
Abstract
Objective:
The aim of this study was to investigate the effects of aroma of Citrus aurantium and Lavender essence on sexual satisfaction in breastfeeding women.
Materials and Methods:
This was a double-blind randomized controlled trial that was conducted on 180 breastfeeding women from January to May 2019. The participants were allocated to three groups of Citrus aurantium (n = 60), Lavender (n = 60), and control (n = 60) groups. Two groups of intervention used 2 drops of essential oil, twice a day, for 40 days as inhalation. The control group received almond oil in the same. The sexual satisfaction was evaluated using the Linda Berg's Sexual Satisfaction Questionnaire before the intervention and 40 days after the intervention started. The data were analyzed using the SPSS statistical software, version 21, and p < 0.05 was considered statistically significant.
Results:
After the 40 days of intervention, the mean score of sexual satisfaction was significantly higher in the Citrus aurantium and Lavender groups compared with the control group (59.3 ± 11.7, 59.3 ± 11.6 vs. 52.02 ± 11.5, p < 0.001). There was no significant difference between Lavender and Citrus aurantium groups.
Conclusions:
The results of this study showed that the aroma of Citrus aurantium and Lavender essence could significantly improve the sexual satisfaction of breastfeeding women. Therefore, it is recommended that health care providers should inform the breastfeeding women and advise them to use these interventions for increase of the sexual satisfaction. Trial Registration Number: IRCT20160427027633N3.
Introduction
Pregnancy and childbirth affects the mother's limbs and sexual organs in particular. These changes create problems in sexual intercourses. 1 Postnatal period, the first 6 months, and breastfeeding are the factors that affect sexual performance of couples. As studies have shown, 83% of women experience sexual problems during the first postnatal 3 months, which are rooted in painful intercourse, lack of vaginal lubrication, orgasm problems, loss of sexual desire, and post-intercourse bleeding and irritation. Hormonal effects triggered by breastfeeding might be the cause of vaginal dryness and a decline of sexual desire in women. 2 Postnatal period is featured with specific physical and psychological changes and it might affect sexual desire and activity as well. 3
A complete function of neuroendocrine system is highly important in sexual function. Norepinephrine, dopamine, oxytocin, testosterone, and estrogen create sexual arousal. Prolactin and serotonin control sexual responses. 4 Breastfeeding women experience less sexual satisfaction and activity owing to an increase in prolactin level that results in a decrease in gonadotropins and a decrease in sexual hormone level (estrogen, progesterone, and testosterone). An increase in stress level, fatigue, and secretion of milk during arousal and orgasm also contribute to these problems. 5 Positive response to pharmaceutical treatment is low in breastfeeding mothers and the main cause of it is the concerns about the side-effects. In addition, mothers are usually concerned about their health and breastfeeding their infant so that pharmaceutical treatments are a big worry for them. These women usually seek supplementary and alternative treatments. 6
Supplementary medicine is gaining more popularity not only for economic reasons but also for reliance of this medicine on holistic care and nursing theories. 7
Aromatherapy is a simple, accessible, and noninvasive technique, which is very popular among mothers. 8 Studies have shown that aromatherapy has many benefits in reducing stress, pain, anxiety, and relaxation by stimulating endorphin production.9–11 The probable therapeutic property of aromatherapy is through psychological and physiological (such as amygdala and hippocampus) routes.
