
Abstract
Introduction:
This prospective longitudinal study examined changes in milk sodium concentration (Na) and sodium:potassium ratio (Na:K), microbiological culture, milk production, and breast health in relation to mastitis after preterm birth.
Methods:
We studied women who gave birth at 29–34 weeks of gestation in a tertiary obstetric hospital in Perth, Western Australia. Milk samples, 24-hour milk production, and breast health data were collected every second day to day 10 postpartum, then every third day until infant discharge from the neonatal unit. Milk Na and K were measured at point of care (POC) using handheld ion selective meters, and Na:K calculated. Cultures were performed on postnatal days 8, 13, and every 6 days thereafter. For episodes of mastitis, milk was cultured at onset, and Na and Na:K measured daily until resolution. Women were followed up at 4 and 8 weeks postpartum.
Results:
In a sample of 44 women, 4 mastitis cases were detected in 3 women during their infants' neonatal stay; all had elevated milk Na and Na:K that resolved within 48 hours; 2/4 experienced reduced milk production and 1/4 had heavy growth of Staphylococcus epidermidis. A further 2 mastitis cases were reported in 39 women followed up to 8 weeks postpartum. Four women had elevated milk Na and Na:K without clinical signs of mastitis; three also had reduced milk production.
Conclusions:
POC testing of milk Na and/or Na:K may offer a useful indicator of breast health. Mastitis may cause an acute reduction in milk production regardless of the presence of culture-positive infection.
Introduction
Human milk (HM) is critical to the health of preterm infants as it prevents or reduces the severity of many diseases and developmental impairments associated with preterm birth. When compared with preterm infant formula, feeding of mother's own milk (MOM) during the neonatal nursery stay is associated with significant reductions in the risk and severity of retinopathy of prematurity 1 and necrotizing enterocolitis, 2 with a dose–response effect noted. 3 Feeding of MOM has advantages over pasteurized donor HM as pasteurization destroys enzymes and microbes and reduces many HM bioactive factors. 4
Low milk production is more common after preterm birth and is associated with shorter breastfeeding duration.5,6 Early postpartum factors contributing to low milk production include infrequent and/or ineffective breast expression and delayed secretory activation.7,8 Furthermore, mastitis, a painful inflammatory breast condition, may reduce milk production and is associated with lower rates of nonexclusive breastfeeding 9 and early weaning. 10 Predisposing factors for mastitis, such as breast pump use, latching difficulties, and stress, are prevalent after preterm birth. 11 While rates of mastitis are similar between women who birthed at term and at 34–37 weeks of gestation, 12 the incidence after birth <34 weeks of gestation is unknown.
Mastitis can potentially reduce 24-hour milk production volume and therefore MOM availability for preterm infants. Milk sodium concentrations (Na) and sodium-potassium ratio (Na:K) are elevated before secretory activation, 13 and during subclinical and acute mastitis.14,15 Beyond secretory activation, Na >16 mmol/L and Na:K >0.616 or >1.015–17 are considered indicative of mastitis. Measures of these biomarkers have largely been limited to the laboratory setting, with Na:K used as it resolves the issue of differing aqueous and fat proportions observed in milk samples collected from breasts of differing degrees of fullness. 18 Furthermore, Na:K is positively associated with immune markers in milk, indicating increased mammary epithelial permeability. 17 Point-of-care (POC) testing of HM has recently been shown to be accurate in the diagnosis of mastitis in term breastfeeding dyads, 19 and may aid the confirmation of mastitis after preterm birth.
Aims
The primary aim of the study was to determine whether elevated milk Na and Na:K measured at POC were associated with mastitis in mothers of preterm infants.
Secondary aims included determination of the following:
the incidence of mastitis in the first 8 weeks after preterm birth, whether an acute reduction in 24-hour milk production volume is associated with mastitis, and causative organisms associated with mastitis in women after preterm birth.
