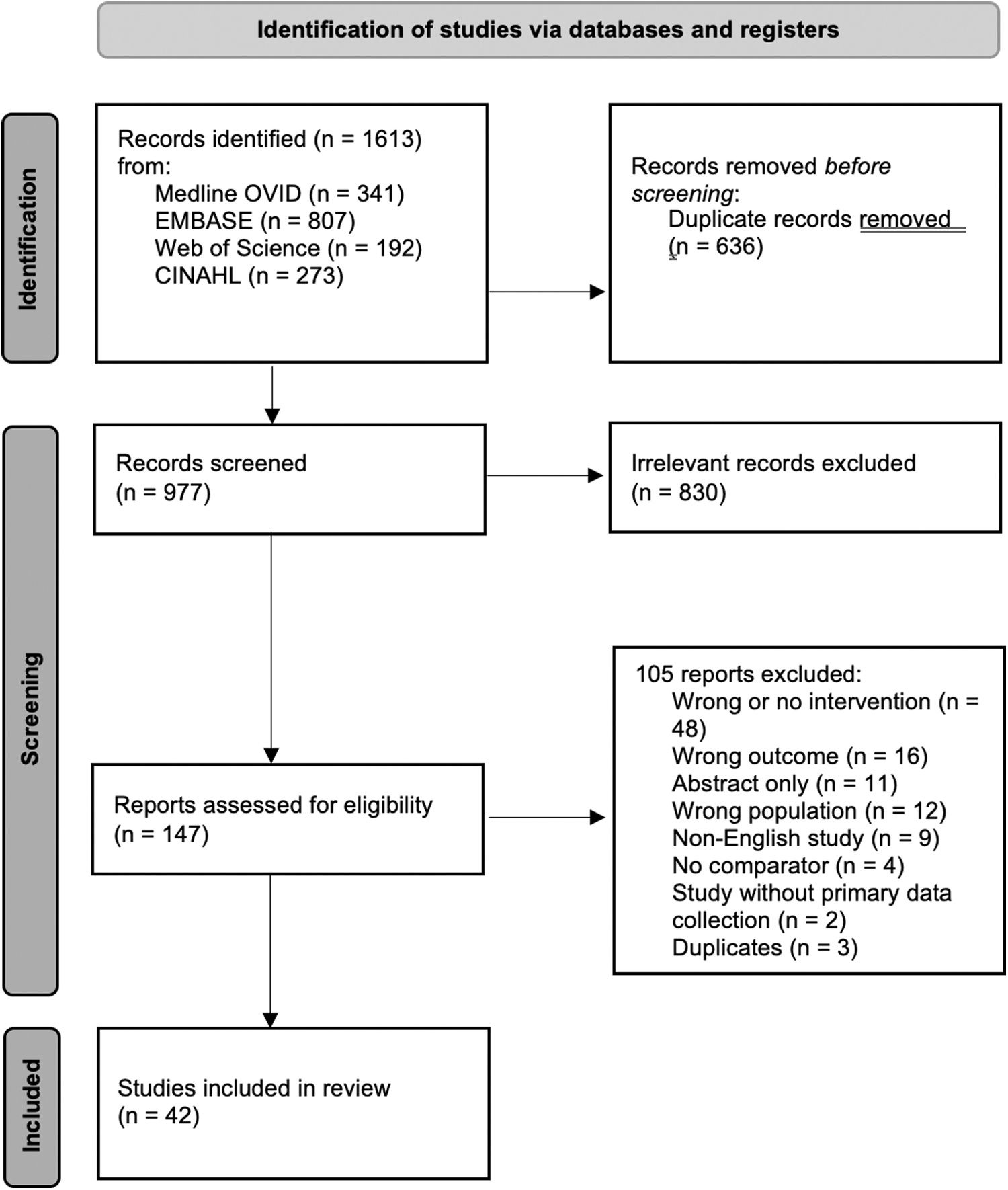
PRISMA diagram of included and excluded studies. One thousand six hundred thirteen records were identified, 977 records for screened, 147 reports were assessed for eligibility, 42 studies were included in this review. From: Page et al. 65 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Of the 42 included publications, publication years ranged from 2000 to 2021 and comprised different study designs: 14 observational cohorts, 2 cross-sectional studies, 1 case-control study, 5 pre- and post-design, and 20 controlled intervention studies (including 17 RCTs and 3 nonrandomized controlled studies). Interventions can be grouped into 6 categories: educational and breastfeeding support programs (10 studies), early discharge programs (3 studies), oral stimulation programs (5 studies), artificial teats and cups (5 studies), kangaroo mother care (KMC) (7 studies), and NICU policies and general characteristics (12 studies).
