
Abstract
Background:
Domperidone is a dopamine-2 antagonist used off-label to increase breast milk production. Dosages commonly promoted for lactation are often far above those of studied on-label indications and might pose additional risks, especially upon discontinuation of the drug.
Patients:
Three U.S. patients are presented who used domperidone for lactation and experienced varying degrees of psychiatric withdrawal symptoms lasting months during dosage tapering and after cessation.
Conclusion:
Domperidone as a galactagogue may pose a significant psychiatric risk upon discontinuation. This presentation is commonly confused with, but clinically distinct from, postpartum depression. Lactating mothers who present with psychiatric symptoms should be explicitly probed about domperidone use, even in areas where domperidone is not authorized for use. Maternal hesitancy to disclose domperidone use may lead to suboptimal outcomes for the patient and delay management of withdrawal manifestations. The best course of treatment remains unknown, but a slow hyperbolic taper to gently discontinue domperidone may minimize withdrawal symptoms in these patients. Individuals exploring domperidone use should be informed of potential risks upon withdrawal, including psychiatric manifestations, requisite taper, and potential impacts of using unstudied high doses.
Introduction
Inadequate milk production is a common concern among lactating mothers. 1 Common etiologies include maternal illness, premature childbirth, low prolactin levels, and early mother-infant separation. The inability to provide sufficient milk for the infant(s) is distressing and understandably drives many mothers and their health care providers (HCPs) to seek solutions. Common first-line options for increasing milk supply include evaluations of breastfeeding technique, infant latch, or maternal medical disorders. 2 Then, pharmaceutical galactagogues may be appropriate. 3
One drug used as a galactagogue is domperidone, a high-affinity antagonist of dopamine-2 (D2) receptors. 4 This mechanism encourages multiple clinical applications. Antiemetic effects of D2 antagonism are responsible for domperidone's primary indications as a gastric prokinetic agent. Off-label lactogenic effects are secondary to dopaminergic blockade, which stimulates the release of stored prolactin in the anterior pituitary. 5 In the brain, dopamine antagonism produces an antipsychotic effect. However, unlike other D2 antagonists, central nervous system effects are rarely reported with domperidone due to minimal transfer across the blood-brain barrier. 6
Domperidone is not legally available in the United States due to concerns regarding Q-T interval prolongation; the FDA has warned against its use as a galactagogue. 7 However, lactating women may learn about domperidone from the internet or from providers who care for breastfeeding individuals. Anecdotal evidence suggests that domperidone use is not uncommon in the United States. Further, patients may be reluctant to disclose domperidone use to physicians due to fear surrounding its legality. Medically unsupervised use of high doses of domperidone is concerning due to cardiac risk alone. In countries supporting gastric indications, the maximum recommended dose is 30–40 mg/day for limited durations.8,9 However, galactagogue doses vary widely and range as high as 180 mg/day. 10 Simultaneously, there is no research suggesting that doses >60 mg/day produce higher prolactin levels or milk production; evidence suggesting an improvement in milk supply using a 60 mg/day versus 30 mg/day is contested.11,12
A literature review revealed five case reports and two qualitative interviews depicting potential psychiatric consequences of domperidone withdrawal. In 2013, Papastergiou et al 13 reported the first incident of psychiatric symptoms, tachycardia, and insomnia in the setting of abrupt withdrawal from 80 mg/day of domperidone used as a galactagogue. Conventional antidepressants were ineffective in relieving the subject's symptoms. Reinstating the 80 mg/day dose with a 10 mg/week taper ultimately proved to be effective in resolving symptomology. 13
In 2017 and 2018, two case reports depicted two similar patients' relief requiring a slower taper. Manzouri and Mink 14 reported a woman who took 80 mg/day for <9 months abruptly discontinued the dose, resulting in insomnia, anxiety, nausea, headache, and palpitations 2 weeks after the last dose. After resuming 60 mg/day to mitigate withdrawal symptoms, the final taper required a dose reduction of 2.5 mg every 2 weeks.