Materials and Methods
Design
An observational study of milk Na and K, Na:K, microbiological count and culture, symptoms of breast inflammation, and 24-hour milk production was conducted in postnatal women after preterm birth. Serial milk sampling and Breast Health Questionnaires (BHQ) were completed throughout the infant's neonatal unit stay, with daily data collection performed during episodes of mastitis. Telephone follow-up interviews were conducted at 4 and 8 weeks postpartum to determine the prevalence of mastitis.
Setting
The study was conducted in the neonatal unit of King Edward Memorial Hospital, Perth, Western Australia, between October 2017 and April 2019.
Participants
Mothers of infants born between 29 and 34 completed weeks of gestation were identified from the neonatal unit admission register and screened for eligibility. We included women ≥18 years of age who were expressing milk for their infants and intended to visit their infant daily. Routine pumping practices in the neonatal unit included provision of an electric breast pump and instructions to perform double pumping six to eight times in 24 hours. Study exclusion criteria included women who were non-English speaking, required hospitalization beyond routine postnatal care, or had complex health and/or psychosocial issues that prevented regular breast expression and/or daily visiting to the neonatal unit. Eligible participants were provided verbal and printed study information within 48 hours of birth and invited to provide written informed consent. A background questionnaire was completed at the time of recruitment.
Sample size determination was based on the primary aim of the study, that is, to determine whether elevated Na or Na:K is associated with mastitis after preterm birth. Relationships between elevated Na and Na:K and breast symptoms, positive microbiology culture, and acute reductions in 24-hour milk production volume of the affected breast/s were also examined. A mixed binomial model was planned with repeated measurements of Na and Na:K over an average of 2.5–3 weeks and separate evaluations of breast symptoms, microbiological culture, and 24-hour milk production. It was estimated that 62 participants were required to ensure a 95% chance of seeing at least 2 cases of elevated Na:K, as calculated using a simulation model with α = 0.05 to a power of 95%.
A secondary aim of the study was to examine the incidence of mastitis after preterm birth. Recruitment of 65 participants would allow for estimation of the true incidence (within 95% confidence interval) in this population, based on an estimate of ∼20% developing mastitis over 8 postpartum weeks. 20
Measures
Serial milk sampling for Na and K analysis and BHQ were completed every second day from days 2 to 10 postpartum, then every third day until infant discharge from the neonatal unit. Sampling for microbiological culture was performed on days 8 and 13 postpartum, and every 6 days thereafter. Researchers met with participants in the neonatal unit and sampled milk at cotside, or in a private room according to the participant's preference. When unable to meet, participants collected samples during a hospital visit and samples were stored in a research freezer at −20°C for later analysis.
We considered mastitis as acute breast inflammation (pain ± erythema ± systemic symptoms) occurring after day 6 postpartum, due to delayed secretory activation being common after preterm birth. 21 Mastitis cases were sampled for microbiological analysis on the day of onset; Na and K analysis and BHQ were completed daily from the day of onset until 48 hours after resolution of symptoms.
Breast Health Questionnaire
The BHQ, adapted from the work of Fetherston et al., 15 provides a numerical expression for breast inflammation symptoms and records the 24-hour milk production for each breast, breast expression frequency, and sensation of breast fullness before expression. Multiple choice or binomial responses are required for each breast, with items relating to pain, inflammation, and systemic symptoms, with higher scores indicating poorer breast health.
Participants recorded expression volumes for left and right breasts separately in a breast expression diary. As breastfeeding was typically initiated >34 weeks of gestation and breastfeeding frequency was infrequent with low milk transfer, 22 the 24-hour expression volume was considered indicative of 24-hour milk production for each breast in the early postpartum weeks.
Milk sample collection
To minimize contamination, participants were asked to avoid breast expression, breast pad, and topical nipple cream use for 2 hours before microbiology sample collection, which was performed before biochemistry sample collection. The nipples and areolae were disinfected with 70% isopropyl alcohol and 1% chlorhexidine swabs (Briemar, Koo Wee Rup, Australia) and allowed to air dry. Hand expression of samples was performed by the participant or the researcher according to participant preference, with the first two to four drops discarded onto a sterile gauze swab (Multigate Medical Products Pty Ltd., Villawood, Australia). For Na and K analyses, 3 mL samples were collected in 5 mL polypropylene tubes (Techno-Plas Pty Ltd., St Marys, SA, Australia). For microscopy and culture analyses, 1 mL samples were hand expressed into a 15 mL beveled base polypropylene tube (Sarstedt AG & Co., Numbrecht, Germany).
