
Abstract
Background:
Many preterm infants cannot breastfeed directly and depend on other feeding methods. Multiple studies have compared feeding methods for such infants; however, the best method remains unknown. We compared Nifty cup with Katori-spoon feeding in preterm neonates deemed fit for oral feeding.
Methods:
This open-label randomized controlled trial was performed in a level III neonatal unit. Preterm (<34 weeks) neonates deemed fit to initiate oral feeding were randomly allocated to the Nifty cup and Katori-spoon groups. Patients were followed up until 40 (±2) weeks of postmenstrual age or until death, whichever occurred earlier. The primary outcome was time to achieve full oral feeding. The secondary outcomes included the time spent per feeding session, time to full direct breastfeeding, anthropometry at discharge, duration of hospitalization, and mortality. The opinions of mothers and nurses were recorded using a structured questionnaire.
Results:
A total of 106 participants (53 in each group) were randomized and analyzed for the primary outcome. The median (1st, 3rd quartile) time to achieve complete oral feeds was 5 (2, 11) versus 6 (4, 11) days in the Nifty cup versus Katori-spoon groups, respectively (p = 0.2). Infants in the Nifty cup group reached full breastfeeds earlier (mean difference = 12.6 days; 95% confidence interval: 4.3 to 20.8, p = 0.003) and had less vomiting (9.4% versus 26.4%, p = 0.023). Mothers and nurses felt that breast milk expression and feeding with a Nifty cup was easier.
Conclusions:
Compared to the Katori-spoon, feeding with a Nifty cup did not shorten the time to full oral feeds. However, it helps in attaining full breastfeeds earlier than the Katori-spoon.
Trial Registration:
Clinical Trials Registry—India (CTRI/2021/06/034252).
Introduction
Globally, more than 15 million preterm infants are born annually, of which over 80% are from Asia and sub-Saharan Africa. 1 Many of these premature infants cannot be breastfed directly in the first few days to weeks of life and require alternative feeding modes like gavage, bottle, cup, paladai, or Katori-spoon until they can transition to direct breastfeeding. In developed countries, bottles are the default feeding mode for babies who cannot be breastfed, but are fit for oral feeding. However, due to increased infection risks and nipple confusion associated with bottle feeding, World Health Organization and United Nations Children's Fund recommend cup feeding in low-resource settings.2,3
Cup feeding provides infants with positive oral, tactile, olfactory, and auditory stimulation, and helps establish breastfeeding. 3 Also, they are relatively easy to clean and reuse. However, there are concerns that traditional cups have poor milk flow control, leading to increased spillage and the risk of choking and aspiration.2,3 Moreover, conventional cups are not wide enough to allow hand expression of milk. Breast milk must be expressed in a wide-mouth container, and then, a measured amount is transferred to the cup. The use of multiple containers and measurements predispose infants to contamination. Furthermore, there is wide variation in cup size, design, and material. 3
At our center, we use Katori-spoon (reusable stainless-steel utensils pictured in Fig. 1) for oral feeding until the mothers can directly breastfeed. 4 Mothers first express milk in the Katori and then transfer it to a syringe for measurement. The requisite amount is again moved back to the same Katori and given to the infant with a thick, blunt-edge stainless-steel spoon. This Katori-spoon has similar disadvantages to a traditional cup, except that the milk expression is straightforward.

Katori and spoon.
Nifty cup (Laerdal Global Health, Stavanger, Norway pictured in Fig. 2) is a reusable cup made of soft silicone that can be boiled or autoclaved.5,6 This cup has a capacity of 40 mL and has a millimeter measurement marking over it. The moldable nature of the cup allows the direct expression of milk. The cup has measurement markings so that the expressed milk can be given directly to an infant without changing utensils. The reservoir of the cup helps the infant to lap milk from it, while controlling the feeding pace.

Nifty cup.
McKinney et al compared the Nifty cup with the traditional cup and Paladai, and observed good acceptability of the Nifty cup among health care providers.5,6 However, they did not report neonate-related clinical outcomes. In this randomized controlled trial (RCT), we aimed to assess whether preterm (<34 weeks' gestation) infants fed with a Nifty cup take less time to reach full oral feeds than traditional Katori-spoon feeding.