Doyle and Grossman 15 reported withdrawal symptoms in a woman taking a maximum dose of 160 mg/day. After 14 weeks of treatment, she tapered by 10 mg every 3 to 4 days until reaching a dose of 20 mg/day when she stopped the drug entirely. A week later, she exhibited insomnia, rigors, psychomotor agitation, and panic attacks. She resumed a dose of 90 mg/day with a 10 mg/week dose reduction, but symptoms reemerged when she reached 20 mg/day. The final phase of dosage tapering took 3 months to complete without recurring withdrawal symptoms.
A severe presentation was published in 2014 of a mother taking 30 mg/day for 8 months. 16 After abrupt discontinuation, the mother experienced insomnia, severe anxiety, akathisia, dysphagia, and cognition and memory issues resulting in suicidal ideation for at least 10 months.
There is only one previously reported case of withdrawal from domperidone in a patient with preexisting psychiatric history, following the same pattern of presentation, recovery, and level of severity as those without preexisting illness. 17 The mother experienced reemergence of obsessive-compulsive disorder and major depressive disorder 1 week following the abrupt discontinuation of 120 mg/day of domperidone after 6 months of use. Other symptoms included insomnia, anxiety, irritability, poor concentration, loss of libido, and lack of energy; she denied thoughts of suicide. The reintroduction of domperidone at 120 mg/day with a 10 mg/week taper (without the support of other psychotropics) ultimately succeeded in remission of her symptoms, although she sought psychiatric support halfway into the taper.
A 2021 thesis study interviewed 18 mothers regarding their off-label use of domperidone in Canada. Two of the 18, unprompted, reported “devastating” psychiatric symptoms, including anxiety, dysphoria, and akathisia, within days of stopping or reducing domperidone. 18
The growing number of reports from women with psychiatric symptoms during withdrawal from domperidone is concerning. At least one of these cases likely originated from the United States. 15 However, the lack of FDA approval in the United States renders physicians unfamiliar with the drug, a factor that, combined with lack of disclosure, can lead to a subsequent missed diagnosis. This report details the presentation and clinical course of domperidone withdrawal among three lactating individuals with separate tapering schedules at different stages of recovery.
Case Presentation
In August 2021, the three patients depicted in this case series contacted the InfantRisk Call Center, which assists clinicians and patients with questions regarding lactational pharmacology. All reported severe psychiatric symptoms following discontinuation of domperidone. Semistructured interviews were conducted and recorded via Zoom. This project was determined to be exempt by the Texas Tech University Health Sciences Center IRB. Case details are included in Table 1.
Case Presentations of Our Three Patients
HCPs, health care providers.
Case 1: “Those were the darkest moments of my life.”
In Case 1, the patient began domperidone obtained from an international website at 90 mg/day to nurse an adopted newborn as advised by a lactation book. She discontinued domperidone after 5 weeks by decreasing 10 mg of her total daily dosage at weekly intervals (e.g., during the first week of the taper, her dose was reduced to 80 mg/day; the second week, 70 mg/day, and so on). Seven days after beginning the taper, she experienced severe anxiety, pulsatile tinnitus, insomnia, and perceived increase in urine output. Two weeks into tapering, the patient returned to her baseline dose, but symptoms persisted; she found relief by increasing her dose to 120 mg/day. During this time, she reports multiple visits to the emergency department (ED) and with various medical providers in the United States.
Due to the nature of medication acquisition, the patient reported hesitancy to discuss her domperidone use during these visits. Online research led her to consider domperidone withdrawal as a possible source of her symptoms, prompting disclosure to HCPs. Several weeks later, a primary care physician advised slowing the tapering regimen by decreasing the total daily dosage by 10 mg at 2 week intervals rather than weekly; this was unsuccessful due to the recurrence of the aforementioned symptoms. Eight weeks following the previous attempt, she began to taper once again by decreasing 10 mg of her total daily dosage at weekly intervals. However, she had a recurrence of symptoms such as insomnia, severe anxiety, and agitation, but this time with suicidal and homicidal ideations, at which point she increased her dose to 150 mg/day with complete resolution of psychiatric symptoms.