The mechanism of action of these essential oils is two main ways: The first is through the olfactory pathway, which stimulates the receptors located in the olfactory bulb and transmits the olfactory message to the limbic system. This system is the brain's emotional center and is effective on pulse rate, blood pressure, respiratory system, and stress response. The second way is through skin absorption. Molecules of essential oils are absorbed through the skin over 20-40 minutes. 12
Citrus aurantium (Bitter orange) is from citrus family 13 and oil essence compounds like alkaloids, linalool, linalyl acetate, meceryne, limonene, limoneoids, and flavonoid are found in it. 14 Bitter orange oil is known for its anti-depression, disinfection, anti-spasm, relaxing, and increase of sexual desire effects. Studies have reported no side-effect for the oil. 15
Lavender (Lavandula officinalis) from lamiaceaea family is used for its disinfection, antibiotic, relaxation, improvement of digestive system, painkilling, and anti-anxiety effects. There are various compounds found in the essence of this plant and among the most important of them geraniol, linalool, linalyl acetate, cineol, borneol, camphor, butyric acid, and valrianik acid are notable. These compounds are the probable cause of the plant's effect on central nervous system and relaxation effects. 16 Linalool in orange blossom and lavender increases dopamine and noradrenaline effect. 17 This can be the probable cause of the effect on sexual satisfaction. Malakouti et al (2016) examined breastfeeding women's sexual performance 40 days after aromatherapy with rose, funnel, lavender, geranium, and orange. They reported an improvement in sexual performance of the subjects. 18 Another study on orange blossom or lavender reported a decrease in pain.19,20
Taking into account the prevalence of sexual intercourse problems during breastfeeding period, its effect on family and society health, and the fact that women are interested in supplementary medicine to avoid side-effects of standard medicine, this study is an attempt to determine and compare the effect of aromatherapy using Citrus aurantium and Lavender essence on sexual satisfaction of breastfeeding women. The participants were mothers visiting Kermanshah-based health clinics.
Materials and Methods
This randomized, controlled trial was conducted on 180 breastfeeding women who had low sexual satisfaction and referred to 2 health centers in Kermanshah, Iran from January to May 2019.
The sample size was calculated for each group based on the results of a previous similar study.18,21 The following equation was used to calculate the sample size:
In this equation, α = 0.05, β = 0.1, μ1 = 3.5, μ2 = 4.3, s1 = 1.6, and s2 = 1.2, and n = 54. We added 10% for attrition, and the total number of individuals in each sample group was calculated to be 60.
Inclusion criteria were Linden Berg's sexual satisfaction scale score <67, no mental and physical diseases, no sexual problem in the spouse (self-statement), no drug dependence, no experience of stressful events (divorce, death of first-degree family members, etc.) during the 6 months before the study, willing to participate, available health records in the health care center, ability to read and write, married and living with a permanent spouse, use of a reliable contraceptive method, breastfeeding (40 days to 6 months after child deliver), feeding the infant only with the mother's milk, not using medicine that affect sexual responses (blood pressure, diuretic thiazide, antidepressants, antihistamines, barbiturates, narcotics, diazepines, amphetamines, cocaine), no smoking, no drinking alcohol, no history of allergic rhinitis or a known respiratory problem such as asthma. Exclusion criteria were being unwilling to continue participation, experiencing side-effects or allergy to the essences, experiencing traumatic events, pregnancy during the study, mental or other health problem developed during the study, living away from the spouse, marital problems, and divorce or loss of the spouse during the study.
After receiving approval from the Ethics Committee of Kermanshah University of Medical Sciences, the researcher referred to two health centers for data collection. Eligible participants were randomly assigned to two intervention groups (Lavender [n = 60] and Citrus aurantium [n = 60]) and a control group (almond oil; n = 60). The participants were selected randomly from the health centers and then randomly allocated to two intervention groups (Lavender and Citrus aurantium groups) and a control group (almond oil) (Fig. 1). For random allocation, simple randomized method was used. So, 180 identical cards were prepared and 60 of them were marked by “1” (Citrus aurantium essence), on the other 60 cards “2” (Lavender essence), and on the last 60 cards “3” (control group). To determine their group, the participants were asked to draw one card (the participants were not informed about the allocation process). The Lavender essence, Citrus aurantium essence and almond oil were kept in identical containers and coded by a pharmacist. Each container was filled by one type of essence. Neither the statistician (the one who did the data analysis) nor the researcher (the one who was involved in sampling) was aware of the coding. The participants were briefed about the study and informed that they would randomly receive one of the containers containing Lavender essence, Citrus aurantium essence, or almond oil. The mothers were not blind to the intervention, but most of them in the intervention groups did not know whether the essential oil they smelled was Citrus aurantium or Lavender. Actually, they did not recognize the type of essential oil.