The youngest included preterm infants were born at 22 weeks' gestation, and the oldest were 36 weeks and 6 days gestational age. LBW (<2,500 g) and very LBW (<1,500 g) infants were also included in 11 studies. Thirty-five studies reported the outcome of any breastfeeding at discharge, 27 reported exclusive breastfeeding at discharge, 13 and 11 studies reported any or exclusive breastfeeding at 3 and 6 months postdischarge, respectively.
Ten studies (22%) were rated as good quality, 23 studies (56%) as fair, and 9 studies (22%) as poor. Five out of 17 RCTs were assessed as good quality for having relatively large sample sizes, adjusting for potential confounders, using appropriate and strong statistical analyses, and in some cases, able to blind both researchers and mothers of participants of the intervention. Four controlled intervention studies were rated poor for not having randomization, unclear reporting of attrition rates, small sample sizes and not considering important confounding variables. Among observational cohort studies, 5 out of 14 were rated as good quality due to having large sample sizes, controlling for potential confounders, and using robust statistical analyses.
Most of these “good” studies were large, multicenter studies that investigated NICU characteristics and policies and their impacts on breastfeeding outcomes. Four observational cohort studies were rated as poor, due to lack of adjustment for confounders, high attrition rates, small sample sizes, and having inherent baseline differences between intervention and comparison groups. Four of the five before and after studies were rated as fair and one was rated as poor due to small sample sizes and differences in baseline characteristics between the two groups. Some studies varied or were ambiguous in their definition of exclusive breastfeeding.17–19 Table 2 for characteristics of included studies and Supplementary Table S3 for details of study characteristics for each study.
Characteristics of Included Studies [N (%) or Median [Range], Unless Otherwise Stated]
High-income countries included: Australia, Canada, Denmark, France, Germany, Italy, Luxembourg, New Zealand, Norway, Portugal, Spain, UK, and the United States.
Low- and middle-income countries included: Brazil, China, Egypt, India, Iran, Malaysia, Turkey, and Ukraine.
KMC, kangaroo mother care; NICU, neonatal intensive care unit.
NICU characteristics and policies
Strengthening NICU policies and characteristics to support breastfeeding for preterm and LBW infants were the most common type of intervention with 12 studies. These included implementing feeding guidelines among NICU staff,20–22 parent friendly policies such as increasing visitation hours,20,23–26 increasing resources to support breastfeeding such as lactation consultants,20,24,25,27,28 and policies modeled after the Baby Friendly Hospital Initiative (BFHI).29–31
Supportive NICU policies that found evidence of higher rates of breastfeeding at discharge or at 3 months postdischarge include liberal parental visitation policies to promote a higher parental presence, 23 lactation consultants to support breast milk feeding initiation and maintenance,25,27,28 involving parents early in feeding support, 20 NICUs that provide spaces for parents to heat food, 25 and rooming-in. 26 Implementing a standardized parental feeding policy, with additional staff training on breastfeeding counseling skills and standardized messaging for mothers, improved any and exclusive breastfeeding at discharge,20,21 while another study introducing a feeding guideline found no statistically significant difference in breastfeeding at discharge. 22 This difference in outcomes between Burnham et al 22 and Low et al 21 can potentially be explained by Low et al's 21 emphasis on early initiation of oral feeding of mother's own milk, leading to a statistically significant earlier achievement of full oral feeds postpolicy.