She then decreased her daily dose by 2.5 mg every 2 weeks for 4 weeks, followed by 2.5 mg reductions every week as tolerated. This schedule will require more than a year to complete, but thus far has prevented the onset of symptoms (Table 1; Fig. 1a).
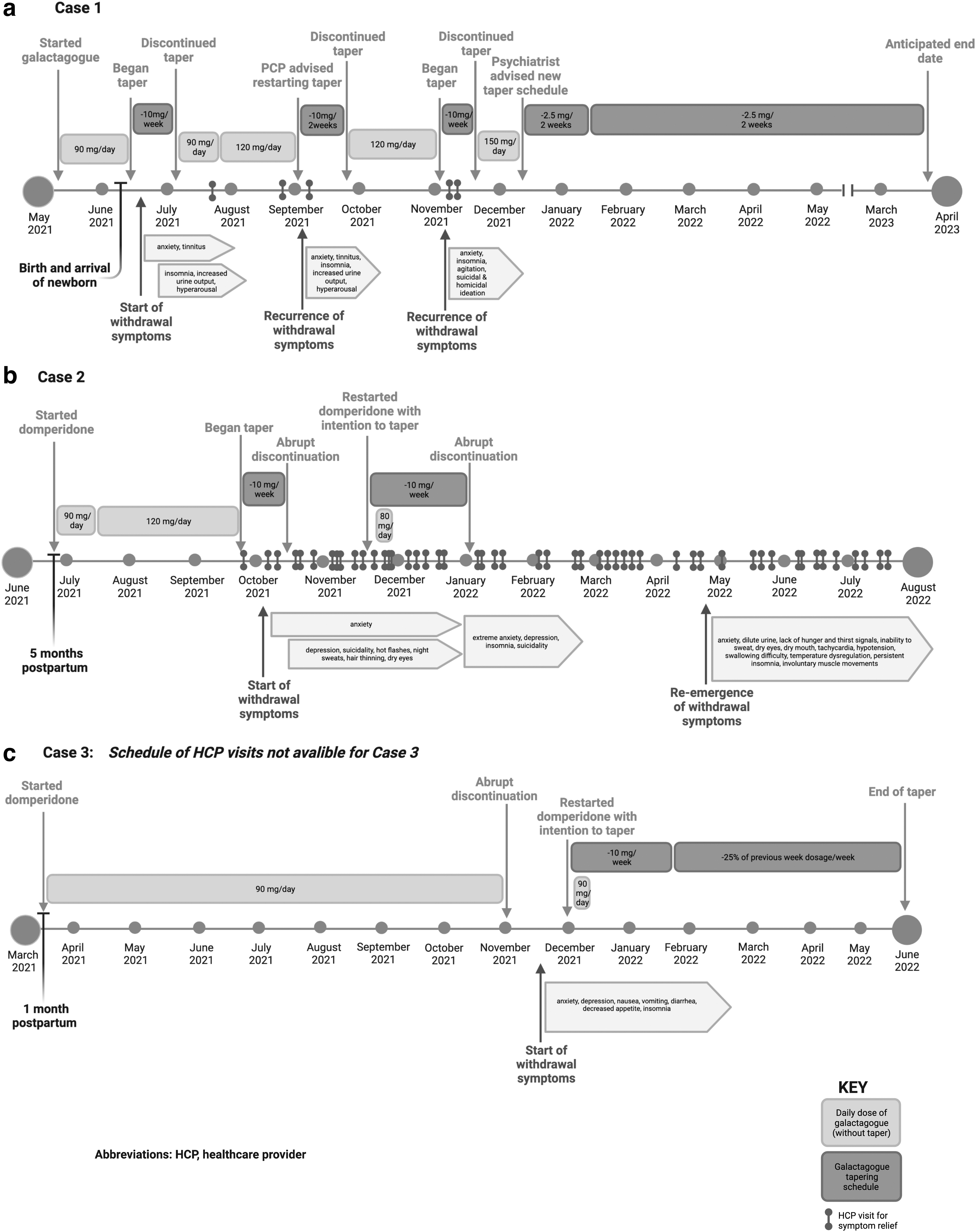
Timeline of tapers, presentation of withdrawal, and related visits to HCPs for each case presentation:
Case 2: “I can't believe I did this to myself when I never even needed it.”
