
Abstract
Objective:
To evaluate the association of the dietary inflammatory index adjusted for energy (E-DII®) with the evolution of maternal body mass index and human milk lipid (HM) profile in the first 6 months postpartum.
Methods:
This is a cohort study with 260 Brazilian women (19–43 years old) in the postpartum period. Sociodemographic, gestational, and anthropometric data of the mother were obtained in the immediate postpartum period and in the six monthly meetings. A food frequency questionnaire was applied at baseline and used to calculate the E-DII score. Mature HM was collected, analyzed by gas chromatography coupled with mass spectrometry and the Rose Gottlib method. Generalized estimation equation models were built.
Results:
Women with >E-DII showed lower adherence to physical activity during pregnancy (p = 0.027), higher frequency of cesarean delivery (p = 0.024), and higher body mass index over time (p < 0.001). At the end of the 6th month, 35 women remained in the study. As for HM, 151 analyses were performed, detecting in the 3rd collection greater fat (%) among those with >E-DII (4.27 ± 1.98 vs. 3.75 ± 2.48; p = 0.003).
Conclusion:
Diets with >E-DII can impact the type of delivery, change the evolution of maternal nutritional status, and the stability of the lipid profile of HM.
Introduction
Nutritional and environmental exposures during pregnancy can have adverse effects on a woman's health throughout her life, which can influence both health maintenance and the risk of comorbidities. 1 The role of maternal food consumption during this window of vulnerability, which corresponds to the gestational and postpartum period, is of particular interest for the prevention of obesity and other female health-related outcomes. Pregnancy, physiologically, is a proinflammatory state, and systemic inflammation becomes more present in overweight pregnant women. 1
A more inflammatory maternal diet during pregnancy has been shown to be associated with birth complications, obesity, and metabolic risk markers in 42 American women. The authors expressed concern about the spread of the proinflammatory state of obese mothers to their babies, and suggest that long-term metabolic outcomes be investigated. 2
Inflammation caused by diet has been studied in recent years, with a focus on the adult population and several comorbidities, based on the expansion of measures by indices such as the Dietary Inflammatory Index (DII®). Developed with the aim of quantifying the role of diet in relation to adverse health outcomes, the DII presents parameters that range from blood concentrations of inflammatory cytokines to chronic diseases. 3
Despite advances in research methods, there is still a lack of research that assesses the relationship between inflammation caused by food consumption in women during the perinatal period (including pregnancy and lactation) with the physiological changes of the nutritional status, and the lipid profile of human milk (HM). 1
As for lactation, it is known that HM is the best food option to be offered to the child, exclusively up to 6 months and supplemented up to 2 years of age or more.4–6 The protein and carbohydrate content of HM is relatively stable, however, the fatty acid (FA) content varies widely (40% to 70%), depending, among other factors, on the maternal diet. 7
In a North American study, the composition of FAs in HM, collected between 4 and 10 weeks postpartum, remained similar among women classified as eutrophic or obese in the pregestational period. However, the concentrations of omega-3, alpha linolenic acid, eicosapentaenoic acid, and docosahexaenoic acid in the group of obese women showed a significant reduction of 20%, 29%, 25% and 33%, respectively. Furthermore, the ratio of omega-6 to omega-3 was higher in this same group. 2
Therefore, the objective of this study is to evaluate whether there is an association between the inflammatory index of the maternal diet adjusted for energy (E-DII), on the evolution of nutritional status, based on the woman's body mass index and HM lipid profile in the first 6 months postpartum.
Methodology
Outline and population
This was a cohort study, composed of puerperal women recruited from June 2018 to June 2019 in a reference maternity hospital in Minas Gerais, Brazil.
Adult women were included in the study, in the immediate postpartum period, at least 24 hours postpartum, who reported good general health status, with live-born, full-term children, and who were willing to participate. Those with multiple pregnancies or those who reported a history of gestational diabetes mellitus, pre-eclampsia, or complications in their health or that of their children were excluded.
The need for 57 women was estimated considering a correlation coefficient (r = 0.44) between the DII score and the lipid composition of HM.2,8 A sample loss of 70% was considered, based on previous experiences of the linked research group. In total, 160 participants were estimated to be needed for the study
Data collection
Puerperal women
The puerperal women were invited for serial evaluations in the first 6 months postpartum, which included the monitoring of food consumption and nutritional status. Using a structured questionnaire, the women provided information regarding sociodemographic and anthropometric data in the pregestational period. Complementary data on the pregnancy were obtained by consulting the participants' medical records. Furthermore, at all times, the practice of exclusive breastfeeding was questioned (yes/no).