In contrast, Burnham et al's 22 feeding policies did not emphasize early initiation of breastfeeding, which subsequently may have affected breastfeeding at discharge. Three out of five studies found that the presence of a lactation consultant increased any breastfeeding rates at discharge,25,27,28 while two studies by Mitha et al20,24 found no significant difference. In the Mitha et al20,24 studies, the variable presence of lactation consultants in NICUs may have contributed to this lack of effect. The lactation consultant was full-time dedicated for breastfeeding support in only 22% of the units, part-time in 34% of units, and not at all dedicated for breastfeeding support in 43% of units. 20 Three studies that implemented BFHI policies in NICU settings 30 or those modeled after BFHI—namely Best Fed Beginnings (BFB), 29 and Spatz 10 Steps for Promoting and Protecting Breastfeeding for Vulnerable Infants (10 Steps), 31 all saw a significantly higher rate of any breastfeeding at discharge.
Educational and breastfeeding support programs
Educational and breastfeeding support targeting parents and/or NICU staff were the second most common type of intervention with 10 studies. Program components included provision of emotional support and breast-pumping equipment, teaching of basic breastfeeding skills, encouragement from staff to practice these skills, and self-monitoring breastfeeding progress.18,19,32–39 Programs directed toward staff included lactation modules and training, streamlining of messaging about breastfeeding, and encouragement of staff to support breastfeeding mothers.18,33–35
Six studies found that infants in the educational/breastfeeding support interventions group had higher rates of exclusive breastfeeding on discharge,18,19,34,36–38 and five studies showed higher rates of any breastfeeding on discharge in the intervention group.19,33,34,37,38 For example, Fontana et al 38 found that parents who attended eight educational sessions to improve parent-infant interactions and recognize signs of infant stress had higher rates of infants fed with any breast milk (75.9% intervention vs. 32.1% control, p = 0.001) and exclusively breast milk (41.4% intervention vs. 10.7% control, p = 0.003). 38 Three studies that followed participants' postdischarge demonstrated a maintenance of higher rates of continued breastfeeding until 3 months of age,19,34,36 and two studies indicated that this maintenance continued up to 6 months of age.19,34 Three studies did not find a statistically significant difference in rates of exclusive or any breastfeeding at discharge postintervention.32,35,39
A majority of breastfeeding education and counseling interventions targeted parents only. Among six studies targeting parents, four found a significant increase in rates of breastfeeding at discharge.19,36–38 Among four studies that targeted both parents and health care workers, three found an increase in rate of breastfeeding at discharge in the intervention group.18,33,34
Kangaroo mother care
The third most common type of intervention was the implementation of KMC with seven studies included. KMC is a cost-effective and safe method of caring for infants that is characterized by early and continuous skin-to-skin contact between mother and infant, with exclusive breastfeeding. 40
All studies found that KMC was associated with higher rates of any and/or exclusive breastfeeding at discharge.41–47 Two studies found dramatically higher rates of exclusive breastfeeding rates at 3 months among KMC infants compared to infants who underwent routine care [(43.5% vs. 5%, p = 0.005) 44 ; 19% vs. 3%]. 45 At 6 months of corrected gestational age, Wang et al 46 found a significantly higher rate of exclusive breastfeeding among KMC infants (46.9% vs. 2.9%), 46 while Almeida et al 44 found no statistically significant difference in exclusive breastfeeding rates. 44 This difference in exclusive breastfeeding rates at 6 months between the two studies may be explained by their different study populations.
Wang et al 46 excluded infants with severe illnesses, while Almeida et al 44 included all infants whose weights were less than 2,000 g and did not exclude those with acute illnesses. Since the infants in the Wang et al 46 study may have been healthier, parents may have had more success with KMC, and thus, demonstrated a sustained beneficial effect that remained at 6 months of follow-up.