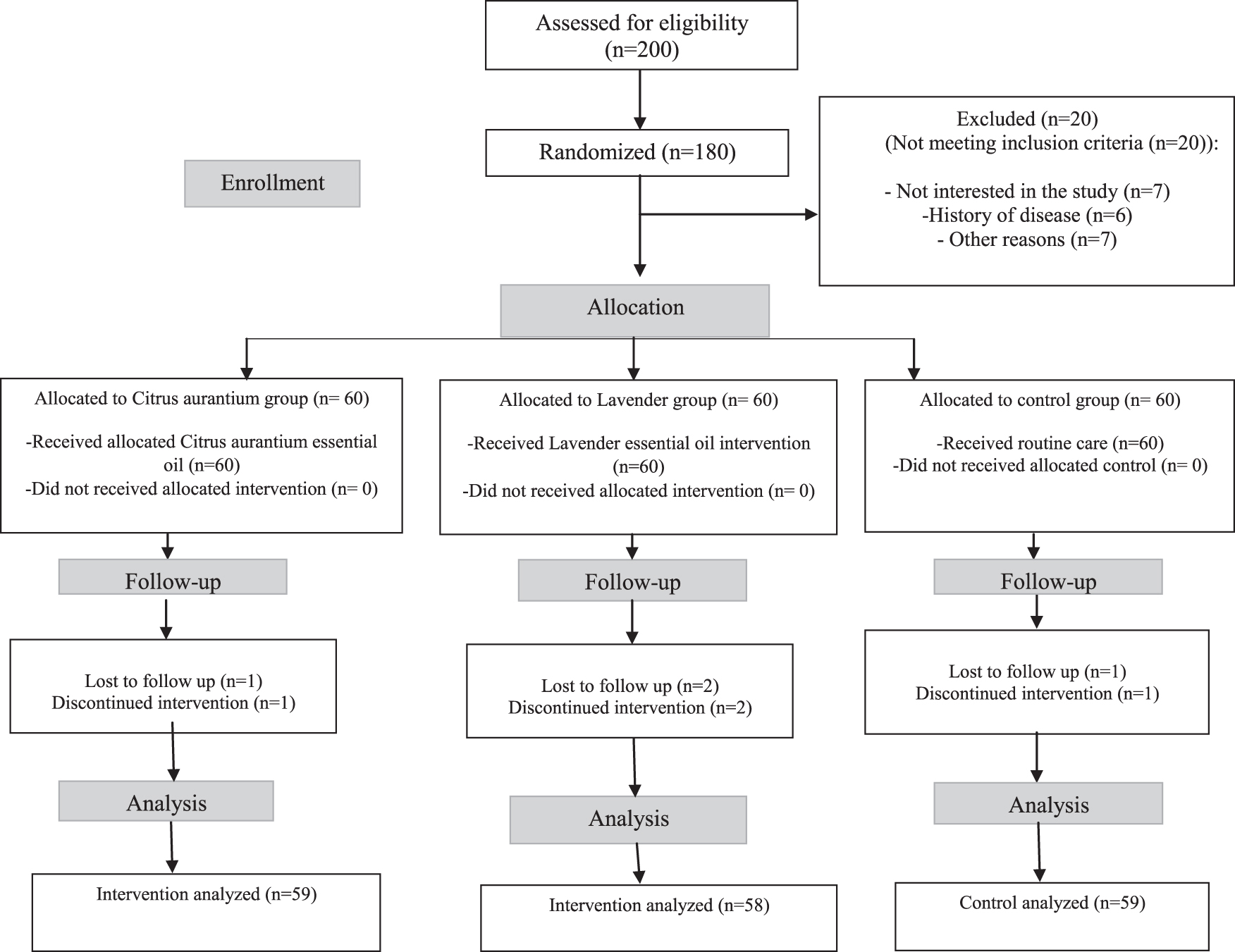
CONSORT flowchart of the study.
The participants received aromatherapy using the essences for 40 days following Malakouti et al. That is, 2 drops of 10% Lavender (Group 1), Citrus aurantium (Group 2), or almond oil (control group) were put on the forearm skin and inhaled for 5 minutes three times a day. 18
Each woman was instructed to be in a comfortable position and place her forearm 30 cm away from her nose and inhale the fragrance for 5 minutes with normal breathing. 18
One of the researchers made phone calls to the participants to make sure of the correct usage and check for any adverse effect. Before the start of the intervention and at the end of the 40th day after the start of the intervention, the participants were asked to return to the center to fill out the Linda Berg's sexual satisfaction questionnaire again.