Methods
We conducted an open-label, parallel-group, superiority RCT in a level III neonatal unit at a referral center in a developing country from June 15, 2021, to December 15, 2021. The study protocol was approved by the institute's ethics committee and prospectively registered with the Clinical Trials Registry, India (CTRI/2021/06/034252). This study was conducted in a step-down neonatal nursery. The infant-mother dyad stayed together, and mothers/caregivers were involved in feeding and infant care.
In the step-down neonatal nursery, infants are received from the neonatal intensive care unit (NICU) once they are stable from hemodynamic and respiratory perspectives, can maintain temperature without incubator/radiant warmer, and are on full enteral feeds. We screened all preterm infants born at <34 weeks of gestation, staying with their mother, and on gavage feeds. Infants on full gavage feed [150 mL/(kg·d)] for at least 3 days and considered fit for transition to oral feeding (spoon/cup) were eligible for enrolment.
We excluded infants with gastrointestinal and craniofacial malformations (where spoon feeding is difficult or not feasible), necrotizing enterocolitis stage II or higher, gastroesophageal reflux requiring medical or surgical management, severe (grade III/IV) intraventricular hemorrhage, neonatal seizures, and hypoxemic ischemic encephalopathy. We enrolled eligible neonates after obtaining written informed consent from one of the parents.
We allocated subjects using a stratified block randomization design with the following strata: (1) gestational age up to 30+6 weeks and (2) gestational age between 31 and 33+6 weeks. One of the investigators (J.K.) generated a web-based (www.randomization.com) randomization sequence and constructed randomly varying, permuted, and even-numbered blocks for each stratum. He concealed the block sizes until the end of the study and was not involved in the subject recruitment. We ensured allocation concealment by using serially numbered, opaque, sealed envelopes containing a slip of paper with the allocation group. Blinding was not possible due to the nature of the intervention. However, the statistician was blinded to the group allocation during the analysis.
The first investigator (N.G.) enrolled the participants and allocated them to the Nifty Cup and Katori-spoon arms. This was an investigator-initiated, investigator-driven study. The unit purchased Nifty cups, Katori, and spoons from the open market, and the manufacturer or seller had no role in study planning, design, conduct, or analysis. Except for the mode of oral feeding, the management remained the same for both groups and was as per standard unit protocols. Most infants are started on enteral feeds from day one in our unit, and feeds are advanced by 20–30 mL/(kg·d). Sick neonates and those born before 32 weeks of gestation are started on gavage feeds and are gradually transitioned to oral feeding once they are deemed fit (>32 weeks postmenstrual age [PMA], hemodynamically stable, on room air, demonstrate normal rooting and swallowing, and no contraindication for oral feeding).
Infants between 32 and 34 weeks receive gavage/spoon-feeding/mixed feeding depending upon the sickness and feeding skills, whereas infants more than 34 weeks are given either spoon or direct breastfeeds. In the author's unit, expressed breast milk (EBM) (primarily by hand expression) is used for infant feeding, and mothers are encouraged to express breast milk from the 1st day. In the step-down unit, nearly 85% of infants receive exclusive breast milk, and 15% get mixed (EBM + formula milk) feeding as a human milk bank was not available at the time of the study. We followed a 2-hourly feeding schedule for all participants.
The bedside nurses trained the mothers for Katori-spoon/Nifty Cup feeding. They performed the initial few feeding sessions until the mother was confident of feeding the baby with the allocated device. Supervised feeding sessions were performed until the mother was fully confident and could feed the baby independently. Almost all infants admitted to the step-down unit are shifted from the NICU and have multiple neonatal illnesses during the first few days of life; they are kept on multipara monitors until they reach 34 weeks PMA and are apnea free for at least a week after stopping caffeine. The index study monitored the vital signs of all infants during the feeding sessions. Oral feeding was withheld if there was any acute adverse event, such as apnea, bradycardia, desaturation, or vomiting during feeding. All adverse effects were recorded.
Daily 2–3 feeding sessions for each infant were directly supervised by the primary investigator until discharge. The duration of the feeding session (from when the Nifty cup/spoon touched the lip until the last sip) was noted. In addition, mothers were asked to record the duration of feeding sessions (at least 2–3 sessions per day) separately from those supervised by the investigator. The primary investigator also assessed spillage during the directly observed feeding sessions. A preweighed cotton bib was used to determine spillage, which was weighed after the feeding session to determine actual spillage. As both Katori-spoon and Nifty cups are autoclavable, routine autoclave/boiling was done per the unit protocol. The allocated feeding mode (Nifty or spoon) was continued until the infant achieved full direct breastfeeding.
