
Abstract
Background:
The symptoms of Dysphoric Milk Ejection Reflex (D-MER) occur just before milk release, last no more than a few minutes, and then subside spontaneously, which are characterized by a sudden and transient feeling of dysphoria, depression, sadness, or other negative emotions. These emotions may adversely affect the mother's lactation behavior and mental health, negatively influence the mother–child relationship, and even result in self-harm or suicidal tendencies in lactating women.
Case Presentation:
We reported two cases of breastfeeding mothers with D-MER who experienced unpleasant emotions during lactation. Severely affected by D-MER symptoms, the mother in the first case chose to wean prematurely after struggling for 6 months, and her symptoms disappeared after weaning. With the help of professional guidance, the mother with D-MER in the second case actively adjusted and persisted in breastfeeding until her daughter was 18 months old, after that her symptoms vanished.
Discussion:
Awareness and knowledge of D-MER are insufficient among the public and health care professionals. D-MER is not a psychological disorder but a physiological issue caused by hormones, which is different from postpartum depression. The severity of D-MER symptoms can be evaluated by the assessment tool of the D-MER spectrum. Lactating women can relieve their symptoms through self-regulation, lifestyle changes, and professional guidance and treatments.
Conclusions:
The two cases studies about Chinese women with D-MER will enrich the knowledge of D-MER, and it might suggest some directions to health care workers for exploring scientific guidance and treatments for lactating women. Because the literature and published empirical studies about D-MER are scarce, further researches on the theory and interventions of D-MER are necessary.
Introduction
The milk ejection reflex occurs when the nipples are stimulated during suckling, which promotes the smooth release of breast milk. 1 Milk ejection is a critical process for successful lactation. However, the abrupt unpleasant feelings or negative emotions that occur just before milk ejection are defined as Dysphoric Milk Ejection Reflex (D-MER) by Heise and Wiessinger. 2 The symptoms of D-MER that lactating women experience are characterized by a sudden and transient feeling of dysphoria, depression, sadness, or other negative emotions. These emotions may adversely affect the mother's lactation behavior and mental health, negatively influence the mother–child relationship, and even result in self-harm or suicidal tendencies in lactating women. 3 Many mothers feel embarrassed and guilty about their negative emotions and are reluctant to mention them. Although some mothers express negative emotions of D-MER, the symptoms are often mistakenly considered to be postpartum depression (PPD). 4
The limited published studies and stories or information shared online about D-MER show that the D-MER symptoms really exist, but the public do not know much about it. The experiences of mothers with D-MER during breastfeeding are slightly different from each other, but one thing in common is that they will experience a wave of abrupt, negative, or destructive emotions ∼30–90 seconds before the milk release, which generally lasts no more than a few minutes. The negative feelings will dissipate when the milk is released, and the baby starts swallowing it. However, it recurs when the next milk ejection occurs. The emotional response above during breastfeeding, pumping, or with spontaneous milk ejection reflex is the key characteristic of D-MER. 2
Mothers mostly describe D-MER as the following words: anxiety, sadness, nervousness, dread, emotional upset, irritability, hopelessness, a hollow feeling in the stomach, and general negative emotions. The more intense the negative emotion the mother experiences while breastfeeding, the longer it lasts. 3 According to the variable intensity of the emotional responses, D-MER is classified within a three-level spectrum: depression, anxiety, and anger. 2
The literature about D-MER is limited, and published empirical studies are scarce. Awareness and knowledge of the adverse emotional reaction of D-MER are insufficient in the public. Moreover, breastfeeding professionals also rarely recognize D-MER, and there is limited access to science popularization, treatments, and health education on D-MER. Therefore, lactating women seldom seek help willingly, which blocks their way to receiving formal guidance and treatments. 5 Accordingly, this article reports two cases of lactating women with D-MER and reviews the related research on D-MER, aiming to arouse the attention of people on D-MER and help medical staff take effective measures and intervention strategies to reduce the negative impact of D-MER on lactating women.
Case Presentation
Case 1
The participant is a 29-year-old, Chinese-speaking, primigravid woman who gave birth to a male infant at term gestation; the infant was delivered through vaginal delivery without complications. The woman had a hard time during breastfeeding. She described that the feelings such as anxiety, hopelessness, and sadness always appeared unavoidably before milk ejection, which continued for ∼2 minutes, then dissipated abruptly and recurred at the next milk ejection. She also experienced negative emotions when pumping, but the emotional response of pumping was less intensive than feeding at the breast. The intensity of her symptoms increased over time, making her feel dread about breastfeeding.