Essential oil of Citrus aurantium and Lavender 10% was purchased from a pharmaceutical research center in Tehran (Iran) and approved by the Faculty of Pharmacy of Kermanshah University of Medical Sciences. Odorless almond oil, diluted with propylene glycol was purchased from a medicinal herbs market in the city of Kermanshah (Iran). Based on previous studies, almond oil was used in the control group.21,22
The concentration of essential oil was 10%, namely 10 mg of essential oil in 100 mL of odorless almond oil and diluted with propylene glycol. Propylene glycol maintained the stability of the essential oil. The amount of essential oil required for a 40 days intervention was provided to the participants at the beginning of the study and stored in the containers.
The data collection instruments consisted of two parts: (1) demographics and fertility questions (age, husband's age, education, husband's education, occupation, husband's occupation, income, marriage duration, type of contraceptive, first postnatal intercourse, number of intercourses in week, baby's gender, number of children, type of delivery, number of deliveries); (2) questions about sexual satisfaction of the participants based on Linda Berg's sexual satisfaction questionnaire. The questionnaire includes 17 items (always = 5, most of the time = 4, sometime = 3, rarely = 4, never = 1). The maximum and minimum scores are 58 and 17, respectively. To interpret the scores, 17–51 means low sexual satisfaction, 52–67 means moderate sexual satisfaction, and 68–85 means good sexual satisfaction. Validity and reliability of the questionnaire have been confirmed by Salehi Fadardi in Iran. 23
The collected data were analyzed with SPSS software version 23, using descriptive statistics (mean, standard deviation [SD], etc.) and inferential statistics (paired t test, chi-square tests, and one-way analysis of variance [ANOVA]). Kolmogorov–Smirnov test was used to ascertain normality of the data.
Paired t test was used to evaluate within-group differences. To compare mean score of sexual satisfaction (total score) at each time interval among the three groups, one-way ANOVA test was used. The significance level for all tests was <0.05.
The Ethics Committee of Kermanshah University of Medical Sciences, Kermanshah, Iran (code: KUMS.REC.1396.189) approved this study. All participants were fully aware of the study objectives and procedures and signed written informed consent. They were assured that their information would remain confidential. They were also informed that they could leave the study at any stage of the research.
Results
In this study, 200 women were assessed for eligibility; 20 were excluded for not meeting the eligibility criteria. Finally, 180 women were randomly allocated into Citrus aurantium, Lavender, and control groups (60 per group). One participant in the Citrus aurantium group, two in the Lavender group, and one in the control group were excluded owing to irregular use or reluctant to participate (Fig. 1).
Table 1 provides the sociodemographic characteristics of the participants in the three groups of Citrus aurantium, Lavender, and control. The participants' mean age was 29.7 ± 5.8 years, and the mean age of their husbands was 34.1 ± 5.9 years. No significant differences were found between the groups in terms of descriptive characteristics (p > 0.05).
Demographic Characteristics of Breastfeeding Women in the Study Groups
One-way ANOVA.
Chi-square tests.
ANOVA, analysis of variance; SD, standard deviation.
A one-way ANOVA indicated that the mean score of sexual satisfaction before the intervention was not significantly different among the three groups (p = 0.95). In addition, after the intervention one-way ANOVA showed that the mean score of sexual satisfaction was significantly different among three groups (p < 0.001). The mean ± SD of sexual satisfaction in the groups who received Citrus aurantium and Lavender were significantly higher than those of the control group at the end of the trial (59.3 ± 11.7, 59.3 ± 11.6, and 52.02 ± 11.5, respectively). Based on the paired t test, there was no significant difference between the baseline and the end of the intervention in the control group (p = 0.78), whereas there was a significant difference at the baseline and end of the intervention in the two intervention groups (p < 0.001) (Table 2). No adverse effects such as headache, dizziness, dyspnea, nausea, and vomiting were reported following inhalation of the aroma of Citrus aurantium, Lavender, and almond oil during the intervention.
Mean Scores of Sexual Satisfaction Between and Within the Citrus aurantium (n = 59), Lavender (n = 58), and Control (n = 59) Groups at the Baseline and After the Intervention
Pair t test.
One-way ANOVA.