A home milk sampling pack was provided at recruitment with instructions for breast disinfection, collection, storage, and transport of milk samples to allow for sampling and data collection when the onset of mastitis occurred at home.
POC analysis of milk Na and K concentrations
Milk Na and K were measured using handheld ion selective meters, B-722 LAQUAtwin Compact Sodium Ion Meter™ (Horiba®, Japan) and B-731 LAQUAtwin Compact Potassium Ion Meter (Horiba). These meters have been validated for use in the measurement of HM Na and K. 18 After calibration, 300 μL samples were assayed in duplicate. Electrolyte concentrations were converted to mmol/L by dividing the concentration (ppm) by the relevant atomic weight. Duplicate results were averaged and used to calculate Na:K.
Microbiological analysis of milk bacterial count and culture
Milk samples were plated onto Columbia agar supplemented with 5% horse blood (Oxoid) to culture Staphylococcus and Streptococcus species. A cysteine lactose electrolyte-deficient agar medium (PathWest Medical Laboratory WA Media, Perth, Australia) was used for all other bacterial species as per standard operating procedures. Samples were incubated at 37°C for 24 hours and single colonies assessed. Matrix assisted laser desorption ionization (MALDI-ToF) Mass Spectrometer (MALDI-ToF MS; Bruker Corporation, Billerica) was used to identify cultured bacterial organisms. 23 Laboratory staff were blinded to whether samples were from mastitis or healthy cases.
This project was approved by the Women and Newborn Health Service Ethics Committee (Ref. RGS103). It was not possible to blind researchers to mastitis status of the participants. However, use of standardized breast health questions, blinding of microbiology laboratory staff, quantitative measures of milk Na, K, and Na:K, and a prospective study design were used to minimize bias.
Statistical analysis
Analysis was limited to descriptive statistics as the required sample size was not achieved for the planned mixed binomial model. Microsoft Excel for Mac (2018) was used for analyses including mean, median, standard deviation, range, and interquartile range. Milk analysis results, milk production, and BHQ scores were categorized before statistical evaluation. Milk Na >16 mmol/L was tested for association with mastitis. Figures were made using R Studio Team. 24
Results
Of the 332 mothers screened for eligibility, 46 consented to participate in the study. Recruitment was undertaken by the second author. Achievement of the required sample size (N = 65) was due to an unexpected low recruitment rate and time frame limitations.
Data and samples were obtained for 44 mothers and their 48 infants (38 singletons, 5 sets of twins, see Table 1). Two participants withdrew due to time constraints, but agreed to inclusion of their data in the analysis. Six participants were uncontactable at 8 weeks, leaving 38 participants followed up to 8 weeks postpartum (Fig. 1).