In Case 2, the patient began a prescription of domperidone at 90 mg/day 5 months after delivery under the supervision of an online physician outside of the United States. Two weeks later, she increased her dose to 120 mg/day due to continued perceived low milk supply. After 3 months, she began a taper which decreased her total daily dosage by 10 mg each week. Within 2 weeks, at 100 mg/day (20 mg into the taper), the patient felt anxious and stopped domperidone immediately with subsequent anxiety, depression, and suicidality, along with hot flashes, night sweats, hair thinning, and dry eyes. She had multiple ED visits and a 2-day admission to an inpatient psychiatric unit for suicidality.
Her online provider advised returning to her maximum dose of domperidone and restarting the weaning process. The patient did not feel comfortable returning to 120 mg/day, instead reinstating 80 mg/day with a plan to continue reducing the daily dose by 10 mg/week. She tried this regimen for 6 weeks without relief of symptoms. She then elected to abruptly discontinue the domperidone without taper again. She rapidly experienced extreme anxiety, depression, and insomnia. She was unable to care for her child and felt distant from him. Several weeks into withdrawal, her primary anxiety, depression, and suicidality eventually resolved. Novel symptoms (Table 1) presented with a reemergence of anxiety, all still present 8 months after the initial taper. She reports multiple additional suicide attempts throughout this period (Fig. 1b).
Case 3: “[Domperidone has] ruined my life.”
In Case 3, the patient began domperidone 90 mg/day one month postpartum under the supervision of an online prescriber outside the United States. After 8 months, the patient discontinued domperidone; she did not recall any discussion of tapering by her prescriber. Two weeks after abruptly stopping therapy, she experienced severe anxiety, nausea, vomiting, diarrhea, decreased appetite, and insomnia. She admitted to depression and thoughts of being a burden to her family. She was initially unable to return to work and did not feel safe independently caring for her infant. She sought care from her online domperidone provider, who sent an email with the standard tapering regimen. She misunderstood the instructions, further delaying the taper.
After contacting her prescriber and the research laboratory for clarification, she began the recommended tapering schedule. She returned to her previous dose, then began a taper which decreased her total daily dosage by 10 mg each week, during which she experienced some resolution of symptoms over the next 3 months. The patient was admittedly impatient with the taper but cited worsening symptoms each time she attempted to accelerate the process. During the last 20 mg of the taper, she slowed the tapering regimen to a 25% dose reduction every week to alleviate symptoms of anxiety and insomnia. Six months after beginning to taper domperidone, the patient reports that she is symptom-free, no longer taking domperidone, has returned to work after extended leave, and can independently care for her child (Table 1; Fig. 1c).
Discussion
The three subjects in this report consumed 90–150 mg/day of domperidone for perceived low milk supply. In line with previous reports, withdrawal symptoms of insomnia, severe anxiety, depression, and intrusive thoughts were dominant. While it is unknown why psychiatric symptoms arise upon drug withdrawal, large doses may be associated with significant penetration of domperidone through the blood-brain barrier, a property not generally associated with on-label doses. 19 Most cases of psychiatric withdrawal from domperidone used doses of at least 80 mg/day; however, one previous severe report followed a 30 mg/day dose. 16 It is possible that genetic variation in efflux capacity of domperidone at the blood-brain barrier in some women could mimic high doses overwhelming the blood-brain barrier. 19 Duration of treatment with domperidone does not appear to influence symptom severity in previously reported cases, a quality reflected in our case series.