Our center primarily deals with high-risk deliveries and has a high turnover rate. We back refer many infants to state-owned level II special newborn care units (SNCUs) once they are on full enteral feeds (orogastric tube/spoon) and need to stay in the hospital for weight gain or transition to breastfeeds. Therefore, many infants in the index study were expected to be referred back to the SNCUs. Infants referred before reaching full oral feed were followed twice weekly to inquire about the volume of feed given through the allocated device. The following information was sought: the day on which full oral feeding was achieved, compliance with the intervention, and any adverse event. Infants back-referred or discharged on full oral/breastfeeds were followed weekly (telephonically) if and until they were admitted to the SNCU and fortnightly (physically) after discharge. All neonates were followed up until 40 (±2) weeks PMA or death, whichever occurred earlier.
Outcomes
The primary outcome was the time to achieve full oral feeding. The time to full oral feeding was defined as the time from the initiation of the first oral feeding after randomization to the time point of achieving full oral feeding. We defined the achievement of full oral feeds when the infant received at least 150 mL/(kg·d) feeds for 3 consecutive days exclusively through a Katori-spoon/Nifty cup with no gavage feed. The 1st day the infant received 150 mL/(kg·d), and no gavage feed was considered the time point of achievement of the outcome. The outcome was not considered achieved if a neonate required any session of gavage feed before the completion of 3 consecutive days of oral feeding.
The secondary outcomes included duration of the feeding session, adverse events (aspiration, vomiting, or apnea), time to reach full breastfeeding, weight gain [g/(kg·d)], anthropometry (weight, length, and occipitofrontal circumference) at discharge, duration of hospitalization, and mortality until discharge. The neonate was classified as being on full direct breastfeed if they were exclusively breastfed for 3 successive days without any Katori-spoon/Nifty cup or gavage feed session.
As it was a new intervention for the unit, we assessed compliance with the intervention, satisfaction of mothers, and feedback from the nurses and mothers regarding the Nifty cup using a structured questionnaire. The questionnaire was developed by us and was validated on mothers and nurses (10 each) before adapting to the study.
Sample size
Previous studies have shown that feeding with Nifty cups leads to less spillage, regurgitation, and a shorter feeding duration.5,6 Therefore, we assumed that it would be superior to traditional Katori-spoon feeding in achieving full oral feeding earlier. In a previous study, the median (interquartile range) duration of the transition from gavage to oral feeding in a 2-hourly feeding group was 11 (9–16) days. 7 Based on this study, we needed 94 participants to detect a significant difference of 3 days in time to full oral feeds (transition duration) with 5% α error and 80% power. We enrolled 106 participants, considering a 5% chance of noncompliance or crossover in the intervention group.
Statistical analysis
Categorical variables were described as percentages, normally distributed numerical variables as means (standard deviations), and those with skewed distributions as medians (1st, 3rd quartiles). Skewness was determined using the Shapiro–Wilk test and Q–Q plots. Categorical outcome variables were compared using the χ 2 or Fisher's exact test, and numerical variables using the Student's t test or Mann–Whitney U test. We performed a preplanned linear regression analysis to determine whether the intervention was an independent predictor of time to full oral feeds after adjusting for prespecified variables such as gestational age, birth weight, and PMA at enrolment. We analyzed the intention to treat using SPSS version 23 (IBM SPSS Statistics, IBM Corporation) for statistical analysis.
Results
We screened 138 infants, of which 106 were enrolled, and all were analyzed for the primary outcome (Fig. 3). The baseline characteristics were similar across the groups, except for birth weight, which was lower (p < 0.01) in the Katori-spoon group (Table 1). Overall, 19 (18%) infants were born before 28 weeks, and 27 (25%) had extremely low birth weights (<1,000 g). Neonatal morbidities before enrolment were similar between the two groups (Supplementary Table 1).

CONSORT flow diagram. IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis.
Baseline Characteristics in Nifty Cup and Katori-Spoon Feeding Groups
p Value <0.01 for birth weight and 0.013 for length. For the rest, the p value was >0.05.