The sociodemographic variables were age, marital status (with or without a partner), education, occupation (with or without payment), and family income (<1 minimum wage, 1–3 minimum wage, and >3 minimum wages). 9 Among the data related to the gestational period, information was obtained regarding parity (primiparous and multiparous) and number of prenatal consultations (< 6 and ≥6). 10
For the anthropometric assessment, the following were investigated: pregestational weight and reported gestational weight gain. Current height and weight were measured at follow-up meetings (immediate postpartum and six monthly meetings). With these data, it was possible to calculate the pregestational body mass index (BMI = kg/m2) and current BMI at all subsequent moments, for adult women and adolescents. 11 The adequacy of gestational weight gain was performed according to the initial nutritional status in the pregestational period. 12 The practice of physical activity (yes/no), referring to the previous month, was also investigated at all times. 13
To determine food consumption, a semiquantitative food frequency questionnaire (FFQ) was applied in the immediate postpartum period, validated for the Brazilian adult population. 14 The information obtained in the FFQ referred to the last 6 months, so that the questionnaire applied corresponds to the last two trimesters of the gestational period. The instrument included foods from the following groups: milk and dairy products; meat and eggs; oils; snacks and canned foods; cereals and legumes; vegetables and fruits; desserts and sweets; beverages; and diet, light, and ultraprocessed products.
The questionnaire consists of 52 food items distributed among these groups and 7 consumption frequencies (once a day; two or more times a day; five to six times a week; two to four times a week; one time a week; one to three times a month; rarely or never).
Nutrient intake was calculated using the daily consumption of each food item and its nutritional composition. 15 Missing data from the Brazilian food composition tables were supplemented using references from the U.S. Department of Agriculture. 16 The information was tabulated in the Brasil Nutri® software. In addition, data from participants with caloric intake considered unlikely (< 600 kcal/day or >6,000 kcal/day) were excluded.17–19
To assess the inflammatory potential of the diet, the DII was used. This is an index developed by Shivappa et al., through an extensive scientific review of articles published between the years 1950 and 2010 about some dietary parameters, including macronutrients, micronutrients, and bioactive compounds, and their relationship with plasma inflammatory markers (IL-1β, IL-4, IL-6, IL-10, TNF-α, and C-reactive protein). With up to 45 parameters, the index assesses the potential effect of the diet consumed on systemic inflammation from scores that usually range from −8.87 to 7.98 (increasing inflammatory potential score). Such values, minimum and maximum, consider the use of all possible parameters.20–25
The calculation of the E-IID® score in this study was performed based on the 28-food consumption data previously obtained from the FFQ: considering, as an adjustment, nutrient intake by energy density (total consumption per 1,000 kcal); carbohydrates; proteins; lipids; cholesterol; saturated, monounsaturated, polyunsaturated, and trans fats; omega-3 and omega-6; dietary fiber; magnesium; iron; zinc; selenium; thiamine; riboflavin; pyridoxine; niacin; beta-carotene; caffeine; folic acid; and vitamins A, D, E, C, and B12. Similarly, Moore et al. and Sen et al. used 28 and 27 parameters (with variations between 0.4 to 1.5 and −2.6 to 1.4), respectively, to evaluate the DII without differences in the predictive capacity of the index, when compared with the greater scope of the instrument.26,27
To avoid acquiring arbitrary values due to the use of raw amounts of food intake with different measurement units, a representative database was established for populations from 11 countries. Food consumption information from the current work was standardized based on the mean and standard deviation of each DII food parameter from the data provided. The standardized values of each dietary parameter were converted into percentage averages and multiplied by their respective inflammatory effect scores calculated from the literature review on the index.20,28 For this study, the total DII ranged from −1.3 to 1.9.
In addition, in this research, the E-DII scores were classified as below (less inflammatory diet) or equal to or above the median values (more inflammatory diet).
Human milk
From the 5th postpartum week on, all women were invited to donate a volume between 30 and 50 mL of HM 29 the meetings were carried out in the morning and afternoon periods. For the allocation of mothers with their respective children, the appointment was made randomly, respecting the family's preference. The extraction of the HM was performed during meetings between feedings, until 6 months postpartum or while lactation lasted, for the analysis of the composition of FAs present in the HM at different times of the study.