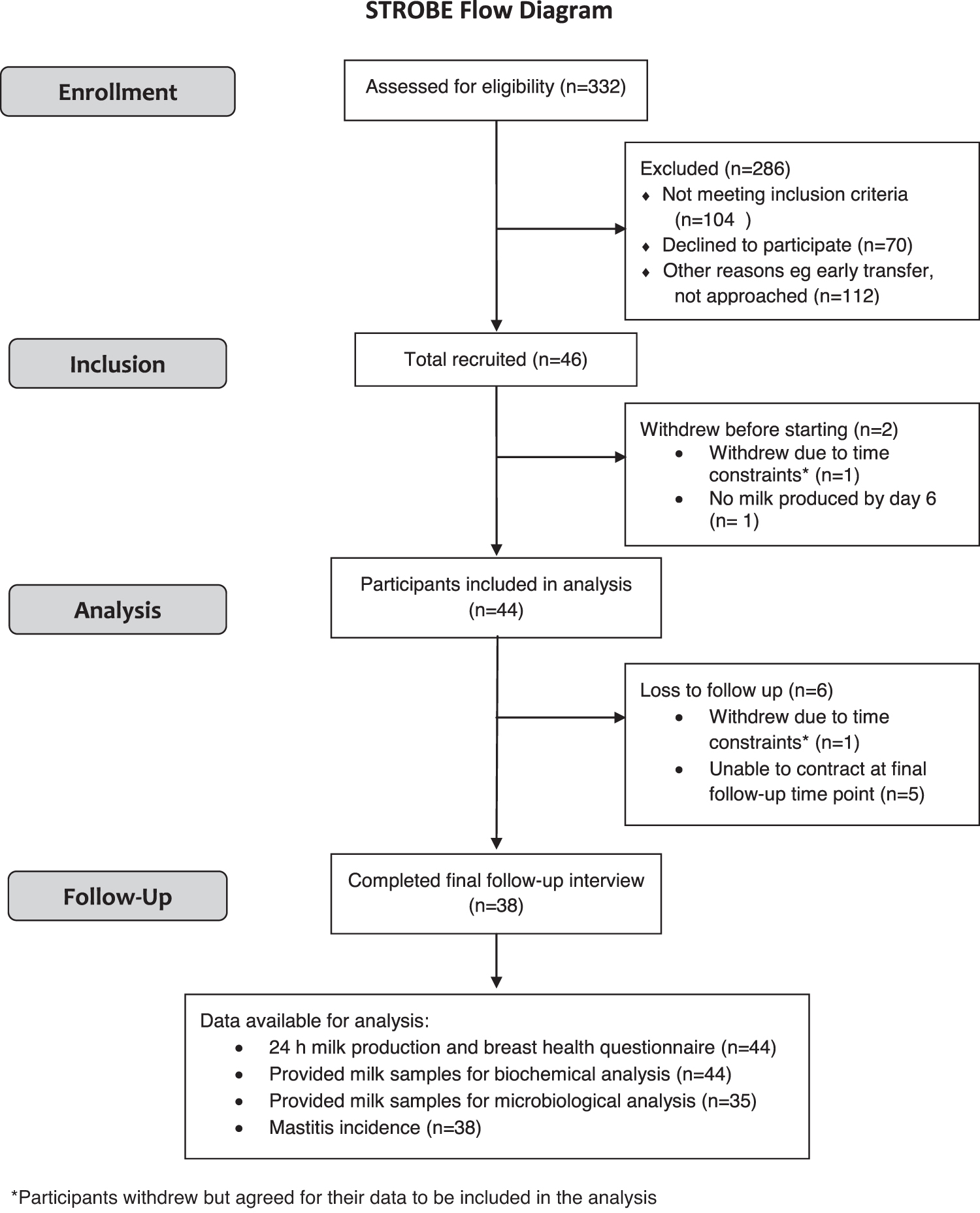
STROBE flow diagram.
Characteristics of Participants
SEIFA index (Socio-Economic Indexes for Areas) categorizes Australian postal area codes by relative socioeconomic advantage or disadvantage with index <3 indicating most disadvantaged and >7 indicating least disadvantaged areas.
Missing data, n = 2.
Missing data, n = 1.
SD, standard deviation.
A total of 677 milk samples (338 paired samples from 44 mothers) were collected for electrolyte concentration analysis, with 611 samples collected from 41 healthy participants. Another 66 samples were collected from 3 participants who experienced mastitis during their infant's neonatal unit admission, including samples collected at scheduled time points and daily over the course of mastitis episodes. Milk sample collection was omitted in some instances due to the inability to express colostrum, prioritization of low milk production to the infant, maternal illness, or unavailability. Approximately 10% of samples were stored at −20°C before initial analysis, with all other Na and Na:K analyses performed on fresh samples.