PMA, postmenstrual age; SD, standard deviation.
Ninety-three (88%) infants achieved full oral feeds during the hospital stay, and the remaining 13 reached full oral feeds after back-referral to SNCU. As decided earlier, all those who achieved full oral feeds until the study endpoint were analyzed (Table 2). The median (1st, 3rd quartile) time taken to reach from gavage feeding to full oral feed in the Nifty cup group was 5 (2, 11) days versus 6 (4, 11) days in the Katori-spoon group (p = 0.2). Both the groups achieved full oral feeds at similar postnatal age (29 [16, 36] versus 28 [16, 42], p = 0.5).
Comparison of Outcomes Between Nifty Cup and Katori-Spoon Feeding Groups
Bold values indicates statistical significance (p < 0.05).
Chi-square or Fisher's exact test for categorical outcomes. Independent sample Student's t test for normal distribution and independent sample Mann–Whitney U test for skewed distribution.
OFC, occipitofrontal circumference.
We did a prespecified linear regression analysis for time to full oral feeds after adjusting for gestational age, birth weight, and PMA at enrolment. These variables were chosen a priori for adjustment because they can directly impact the feeding skills of the infant. After adjusting for these variables, we did not find any significant effect of the intervention group (Nifty cup) on time to full oral feeds (Table 3). As expected, gestational age and PMA have significant impact on time to full oral feeds.
Regression Analysis for Time to Full oral Feeds (in Days)
CI, confidence interval.
The primary investigator (PI) directly observed a median (1st, 3rd quartile) of 19 (10, 27) feeding sessions per infant and assessed the duration of feeding sessions and spillage based on the data recorded during these sessions. The infants fed with Nifty Cup were able to finish their feeds much faster than the Katori-spoon group in the PI observed sessions (12 [13, 13] versus 16 [15, 17] minutes, p < 0.001). Similar observations were made in caregiver-recorded sessions (Table 2). There was no significant difference in milk spillage. Infants in the Nifty cup group reached full direct breastfeeds earlier than those in the Katori-spoon group (mean difference = 12.6; 95% confidence interval [CI]: 4.3 to 20.8 days, p = 0.003). However, there was no significant difference in the proportion of infants reaching full breastfeeding by 40 weeks PMA (89% versus 74%, p = 0.08).
Infants in the Nifty cup group had significantly fewer episodes of vomiting (p = 0.023) than those in the Katori-spoon group, but there was no difference in other adverse outcomes, including mortality. Both groups showed excellent compliance with the assigned interventions (96.2% versus 94.3%). There was no significant difference in weight or occipitofrontal circumference at discharge. The infants in the Nifty cup group were longer at discharge; however, the length gain was not different (mean difference: 0.05 cm; 95% CI: −0.82 to +0.93, p = 0.9).
Subjective assessment
Using a structured questionnaire, we sought a subjective assessment of Nifty cup use from nurses and caregivers. Responses were recorded on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree” (Fig. 4). As nurses had experience using both interventions (Nifty cup and Katori-spoon), questions addressed to them were regarding the comparison of the Nifty cup with Katori-spoon. Since caregivers were exposed to only one device (either the Nifty cup or Katori-spoon), we sought responses regarding the Nifty cup only from them. Twenty nurses were interviewed at different time points, mainly during the second half of the study.