Consistent with previous reports, antidepressants, anxiolytics, antipsychotics, and sleep aids were largely ineffective at treating these patients' symptoms.13,14 Most cases reported no personal or family history of psychiatric disorders. Prior psychiatric history was noted only in the Sharma et al 17 case report and Case 3 of this series. In Case 3, symptomology was clinically distinct from her prior postpartum depression and appeared to have activating features (Table 1). These two reports seem no more severe than the withdrawal exhibited by cases without psychiatric history.
It is commonly accepted that domperidone should be tapered upon cessation to manage withdrawal effects, usually by decreasing the total daily dosage by 10 mg each week. The cases in this series, coupled with previous reports, suggest that this common tapering regimen may be more aggressive than some patients can tolerate.14,15 Regardless, higher doses require extended time frames for patients to be free of the drug.
The theory of dopaminergic supersensitivity may account for the rapid development of psychiatric symptomology following the discontinuation of domperidone. 20 It suggests that chronic antagonism is responsible for an increased functional state of each D2 receptor. Alternatively, or simultaneously, chronic antagonism may result in compensatory upregulation of D2 receptors. In tandem, these theories may synergistically increase dopaminergic sensitivity.
Further, the antagonism of the receptors would mask either of these processes until domperidone is discontinued. Horowitz et al 21 suggest that a hyperbolic taper may be effective in these cases. Hyperbolic tapering decreases the dose by 10–25% every 3–6 months to allow for the resolution of underlying adaptations. They also suggest that necessary final doses may be as small as 1/40th of a therapeutic dose. A hyperbolic regimen was more successful for symptom management in Cases 1 and 3 than sudden discontinuation or decreasing the total daily dosage by 10 mg each week.
In the United States, HCPs have limited to no experience recognizing and treating this withdrawal phenomenon. This is primarily due to the drug's lack of FDA approval because of concerns for fatal cardiac arrhythmia. Apprehension about the legality of domperidone use initially inhibited the patients in this case series from freely divulging the medication use to their HCPs. This was most significant for the patient who obtained the drug online without medical supervision. Patient reticence when providing medical history paired with sparse domperidone awareness likely resulted in suboptimal diagnosis and care in these cases.
Further, because American patients often become aware of the drug through online forums and can obtain the drug from online sources, there may be suboptimal consideration and discussion of domperidone's risks. Many patients adjust their dosages without medical supervision, as described in both our case series and a 2021 qualitative study. 22 The most effective intervention may be increasing awareness of the risks and benefits of domperidone, including those of psychiatric withdrawal, among lactation consultants and physicians with whom lactating patients might come into contact. Providers practicing in psychiatry, family medicine, internal medicine, emergency medicine, and obstetrics and gynecology are most likely to encounter patients withdrawing from domperidone. Therefore, lactating patients with psychiatric symptoms should be explicitly asked about domperidone use as a part of their medical history.
A major limitation of this case series is the sole reliance on the patients' anecdotal reports sourced from interviews. There was no independent review of patients' medical records, which would have included laboratory values, imaging, medications, past medical history, clinician visits, and symptomology.
Despite domperidone's not being approved status for marketing in the United States, there remain sources that encourage its foreign purchase and use by mothers interested in increasing their milk supply. Limited information prevented these mothers from making fully informed decisions. These patients all suggested that they would never have consumed domperidone had they been made aware of and expected the risk of difficulty of withdrawal. They expressed a shared sense of frustration, helplessness, and desire to prevent others from repeating their experience.
Footnotes
Acknowledgment
We thank Janet C. Currie for her expertise and guidance on this topic.
Authors' Contributions
All authors listed for this article were directly involved in the study design, article preparation, and article draft. All authors have consented to the publication of this article in Breastfeeding Medicine. E.M.: investigation, original draft preparation, review, and editing; S.H.: investigation, original draft preparation, review, editing; K.K.: conceptualization, methodology, original draft preparation, review, and editing; A.S.: review and editing; T.W.H.: review, editing, guidance, and supervision.
Disclosure Statement
None of the authors of this article has any conflict of interest to disclose.
Funding Information
This article was not funded by any source.