Mastitis and milk Na:K, Na concentrations
For the four episodes of mastitis detected in three participants during their infant's neonatal unit stay, elevated Na:K and Na were observed on the day of onset for three cases, and on the second day for one case. In three episodes Na:K normalized within 48 hours of onset, while in one episode (bilateral mastitis), both Na:K and Na remained elevated until the sixth day despite resolution of symptoms (Fig. 2).

Milk sodium (Na) concentration and sodium:potassium ratio (Na:K) over the course of mastitis episodes. “Pre”: last value recorded before the onset of mastitis. “Day 1”: onset of mastitis. The
Elevated Na and Na:K were identified in 17 participants in the absence of breast inflammation; 14 on day 2 postpartum, consistent with colostrum or transitional milk. Bilateral elevated Na and Na:K and continued low 24-hour milk production volumes with no breast inflammation (BHQ score = 0) were observed in five participants on day 4, one on day 6, and two on day 8, likely indicating delayed secretory activation. The latter two cases had persistent elevated Na and Na:K and low milk production volumes with no breast symptoms; up to day 16 postpartum for one participant who could not provide subsequent milk samples due to infant transfer, and unilaterally up to day 19 postpartum for the other where Na and Na:K then normalized, and milk production increased.
One participant had a single episode of bilateral elevated Na and Na:K, no breast symptoms, and a full (combined) milk production of 840 mL/24 hours on postnatal day 10, and one had unilateral elevated Na:K but normal Na, no breast symptoms, and an unchanged milk production on postnatal days 28 and 32.
Three participants reported transient breast pain (<3 hours) with no inflammation at 13, 31, and 34 days postpartum; one participant reported an elevated temperature and reduced milk production. As the participants and/or clinical staff did not consider the symptoms to be indicative of mastitis, they did not inform the researchers until the next routine data collection time point. Subsequent Na:K and Na levels were not elevated.
Incidence of mastitis
Of the 38 participants followed up to 8 weeks postpartum, 3 experienced a total of 4 symptomatic mastitis episodes during their infants' neonatal unit stay that presented at 13 to 22 days postpartum (Table 2). A further two participants reported three episodes between 4 and 8 weeks, and so, milk samples were not available for these cases. Of those reporting mastitis during their infant's neonatal unit stay, one participant had two episodes of mastitis: the right breast at day 13, which resolved before the onset of mastitis in the left breast at day 20. One participant had unilateral mastitis, and another had bilateral mastitis. The incidence rate per episode of mastitis was 18.4% (7 episodes per 38 participants) and per participant 13.2% (5/38 participants) up to 8 weeks postpartum.
Breast Health and Milk Na and Na:K Characteristics for Affected Breast on the Day of Onset of Mastitis, and for Bilateral Breasts of Participants Without Mastitis During Their Infants' Neonatal Unit Admission
One participant had bilateral mastitis.
BHQ, Breast Health Questionnaire.
Mastitis and milk production
The three participants who developed four episodes of mastitis during their infant's neonatal unit stay had combined premastitis 24-hour milk productions of 695 and 700, 1,200, and 1,240 mL. Of the four episodes, two were associated with acute reductions in milk production of 33–40% in the affected breast that recovered within 5 days of onset (Fig. 3).