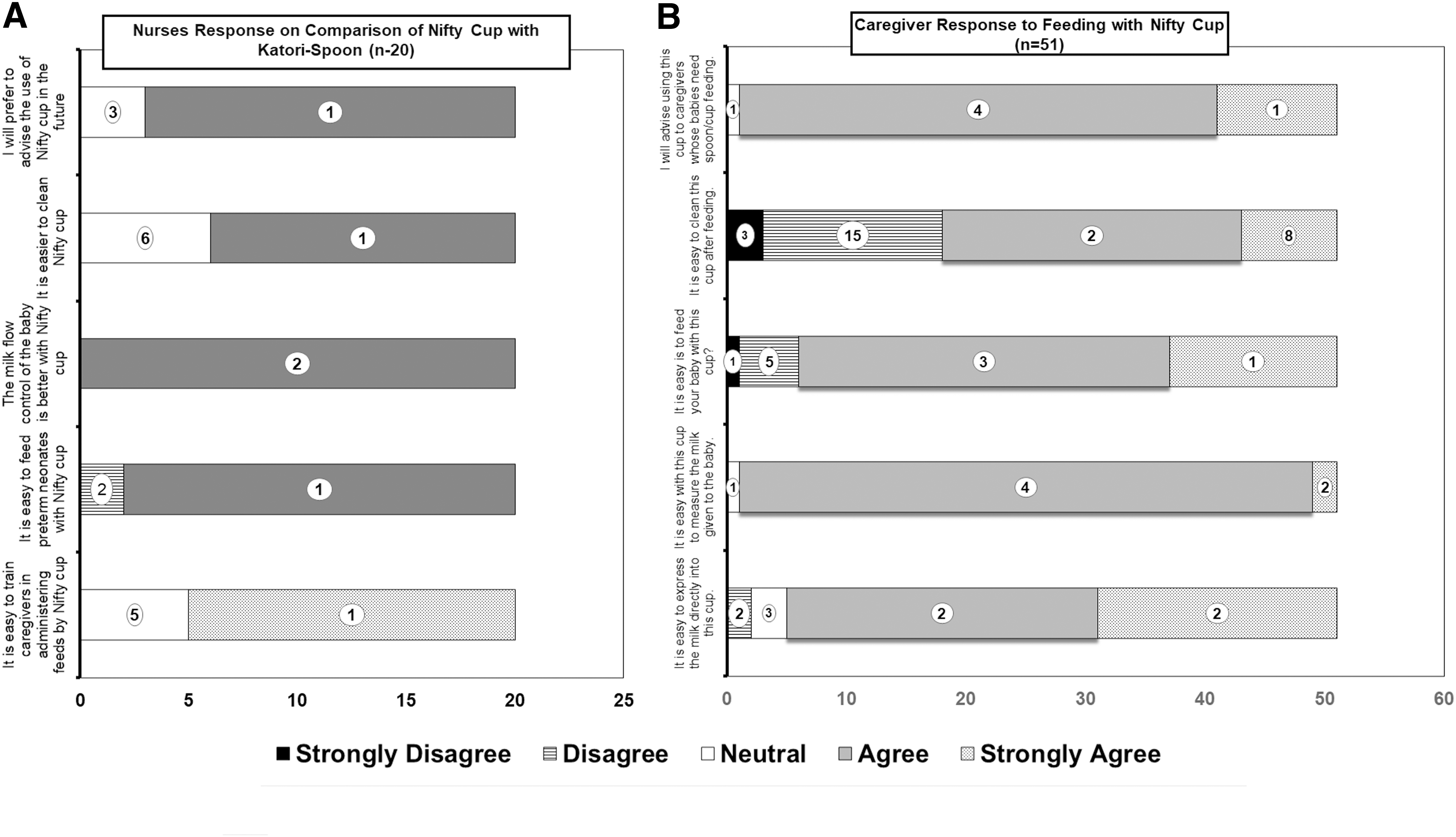
Most nurses felt that feeding with a Nifty cup was easy as it had better control of milk flow to the baby, and hence, it was easy to train the caregivers. Most said they would recommend this device over the Katori-spoon for babies eligible for oral feeding. We interviewed 51 mothers/caregivers in the Nifty Cup group. Most felt that it was easy to express milk directly in the cup and give measured feeds to the baby. Owing to ease, most (98%) said they would advise using this cup for eligible babies. However, a significant proportion (36%) felt that cleaning the cups was difficult.
Discussion
We did not find a statistically significant difference in the time to full oral feeding between the Nifty cup and Katori-spoon feeding groups. Hence, we could not prove the hypothesis that feeding with a Nifty cup helps achieve full oral feeds earlier in preterm infants. However, we observed that the infants fed with the Nifty cup took a relatively shorter time to complete their feeds and achieved full breastfeeding earlier than the Katori-spoon group. Moreover, there were fewer episodes of vomiting/regurgitation with the Nifty cup feeding than with Katori-spoon feeding. Contrary to our assumption, there was no significant difference in milk spillage. On subjective assessment, nurses and caregivers felt that milk expression, measurement, and feed administration were easy with the Nifty cup. However, many nurses and caregivers felt that cleaning the cups was difficult. Despite this limitation, 85% of the nurses and 98% of the caregivers recommended their use.