The collection and storage process followed the rules proposed by the National Network of Human Milk Banks. 30 All samples were stored in a freezer at −80°C. 31 The determination of the lipid composition of HM was performed using gas chromatography coupled to mass spectrometry (GC/MS). This method allows transesterification to be carried out directly, that is, without prior extraction of the fat, resulting in a fast method with little reagent expense (Fig. 1). The test was performed in a gas chromatograph (Agilent 7890B) equipped with a mass spectrometry detection system (Agilent 5977A -MSD), with a quadrupole mass analyzer. The column used was SPTM −2330 capillary (80% biscyanopropyl/20% cyanopropylphenyl siloxane), 30 m × 0.25 mm × 0.20 μm internal diameter.
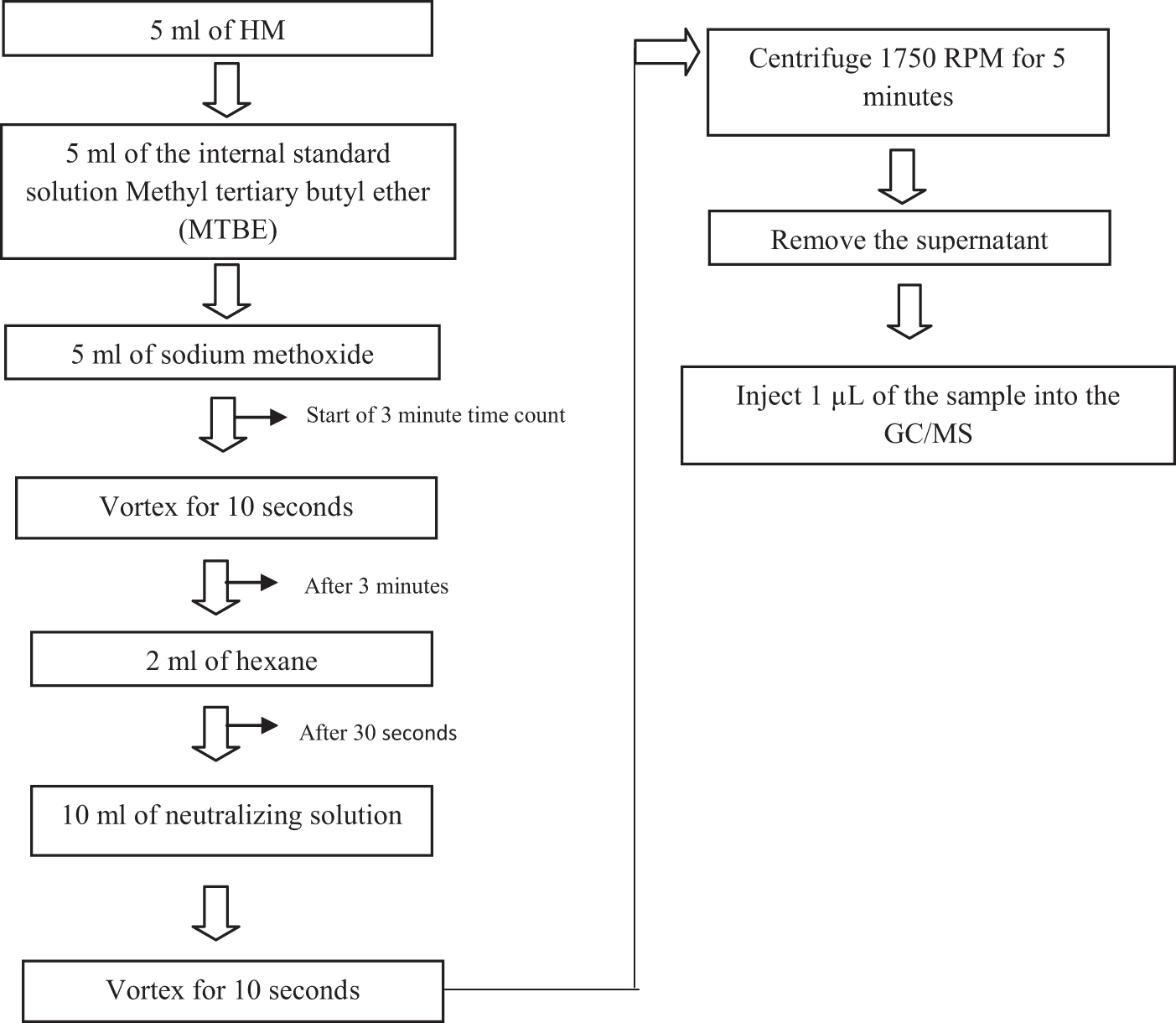
Flowchart of the lipid transesterification method by AOAC, 2012. AOAC, Association of Official Analytical Chemists; HM, human milk; MTBE, methyl tertiary butyl ether; GC/MS, gas chromatography/mass spectrometry; RPM, rotation per minute.