Other interventions
Other intervention types with fewer studies include oral stimulation, artificial teats and cups, and early discharge programs.
Five studies explored oral stimulation to facilitate preterm infants' oral feeding on breastfeeding rates at discharge. Oral stimulation consisted of stroking cheeks, lips, jaw, and tongue, with some studies also including non-nutritive sucking (NNS), which consists of allowing the infant to suckle on fingers, pacifiers, or emptied breasts, to strengthen the infant's sucking abilities.48–52 The stimulation was performed for 10 days during the infants' transition from tube to oral feeding. Four studies found significantly higher rates of any breastfeeding in the intervention compared to control groups48,49,51,52 but not significantly higher rates of exclusive breastfeeding.48,52 One study examining longer term breastfeeding outcomes did not find any difference between groups at 3 and 6 months of postdischarge. 51
Five studies explored the use of artificial teats and cups, including pacifiers, vacuum release teats and cups feeding on breastfeeding rates at discharge. Two studies examined pacifier use found that pacifier use may be associated with lower rates of exclusive breastfeeding at discharge compared to NNS on an emptied breast 17 but similar rates when compared to routine care.17,53 Two studies explored the use of a novel vacuum release teat attached to a bottle during feeds, which requires negative pressure to release milk so the infant practices the sucking motion needed for direct breastfeeding.
Results were mixed with one study finding significantly higher rates of exclusive breastfeeding at discharge 54 and the other finding no difference between groups. 55 Two studies investigated cup versus bottle feeding and both studies found significantly higher exclusive breastfeeding rates at discharge among the cup-fed group, but mixed results for any breastfeeding at discharge, and at 3 and 6 months postdischarge.53,56
Three studies investigated whether discharging clinically stable infants home a few days early with continued support from nurses until conventional discharge indication supported breastfeeding among preterm and/or LBW infants.57–59 Early discharge aimed to reduce psychological stress associated with long hospitalization and encouraged parental–infant interaction. The three studies varied in how early the intervention group was discharged compared to the routine group, as well as the amount of training and supervision parents were provided once home. Only one study found a beneficial effect on breastfeeding (88% vs. 80%, p < 0.005), which discharged infants an average of 3 days earlier, and formally trained parents in tube feeding, with 1–2 nursing visits per week. 58 Other studies did not find a difference in any or exclusive breastfeeding rates between the early discharge group and the routine discharge group.57,59
Meta-analysis
Interventions to promote human milk and breastfeeding among preterm and/or LBW infants were associated with significantly increased rates of any breastfeeding at discharge (OR: 2.05, 95% CI: 1.64–2.55, 46 comparisons, 57,372 participants, I2 = 93%) and exclusive breastfeeding at discharge (OR: 1.92, 95% CI: 1.54–2.40, 34 comparisons, 41,644 participants, I2 = 86%) in comparison to control groups. For our secondary outcomes, interventions were associated with a significant increase in any breastfeeding at 3 months postdischarge and 6 months postdischarge (3 months postdischarge: OR: 2.47, 95% CI: 1.57–3.88, 14 comparisons, 1,869 participants, I2 = 72%; 6 months postdischarge: OR: 2.48, 95% CI: 1.48–4.16, 12 comparisons, 1,992 participants, I2 = 68%).
In the subanalysis by study population, compared to no intervention, any intervention for preterm infants resulted in a significant increase in any (OR: 1.94, 95% CI: 1.52–2.48) and exclusive breastfeeding (OR: 1.75, 95% CI: 1.41–2.16). For LBW infants as well, interventions resulted in an increase in any and exclusive breastfeeding (any breastfeeding: OR: 2.98, 95% CI: 1.73–5.13; exclusive breastfeeding: OR: 6.26, 95% CI: 1.66–23.56).
Among high-income countries, compared to no intervention, having any intervention led to a significant increase in any and exclusive breastfeeding (any breastfeeding: OR: 1.73, 95% CI: 1.38–2.18; exclusive breastfeeding: OR: 1.64, 95% CI: 1.32–2.04). Among low- and middle-income countries, having any intervention again led to an increase in any and exclusive breastfeeding (any breastfeeding: OR: 5.33, 95% CI: 2.67–10.64; exclusive breastfeeding: OR: 2.88, 95% CI: 2.08–3.99).