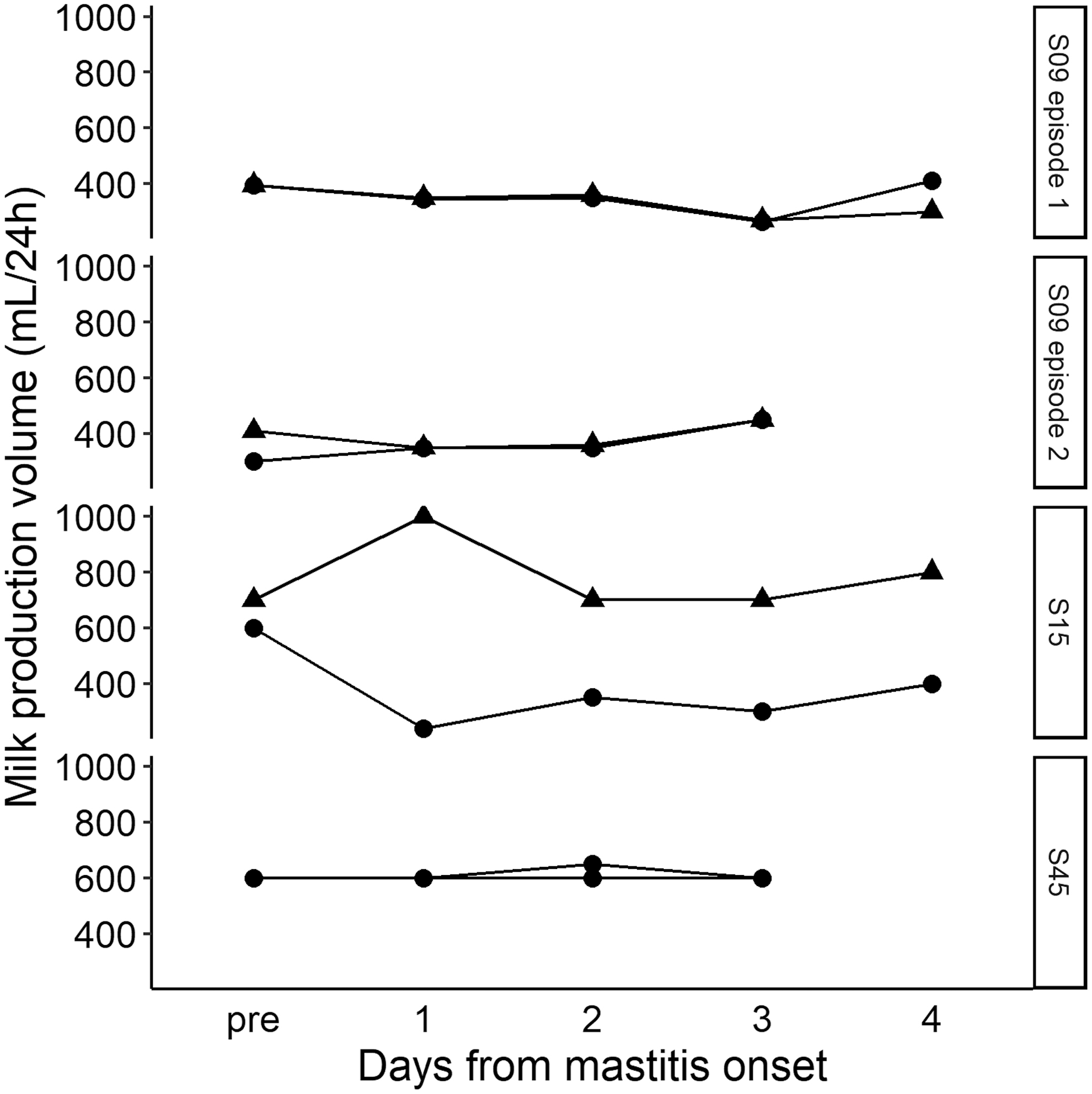
Twenty-four-hour milk production volumes (per breast) in women with mastitis. “Pre”: last value recorded before onset of mastitis. “Day 1”: onset of mastitis. The
Causative organisms associated with mastitis
Of samples collected on the day of mastitis onset, only one had significant growth (>105 CFU/mL) of Staphylococcus epidermidis from the affected breast. This species was isolated in all other mastitis samples at 104 to 105 CFU/mL. Some participants with no symptoms of mastitis also had significant growth of Staphylococci species (Supplementary Table S1), including Staphylococcus aureus.
S. aureus was isolated from four participants; one had recently recovered from infective mastitis with S. epidermidis, one had transient mild breast pain associated with physiological engorgement, and two had no breast symptoms. S. aureus was identified in one breast initially for three of the four participants, with later samples showing bilateral colonization (Supplementary Tables S1 and S2). None of the participants who became colonized with S. aureus reported breast symptoms or mastitis up to 8 weeks postpartum. In addition, asymptomatic participants had heavy growth of S. epidermidis (n = 11), Staphylococcus warneri (n = 1), and Pseudomonas koreensis (n = 1) (Supplementary Table S1).