The oven temperature programming started with 120°C for 1 minute and then increased in increments of 4°C per minute until a temperature of 240°C was reached, remaining for another 15 minutes and totaling an analytical run of 46 minutes. Helium gas was used as carrier gas at a constant flow of 1 mL per minute. The injection mode was with flow division (split) of 1:10 and injection volume of 1 μL.
Data acquisition took place in SCAM and SIM mode, using charge–mass ratio (m/z) from 14 to 500. The chromatograph interface with the detector was maintained at 240°C and electron impact ionization operated at 240°C was used. The mass analyzer was a single quadrupole type operated at 150°C.
The mass and fragmentation profile of the peaks found was compared with the FAME C4–C24 standard and the spectra bank of the National Institute of Standards and Technology (NIST) library. The results of percentage of Fames were compared with the results of total lipids obtained in the methodology of Rose Gottlib 32 (extraction of total lipids, Fig. 2), which refers to a method standardized for infant formula and adapted for HM analysis. 29

Flowchart of the lipid extraction method by Rose Gottlieb adapted.
To carry out the analysis, subsamples were considered both for the lipid determination of HM and for the characterization of FA.
Statistical analysis
The data collected were tabulated in the Epi Info program, version 7.0, by means of double typing, which allowed for the proper consistency analysis. Descriptive analysis included estimates of measures of central tendency and dispersion for quantitative variables and frequency distribution for categorical variables. Data normality was tested by the Shapiro–Wilk test. Mann–Whitney and t-Student tests were performed to compare medians and means in two independent samples, respectively, as well as the chi-square test to compare proportions.
The model of generalized estimation equations was used to evaluate the evolution of maternal BMI and the lipidic percentage of HM from the E-DII classifications. The variables were treated as a normal distribution, with a connection identity function. The working correlation matrix used was the unstructured and robust estimated covariance matrix. In this analysis, the post hoc test used was the Bonferroni for intra- and intergroup comparison, and these models were adjusted for the variables: exclusive lactation, family income, education, maternal age, and physical activity. Furthermore, the model referring to the lipidic percentage of HM was also adjusted for the mother's nutritional status (BMI along the segment).
The Software Statistical Package for the Social Sciences (SPSS) version 23.0 was used and a significance level of 5% was adopted for all analyses (p-value <0.05).
Ethical aspects
The study was conducted in accordance with the guidelines and standards of Resolution No. 466/2012 of the National Health Council, and approved by the Research Ethics Committee (COEP), number 52537215.5.0000.5149 and by the National Research Ethics Committee (CEP-CONEP) (CAAE 86818118.0.0000.5149).
Results
A total of 260 women were recruited from the hospital, with a median age of 28 (19–43) years, the majority (96.2%) being adult puerperal women (≥20 years). The largest portion (65.6%) had completed high school and 65.8% reported having a partner (Table 1).
Sociodemographic, Gestational, and Anthropometric Characteristics of the Woman at Baseline, According to the Maternal Diet Inflammatory Index Score
Bold values indicate p-value < 0.05 (statistically significant).
Median values (min-max).
BMI, body mass index; tests: Mann–Whitney and chi-square.
At baseline, women with higher E-DII (≥0.04; 95% CI: 0.01–0.17) showed lower adherence to physical activity (9.3% vs. 20.0%; p-value = 0.02) and higher frequency of cesarean delivery (33.1% vs. 24.2%; p-value = 0.02). At this time, no other significant differences were observed according to the E-DII classification (Table 1).
They remained in the study for six months of follow-up, total of: 68 (26.15%), 44 (16.92%), 36 (13.85%), 32 (12.31%), 29 (11.15%), and 35 (13.46%) women in the 1st, 2nd, 3rd, 4th, 5th, and 6th month, respectively. It is noteworthy that women under the age of 20 years did not return for follow-up 6 months postpartum.