For detailed results of this meta-analysis by intervention types, study location, and study population, please see Table 3. For forest plots and funnel plots of our outcomes, any breastfeeding at discharge, exclusive breastfeeding at discharge, any breastfeeding at 3 months and at 6 months postdischarge, as well as our subanalyses, please see Supplementary Figures S4–S15.
Summary of Findings
CI, confidence interval; OR, odds ratio; RCTs, randomized controlled trials.
Our sensitivity analyses examined if the effect of interventions on any breastfeeding at discharge changed when restricting to only RCTs, studies rated high quality, and studies published in the last 5 years (≥2016). We observed a positive effect of interventions on any breastfeeding at discharge in all three analyses (Table 3). Funnel plots (Supplementary Figs. S5, S7, S9, S11) for our primary and secondary outcomes were asymmetrical, suggesting potential publication bias.
Discussion
Overall, breastfeeding promotion interventions, including KMC, artificial teats/cups, early discharge programs, breastfeeding educational and support programs, oral stimulation, and breastfeeding supportive NICU policies, were associated with about a twofold increased odds of both exclusive and any breastfeeding among preterm and LBW infants at hospital discharge. For exclusive breastfeeding at discharge, only oral stimulation programs and artificial teats/cups did not show a statistical improvement among interventions identified. All interventions demonstrated statistically significant improvement in any breastfeeding at discharge. KMC was particularly effective, with over fourfold increased odds of breastfeeding at discharge among preterm and LBW infants compared to no intervention. BFHI, rooming-in, liberal visitation policies, and access to lactation consultants were effective NICU policies to promote breastfeeding among preterm and LBW infants. Breastfeeding interventions with preterm and LBW infants were effective at improving any breastfeeding rates from discharge to 3 and 6 months.
Interventions were effective in both HICs and LMICs, with potentially larger effects and lower heterogeneity in results in LMICs, especially for exclusive breastfeeding at discharge. However, there may be publication bias where studies with positive findings are more often published than those that did not find a significant result, as suggested by the asymmetrical funnel plots skewed toward the positive direction. We also note that, unfortunately, there were no studies for any interventions conducted in sub-Saharan Africa, the WHO region that currently has the most childbirths and a disproportional burden of premature deliveries and LBW infants. 60
Upon examining the effect sizes of intervention versus no intervention for preterm and LBW infants, having received any intervention among preterm infants resulted in a near twofold increase in odds of any and exclusive breastfeeding at discharge, while interventions among LBW infants led to a near threefold increase in odds of any breastfeeding at discharge, and a near fivefold increase in odds of exclusive breastfeeding at discharge. It is possible that the impact of interventions on breastfeeding rates at discharge is greater for LBW infants. However, because CIs for the two populations widely overlap, further statistical analysis is needed to determine if there is indeed a difference in intervention effects between preterm and LBW infants.
Although breastfeeding interventions remained significantly beneficial throughout all sensitivity analyses, heterogeneity remained high even after examining preterm and LBW separately, restricting to RCT study design, to good-quality studies, and recent publications in the previous 5 years. Only restricting studies to those conducted in LMICs substantially reduced heterogeneity for exclusive breastfeeding at discharge. HIC studies may include younger preterm and more VLBW neonates, who are more difficult to breastfeed and likely have more health complications, requiring prolonged stays at NICUs. There may also be a more reliable availability of formula in HICs, whereas there may be higher motivation to breastfeed among mothers in LMICs in the absence of accessible formula. While still substantial, KMC studies had the lowest heterogeneity among the interventions covered and KMC studies were largely found in LMICs. NICUs, on the contrary, varied in their characteristics, policies, and in the package of interventions delivered.