Discussion
The effects of aromatherapy using Citrus aurantium and Lavender on sexual satisfaction in breastfeeding women were examined. After the intervention, the mean of sexual satisfaction score in the two groups who received Citrus aurantium and Lavender was significantly higher than that of the control group. The effects of Citrus aurantium and Lavender essences on increasing sexual satisfaction in breastfeeding women were the same. Therefore, these results suggest that aromatherapy with Citrus aurantium and Lavender improves sexual satisfaction in breastfeeding women. Consistent with our results, a previous study investigated the effects of lavender and bitter orange on sexual performance and satisfaction in women. The study examined sexual performance of menopausal women after 40 days aromatherapy using rose, funnel, lavender, geranium, and orange essence and reported an improvement in the participants' sexual performance. 18
Another study used aromatherapy with 0.1% and 0.5% orange blossom essence for 5 minutes twice a day for 5 days in postmenopausal women and reported an increase in sexual desire and concentration of estrogen in the participants. 24
The results of the study showed that using massage and aromatherapy with lavender, geranium, jasmine, almond oil for 30 minutes per week for 8 weeks decreases climacteric symptoms such as spasm, depression, and dyspareunia in menopausal women. 25
A branch of aromatherapy is focused on identifying the effects of this therapy on sexual problems. There are evidences that olfactory receptors can identify gender and individuals' sexual performance changes when exposed to the scent of opposite gender.26,27 Apparently, after absorption of volatile oils through the skin and respiration system and stimulation of very fine branches at the end of trigeminal sensory nerves in the nose and throat mucus, they affect, through reflexes, many key body functions including sexual desire. 28 Lynalol found that lavender increases dopamine and neuro adrenaline, which is responsible for the antidepressant effect of lavender. 17 The same mechanism can be responsible for the probable effect on sexual performance. Some of aromatic herbal essences in funnel, Persian hogweed, common sage, lavender, bitter orange, and geraniums contain phytoestrogen that stimulates nervous cells of olfactory center. Afterward, they discharge different neurotransmitters (endorphin, noradrenaline, and serotonin) that influence one's feeling and alleviate flush symptoms, sexual disorders, and depression.29–31
Given the results, aromatherapy increases sexual satisfaction in women through decreasing depression, increasing sexual desire, and increasing estrogen concentration.
Studies have shown that mixed aromatherapy does not have any effect on dyspareunia and sexual desire.20,32 Yosefzadeh et al found that date palm pollen improved orgasm in postmenopausal women so that it had no effect on sexual satisfaction. They argued that the reason can be one's attitude toward life, personal responsibilities, effects of environment on sexual relationships, sexual intercourses, and suppressors (e.g., anxiety, fear, and worries). They recommended more studies with higher doses and longer intervention terms. 33
Of advantages of this study were its three-side blind design and the very few participants who left the study. In addition, the random allocation of subjects to avoid selection bias and the use of blinding method to reduce the risk of bias during data collection were the other strengths of the study.
As to the limitations, failure to control all the factors in sexual satisfaction such as mental and spiritual mood and personal traits of the participants, which were beyond the control of authors, is notable. Since sexual matters are of taboo nature, finding the candidates was not easy. Another limitation was failure to find a proper placebo for aromatherapy.
Another limitation of this study was that we did not assess the causes and duration of sexual dysfunction that could affect the sexual satisfaction of women. Furthermore, we studied only the short-term effects of aromatherapy. On the contrary, this study was the first to assess the effect of Citrus aurantium and Lavender aroma on the sexual satisfaction in breastfeeding women.
Conclusion
The effects of aromatherapy using Citrus aurantium and Lavender essences on increasing sexual satisfaction in breastfeeding women were the same. Given that those interested in aromatherapy find it economic and free of pharmaceutical side effects, caregivers are recommended to use aromas along with standard care to solve sexual problems in breastfeeding women. In addition, it is recommended that health care providers should inform the breastfeeding women and advise them to use these interventions for increase of sexual satisfaction.
Footnotes
Acknowledgments
This article is the result of a research project with number 96432 and is financially supported by Kermanshah University of Medical Sciences. We would like to thank all of the participants in the study.
Authors' Contributions
All authors made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be submitted.
Disclosure Statement
S.H., F.S., and N.S. are employed by Kermanshah University of Medical Sciences, an institution that is involved in education and research.
Funding Information
This study was financially supported by Kermanshah University of Medical Sciences. S.H., F.S. and N.S. received research support from Kermanshah University of Medical Sciences (Grant number: 96432).