Evolution of the maternal body mass index according to the E-DII
It was observed that the women's BMI, regardless of the E-DII classification, evolved differently over time (p < 0.001) (Table 2). However, among those classified with higher E-DII, higher BMI means, and a significant difference between moments 1 and 6 (27.80 kg/m2 ± 0.62 vs. 25.36 kg/m2 ± 0.69) and 2 and 6 (27.84 kg/m2 ± 0.66 vs. 25.36 kg/m2 ± 0.69) were observed. Therefore, among women who had greater adherence to a more inflammatory diet, it was observed that BMI parameters took longer to reduce and/or stabilize over time.
Evolution of Maternal Body Mass Index (Mean ± Standard Error) Over Time According to the Inflammatory Index of the Diet
Distinct lowercase letters show that the means of anthropometric indices differ within a given time. Distinctive capital letters show the evolution of a given group over time. Generalized estimating equations (GEEs) model. The model was adjusted for exclusive breastfeeding, income, education, maternal age, and physical activity. Caption: E-DII = Inflammatory index of the energy-adjusted diet; baseline = immediate postpartum; time 1 = 30 days postpartum; time 2 = 60 days postpartum; time 3 = 90 days postpartum; time 4 = 120 days postpartum; time 5 = 150 days postpartum; time 6 = 180 days postpartum.
Human milk
A total of 121 analyses were performed on different women during the first 6 months postpartum. The mean total fat concentration at all times was 3.86% ± 1.80%, with significant differences in the 1st HM collection according to the E-DII classification (Table 3). In addition, 30 random samples (different women and time points) were analyzed for FA determination, and the three most evident in the HM of the participants were oleic acid (C18:1 n-9) (31.65% ± 6.67%), palmitic acid (C16:0) (25.07% ± 5.23%), and linoleic acid (C18:1 n-6) (18.31% ± 3.64%), with no differences between the E-DII classifications.
Characterization of the Lipid Profile of Human Milk from the Inflammatory Index of the Diet
Bold values indicate p-value < 0.05 (statistically significant).
Test: t-Student.
A higher concentration of caprylic acid (C8:0) was identified in the 1st HM sample among women with higher E-IID® (0.53% ± 0.05% vs. 0.36% ± 0.06%; p < 0.001).
There was also a significant difference between the age classifications (≤25 years and between 26 and 35 years) of women who donated at least one HM sample when compared with those who did not donate (19.5% vs. 41.6%; p-value = 0.013). Other information is described in Table 3.
Evolution of HM total fat over 6 months, according to maternal E-DII
The fat of women's HM, regardless of the E-DII classification, evolved differently over the 6 months postpartum (p-value = 0.003). In Figure 3, among the women classified as having the highest E-DII, significant differences were observed between the values of total fat at moments 1 and 5 (4.4% ± 0.3% vs. 1.5% ± 0.5%), 1 and 6 (4.4% ± 0.3% vs. 0.2% ± 0.9%), 2 and 5 (3.1% ± 0.2% vs. 1.5% ± 0.5%), 2 and 6 (3.1% ± 0.2% vs. 0.2% ± 0.9%), 3 and 5 (5.3% ± 0.8% vs. 1.5% ± 0.5%), and 3 and 6 (5.3% ± 0.8% vs. 0.2% ± 0.9%). In the comparison between the index classifications, at the 3rd moment, a higher percentage of HM fat was identified among those with higher E-DII (4.2% ± 1.9% vs. 3.7% ± 2.48%).

Variation of total fat in human milk during the first six postpartum periods, according to the inflammatory index of the maternal diet. Distinct
Discussion
In this study, it was identified that women who consumed diets with higher E-DII had lower adherence to physical activity during pregnancy, greater occurrence of cesarean section, and higher BMI values at baseline, which took longer to reduce throughout the follow-up. In addition, a higher percentage of total fat in the HM was identified in this group, with a higher concentration of caprylic acid.