Discussion
For the first time in the preterm population, our study findings indicate that mastitis after preterm birth is associated with elevated milk Na and Na:K, as measured at POC, confirming physiologic changes previously seen in term mothers with mastitis. The incidence of mastitis cases in this study was 13.2%, with 7 episodes (in 5 of 38 participants) occurring within 8 weeks of birth. Acute reductions in milk production were observed in two of four mastitis cases, with evidence of bacterial infection detected in one case. Significant growth of Staphylococcus species was also found in participants with no clinical signs of mastitis (Supplementary Table S1).
Elevated milk Na and Na:K were detected in all four mastitis cases. A further four cases of elevated Na and Na:K detected beyond day 6 postpartum were not associated with pain or breast inflammation, as indicated by BHQ scores of 0; three had reduced 24-hour milk production. These findings suggest that POC measurement of milk Na and Na:K may be useful in identifying and addressing delayed secretory activation 13 and subclinical mastitis 14 as well as unexplained low milk production. Indeed an elevated milk Na:K on day 7 postpartum has been associated with early breastfeeding cessation due to perceived low milk supply. 25 As all milk samples with elevated Na also had elevated Na:K, it is possible that a single POC Na measurement may provide a faster and simpler indicator of breast health status than Na:K.
Quantitative POC assessments of breast health may be particularly useful in the neonatal unit setting where mothers of preterm infants are at increased risk of poor health but also less likely to access postnatal care and support. 26 For example, POC testing may be used to rapidly confirm or exclude mastitis in women presenting with breast pain without systemic symptoms, to investigate subclinical mastitis as a possible cause of reduced milk production, and to a monitor the progression of delayed secretory activation.
We observed a prevalence of 13.2% during the first 8 weeks after preterm birth <33 weeks of gestation, that is similar to rates reported in first 6 months after term birth (17–25%), with most occurring within 8 weeks of birth. 11 Evidence for the prevalence of mastitis after preterm birth is limited to a report of similar rates of mastitis in the first 4 weeks after birth for mothers of late preterm infants (birth gestation 34–36+6 weeks) and of term infants. 12 As our study findings are limited by a reduced statistical power due to an inadequate sample size, we cannot be fully confident of our reported prevalence of mastitis after preterm birth. We were unable to achieve the desired sample size due to unusually low admission rates over the study period, and lack of staff to continue the project beyond the time frame of the researcher's master's program.
Several risk factors for mastitis are more commonly associated with preterm birth including cesarean birth, prolonged use of a breast pump, maternal–infant separation >24 hours, delayed secretory activation, latching difficulties, and use of a nipple shield.11,27 Conversely, low milk production is also more prevalent after preterm birth.6,28 Thus, in the neonatal unit setting, professional lactation advice regarding expression frequency may minimize milk stasis, a precursor to mastitis, and increase milk production.
For two of four monitored mastitis cases, the affected breasts had transient reductions in 24-hour milk production of 135 mL (33%) and 360 mL (40%). While documented in the dairy science literature, quantitative measures of reduced milk production associated with human lactational mastitis have not been reported. Reduced HM lactose during mastitis may be considered a proxy indicator of downregulated milk production. 15 Bovine studies indicate that mastitis induces the plasminogen activator of mammary epithelial cells to activate the plasminogen–plasmin system; proteolysis of β-casein produces β-casein 1–28 fragments that downregulate milk secretion. 29 It is unclear whether the plasminogen–plasmin system acts by the same pathway to alter HM production, and under what conditions, and warrants further investigation.