Nifty Cup is a relatively new device and has not been much tested in clinical settings. Previously, McKinney et al compared it with a medicine cup in an RCT, although they focused more on the acceptability of the cup among mothers. 5 No study has compared the Nifty cup with Katori-spoon, which is commonly used in India. McKinney et al's study found a positive response toward the Nifty cup. 5 Likewise, in Index study too, most mothers felt it was easy to express, measure, and feed the baby with the Nifty cup.
A significant advantage is that the same cup can be used for these three purposes, thereby decreasing the risk of contamination. Although milk expression is easy in Katori, the measurement is challenging and requires an additional syringe and pouring milk back and forth into Katori. Contrary to beliefs and subjective feedback and similar to McKinney et al, we also did not find a significant difference in spillage. 5
In another study from South India, McKinney et al compared the Nifty cup with the paladai. 6 They found that compared to the paladai, the Nifty cup use was associated with less spillage, regurgitation, gagging, and injury. Hence, most caregivers and nurses preferred the Nifty Cup to Paladai. In our study, the Nifty cup group also had less vomiting, although there was no significant difference in spillage. In addition, like previous study, in this study also, the nurses preferred Nifty cup over the Katori-spoon in almost all aspects. Also, like McKinney et al in index RCT, the infants in the Nifty group took relatively less time to finish their feeds, probably owing to better milk flow control coupled with active suction efforts exerted by the baby.5,6
Previous studies have not investigated the effects of Nifty cups on breastfeeding. In the index study, the Nifty cup group achieved full breastfeeding earlier. A possible explanation for this early transition is the cup design. In the Nifty cup, the reservoir and flow channels allow the infant to lap milk rather than pouring it into their mouth, and the infants can control the pace and flow of milk. This may help to establish good sucking and coordinated swallowing, a prerequisite for breastfeeding. However, as for any new device, mothers and nurses need training on Nifty cup use. In our initial experience, caregivers tended to press the Nifty cup, which led to spillage. However, with training and experience, spillage decreased over time.
In addition to providing positive feedback on its ease of use, our study adds an important point to its cleaning. The cup must be cleaned thoroughly before boiling or autoclaving. One-third of the mothers felt that cleaning the Nifty cup (more so the bottom) was challenging. A similar proportion of nurses also felt that it was more difficult to clean the cup compared to Katori. Therefore, there is a potential need for modification in cup design to make it easier to clean and improve user experience.
This study is the first to provide evidence comparing the Nifty cup and Katori-spoon for feeding preterm infants and provides both objective and subjective assessments. This study has many limitations. Due to the nature of the intervention, it could not be blinded. As the mothers used only one intervention, we could not compare their subjective assessments of the two feeding modes. However, nurses who used both devices favored Nifty Cup. The spillage might not have been estimated very accurately, more so in the Katori-spoon group, where the sideways spillage is greater.
Despite the above limitations, the Nifty cup seems to be a promising device for oral feeding with the possible advantages of lesser vomiting and early transition to direct breastfeeding. Previous studies and reviews suggest that difficulty in milk expression, increased time spent on feeding infants, and excessive spillage during feeding are important barriers to establishing Kangaroo mother care and early discharge.8,9 Nifty cup may be able to mitigate some of these barriers.
Conclusions
We conclude that feeding preterm infants with a Nifty cup does not affect the time to reach full oral feeds. However, compared to Katori-spoon feeding, it helps achieve full breastfeeding earlier. In addition, nurses and caregivers found the Nifty cup easier to use.
Footnotes
Authors' Contributions
N.G., G.K., J.K., and P.K. conceptualized the study design. N.G. and S.S. applied the intervention and collected data. J.K. and P.K. performed the data analysis. J.K. drafted the article. N.G., G.K., S.S., and P.K. critically reviewed and revised the article. All the authors agree with the final version of the article and are accountable for all aspects.
Data Sharing Statement
Individual de-identified patient data will be made available immediately after publication to researchers who provide a methodologically sound proposal for meta-analysis of individual participant data. Proposals should be directed at ![]() . To gain access to the data, requestors will need to sign a data-access agreement.
. To gain access to the data, requestors will need to sign a data-access agreement.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.