As for the lower adherence to physical activity associated with the highest E-DII, regardless of age, educational level, or type of physical exercise, some authors have found a direct association between the practice of activity with greater consumption of healthy foods, such as fruits and vegetables. Likewise, unhealthy eating patterns (more inflammatory) are associated with sedentary behaviors that may help to explain the findings of this study. 33
There was a difference when comparing the highest frequency of cesarean section identified with a North American cohort with ethnic diversity. In the study previously mentioned, such a relationship was pointed out in women with obesity. 34 This condition, like pregnancy, is intrinsically a more inflammatory state and may be associated, among other factors, with a food consumption characterized by ultraprocessed products, rich in sugars and fats, mainly saturated and trans FAs. 35
In >10,000 North American women, a greater chance of cesarean delivery was found among women who had a lower quality of diet (first quartiles of the index), measured by the Healthy Eating Index-2010 (HEI-2010). Poor prepregnancy food intake was also associated with several other negative maternal outcomes including hypertensive disorders, preterm birth, and obesity. 36
Similar studies showed that women who had a higher BMI in the immediate postpartum period also had higher E-DII when compared with those with lower values.37,38 However, unlike the current findings, such results were not identified in the monitoring of maternal nutritional status (1st and 6th month postpartum) in the study conducted by Zhou et al., highlighting the need for more studies to monitor this evolution and the presence of other associated factors, such as adherence to EB. 38
Among women who donated HM, donation was significantly higher among those aged between 26 and 35 years. The findings in the literature indicate that the highlighted age group includes a phase of lower vulnerability and greater adherence to lactation when compared, for example, with adolescence, a period characterized by intense changes, both physiological and social.18,23,38,39
With regard to women with higher E-DII, a higher percentage of fat was observed in the HM, with values in line with the findings in the literature (3% to 5%),t of caprylic acid (C8:0) was also higher at the first moment. Belonging to the class of saturated FA, it is considered important in the structuring of HM, as they present themselves as an energy source or as a substrate for the synthesis of intermediate components. The formation of FA (C8:0) in milk is influenced by maternal nutrition, and diets characterized by low percentages of lipids and high percentages of carbohydrates (an important inflammatory marker) intensify the presence of these FAs in the HM. 39
Corroborating the findings of this study, Penfield-Cyr et al. identified a positive correlation between maternal DII and the FA saturated of the HM. In addition, another study found that HM from obese mothers has a general profile of proinflammatory FA and reduced FA concentrations that have been shown to play a critical role in the infant's growth, visual, and neurological development.2,40 However, such associations were not found in this study, and it was also not possible to follow the evolution of the HM profile over time from the maternal E-DII because of the interruption of the analysis due to the coronavirus pandemic (COVID-19).
The location chosen for this study may also be a factor that contributed to some divergences with the literature, given that there was no significant difference between the maternal E-DII and the practice of exclusive lactation up to 6 months of the baby's life. It was a maternity hospital certified as a Baby-Friendly Hospital, which has among its goals, the promotion, protection, and support of lactation.
Also, the possibility that unmeasured confounders, such as genetic factors, may influence the observations made, as well as the sample losses inherent in cohort studies, cannot be excluded. Still on sample losses, this limitation, observed mainly at the 6th month postpartum, is due to the financial difficulties of the women in the study. In Brazil, research participants cannot receive financial incentives, so displacement and other expenses to attend the research site can be a limiting factor for many families, which may have contributed to low adherence to the research. Despite the limitations, there are no studies in the literature that have evaluated the anthropometric indices of both the mother and the child and the HM lipid profile from the maternal E-DII over time so far, highlighting the relevance and novelty of the topic.
It was, therefore, concluded in this study that women who consumed diets with higher E-DII had lower adherence to physical activity in the gestational period, greater occurrence of cesarean deliveries, greater BMI during follow-up, and greater instability of the lipid profile of the HM during the 6 months postpartum.
The findings of this study also pointed out the complexity of the period that extends from pregnancy to lactation, reinforcing the need for a more detailed screening, in different health services (public/private).
Finally, there is also a growing need for more studies and specific nutritional guidelines for this stage of life and for the entire reproductive period of women. The consumption of foods with a lower inflammatory profile is indicated, which includes, especially fresh foods, minimally processed foods and includes good food sources of AG, such as olive oil, tuna and salmon, to enable better results in maternal health both during the lactation period, as well as in the long-term nutritional status, which also reflects on the adoption of good eating habits by the child.
Footnotes
Disclosure Statement
Dr. J.R.H. owns the controlling interest of the Connecting Health Innovations (CHI), a company that licensed the right to his invention of the Dietary Inflammatory Index (DII) from the University of South Carolina to develop computer and smartphone applications for patient counseling and dietary intervention in clinical settings. Furthermore, Dr. N.S., who is another author of this study, is an employee of CHI. However, these issues do not bear any direct relation to this study, nor did the activities described exert any influence on this project. The authors L.B.F., T.N.S., G.C., A.S.C., R.L.B.A., and L.C.S. declare that there is no conflict of interest.
Funding Information
Financial support was granted by the Coordination of Improvement of Higher Education Personnel (CAPES - Financial Code 001), National Council for Scientific and Technological Development (CNPq - Research Productivity Scholarship (301555/2019-2), and Universal Public Notice 2016 (406644/2016 -0).