Mastitis is an inflammatory breast condition that may be complicated by infection. Previous studies have characterized mastitis by the presence of an increased milk bacterial load, dysbiosis, and breast inflammation.15,30 The bacterial load of HM ranges from 103 to 105 CFU/mL, with >105 CFU/mL bacteria considered indicative of infection. 31 Microbiological examination of our mastitic milk samples showed heavy growth (>105 CFU/mL) of S. epidermidis in only 1/4 (25%) cases. However, 12 participants with no breast or systemic symptoms, and 3 participants with transient breast pain and no visible inflammation also had levels of bacterial growth indicative of infection (Supplementary Table S1).
Similarly, S. aureus has been described as one of the most common causative agents of mastitis and has been reported in 32–44% of mastitis cases, and in up to 17% of healthy breastfeeding women.32,33 We found heavy growth of S. aureus in 3/35 (9%) of asymptomatic participants, and growth 103 to 105 CFU/mL in one participant after the resolution of mastitis (Supplementary Table S1). The range of symptoms and bacterial profiles observed support current understanding of a breast health continuum, with many factors contributing to prevention, or to progression to acute bacterial mastitis. 34
The HM microbiome (HMM) is dominated by coagulase negative Staphylococci (CoNS) and oral Streptococci. 35 S. epidermidis is considered a part of the normal HMM, and was identified in all participants, and in 95% of samples (n = 197) (Supplementary Table S2). However, it is also considered an etiological agent of mastitis. When the HMM is disrupted, such as through the administration of maternal antibiotics, resident bacteria (most commonly Staphylococci and Corynebacterium) can overgrow. This overgrowth can lead to an inflammatory immune response and allow for the formation of bacterial biofilms, which may partially obstruct milk ducts and lead to milk stasis. 34 The formation of biofilms has been previously shown to occur with CoNS and viridans Streptococci.32,33
Further studies are needed to understand the continuum of breast health and its implications for breastfeeding mothers, particularly in terms of the prevention, diagnosis, and treatment of mastitis. From this study and others, it appears difficult to differentiate infective from noninfective mastitis with regard to clinical presentation, milk Na, and Na:K.36,37 Recent clinical guidelines indicate that strategies to reduce inflammation, prevent tissue damage, and overstimulation of milk production should be utilized, with antibiotics reserved for conclusive infective cases. 34 Alternative rapid diagnostic microbiology tools are required to detect infection as the antibiotic treatment for all symptomatic mastitis cases alters the HMM and may potentially worsen inflammatory or subacute mastitis.
Conclusions
Elevated milk Na and Na:K are detected during episodes of altered breast health, in particular in cases of mastitis after preterm birth. We also observed reduced milk production that resolved within 5 days, which may explain some instances of reduced availability of MOM for preterm infants. POC measurement of milk Na and Na:K may provide a valuable tool in evaluating breast health and the effectiveness of treatment strategies.
Footnotes
Acknowledgments
We acknowledge our participants' generous contribution of time and samples for this study. We appreciate the expert contributions of Dr. Tony Keil (Director of Pathology, Women's and Children's Health Service, Nedlands, Western Australia), Jane Bew (Scientist in Charge, Bacteriology, Department of Microbiology, QEII Network, Nedlands, Western Australia), and colleagues in planning and facilitating microbiological analyses.
Authors' Contributions
S.L.P.: Conceptualization, methodology, investigation, data curation, writing—original draft, reviewing, and editing, and supervision. E-L.A.-M.: Methodology, formal analysis, investigation, and writing—original draft. G.M.: Writing—original draft and visualization. C.T.L.: Validation and supervision. K.N.S.: Methodology, resources, and supervision. D.T.G.: Conceptualization, methodology, resources, and supervision.
Disclosure Statement
S.L.P., D.T.G., and C.T.L. receive salaries from an unrestricted research grant paid by Medela AG to The University of Western Australia. The funding body was not involved in the study design, collection, analysis and interpretation of data, writing of the article, and the decision to submit the article for publication. E-L.A.-M., G.M., and K.N.S. have no potential conflicts of interest to declare.
Funding Information
Sharon Lisa Perrella, Donna Tracy Geddes, and Ching Tat Lai receive salaries from an unrestricted research grant paid by Medela AG to The University of Western Australia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.