Overall, those that examined more comprehensive policy packages such as the UNICEF 10 Steps to Successful Breastfeeding, Spatz 10 Steps, and BFB found positive results,29–31 while studies that looked at certain policies in isolation, such as only implementing lactation consultants, had a mix of results.27,28
Our meta-analysis findings are in line with a previous scoping review 61 and integrative review, 62 which narratively summarized the benefits of KMC, breastfeeding education and support programs, artificial teats/cups and NICU policies, particularly rooming-in, on improved breastfeeding among preterm infants at discharge, 61 and exclusivity and duration of breastfeeding. 62 Our review found that artificial teats/cups only significantly improved any breastfeeding at discharge, not exclusive breastfeeding. In addition, our review did not restrict on prematurity level, while the Cartwright et al review focused only on late preterm infants (34–37 weeks gestation). 62 Other reviews only examined the outcome of breastfeeding initiation and focused on at term infants.13,14 KMC emerged as a key intervention to promote breastfeeding among preterm and LBW infants in our review, which may be missed in a review focusing only on term infants.
While most intervention types identified in this review showed positive impacts on breastfeeding, some interventions are more easily accessible than others. For instance, KMC and oral stimulation are both inexpensive and require little in terms of equipment. KMC in particular may be promising to support breastfeeding among preterm and LBW infants. KMC is currently recommended by the World Health Organization for the routine care of LBW infants weighing 2,000 g or less at birth who are in stable health condition, 63 but a recent multicountry trial has found evidence supporting the use of immediate KMC, while provisioning care for LBW infants has implications for using KMC during NICU stays. 64
To our knowledge, this is the largest review that examined breastfeeding interventions in the preterm/LBW population, which is not as often studied as term infants. In addition, our review focused on interventions that improved breastfeeding at discharge, not solely the initiation of breastfeeding. However, the review is limited by the inclusion of only English-language studies. Since our study focused only on interventions that aimed to increase breastfeeding, we did not analyze studies with interventions that may have inadvertently decreased breastfeeding, such as the use of human milk banks. Future research is needed to identify interventions that may interfere with breastfeeding among preterm or LBW infants.
Regarding NICU policies and characteristics, the present review was unable to analyze individual policies and their effects on breastfeeding rates, since many studies examined “packages” that included multiple policies. For example, the use of donor milk is included as part of the Spatz 10 Steps policy in Fugate et al and is not individually analyzed by the study authors. 31 The use of donor milk is mentioned in the following studies: Mitha et al 24 and Rodrigues et al, 25 but whether the use of donor milk led to a change in breastfeeding outcomes was not analyzed. Future studies measuring the impact of each policy change may be important to elucidate what element of the NICU environments prove to be the most supportive of breastfeeding in the preterm and LBW population.
Further studies are also needed with longer follow-up periods to better identify interventions with long-term benefits as well as how participant characteristics, such as socioeconomic status, maternal age, education level, family support, maternal stress, and anxiety, may influence impact of interventions.
Conclusion
There are a number of evidence-based interventions available to improve breastfeeding rates of preterm and LBW infants. While hospital settings for preterm and LBW infants, such as NICUs and KMC wards, may serve as a challenge to breastfeeding, it may also hold unique opportunities for breastfeeding promotion interventions since there is often longer engagement between family members and clinical staff. KMC emerged as a strong intervention to promote breastfeeding among preterm and LBW infants. More research is needed to understand the effects of KMC on breastfeeding at discharge in HICs and/or NICUs.
Footnotes
Authors' Contributions
J.T.S.: conceptualization (equal); data curation (equal); formal analysis (lead); methodology (equal); writing—original draft (lead); and writing—review and editing (equal). M.-L.W.K.: conceptualization (equal); data curation (equal); formal analysis (support); methodology (equal); and writing—review and editing (support). K.K.: conceptualization (equal); methodology (equal); supervision (equal); and writing—review and editing (support). D.M.G.: conceptualization (equal); methodology (equal); supervision (equal); and writing—review and editing (support).
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.