When she told such negative emotions to her family, they consoled her “it is normal for a novice mother to feel stressed.” She neither wanted to stay with her baby nor fed the baby breast milk, and several times she had the impulse to leave the baby behind. Moreover, she had never felt the feeling of other mothers saying “Breastfeeding is one of the sweetest and happiest parts of motherhood.” Worst of all, she thought that she was not qualified to be a mother or have a child. When she was told that she might be suffering from D-MER, she felt better, but she still chose to wean prematurely when the baby was 6 months old, after that her D-MER symptoms disappeared.
The participant stated that she had experienced negative feelings similar to breastfeeding in childhood. She recalled, “When I was a child, I would feel an abrupt wave of sadness and nervousness swept over me when my nipples were touched, especially while dressing/undressing or taking a shower, but it vanished quickly after several seconds. No matter how happy I was, I felt an overwhelming sense of sadness at that moment. Combined with experiences during breastfeeding, I mistakenly thought that I had psychological problems.”
Case 2
The second case is that of a healthy, 34-year-old Chinese woman with a 5-year-old son and a 3-month-old daughter. The woman delivered two children at term without complications and experienced D-MER during breastfeeding in both children. After her son was born, she was unaware that her emotional problem was caused by D-MER and did not have much experience in breastfeeding, so she stopped breastfeeding early. After her daughter's birth, she found the occurrence regularity of negative emotions, which only occurred at every breastfeeding and lasted no more than 3 minutes. Thus, she searched online for information and learned that her symptoms were D-MER and the intensity of her symptoms was moderate level. Moreover, she was relieved to learn that D-MER was just a physiological problem caused by hormones. She consulted a doctor about her emotional problems once before. However, owing to insufficient knowledge of D-MER, the doctor mistakenly diagnosed her with postpartum depression.
This time medical staff provided guidance and suggestion to her after listening attentively to her experiences. Considering that medicine could be secreted through breast milk which might be detrimental to infant's health, she refused to take medicine and chose natural and healthy ways to improve D-MER symptoms.
In the first week, this mother changed the way of breastfeeding and pumped breast milk for bottle feeding, but it did not work very well. In the second week, she reorganized her eating and found that the intake of chocolate and other desserts could relieve symptoms. However, she had to quit eating desserts because of her high body mass index. Because the woman was a fitness enthusiast before pregnancy, she tried yoga and meditation to ease her symptoms on the doctor's advice in the third week. Surprisingly, it did work, and her symptoms improved obviously. During the period, she recorded the intensity of D-MER symptoms via the D-MER intensity spectrum (Fig. 1), and the comparison between the effects of the three alleviation ways is given in Figure 2. Since then, she tried various ways to alleviate the symptoms according to information from the Internet and finally found that yoga and meditation were healthy and effective for her. She actively adjusted and persisted in breastfeeding until her daughter was 18 months old, and her symptoms vanished after weaning.
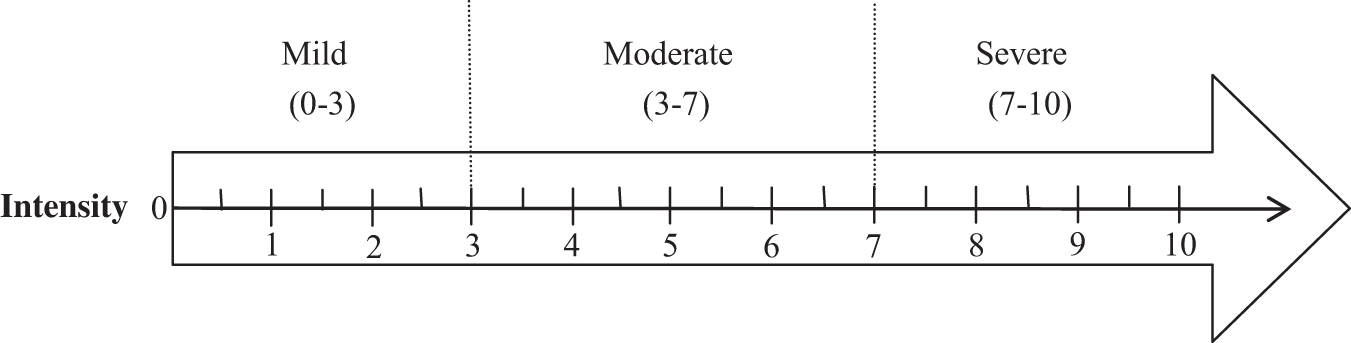
Intensity of Dysphoric Milk Ejection Reflex symptoms.
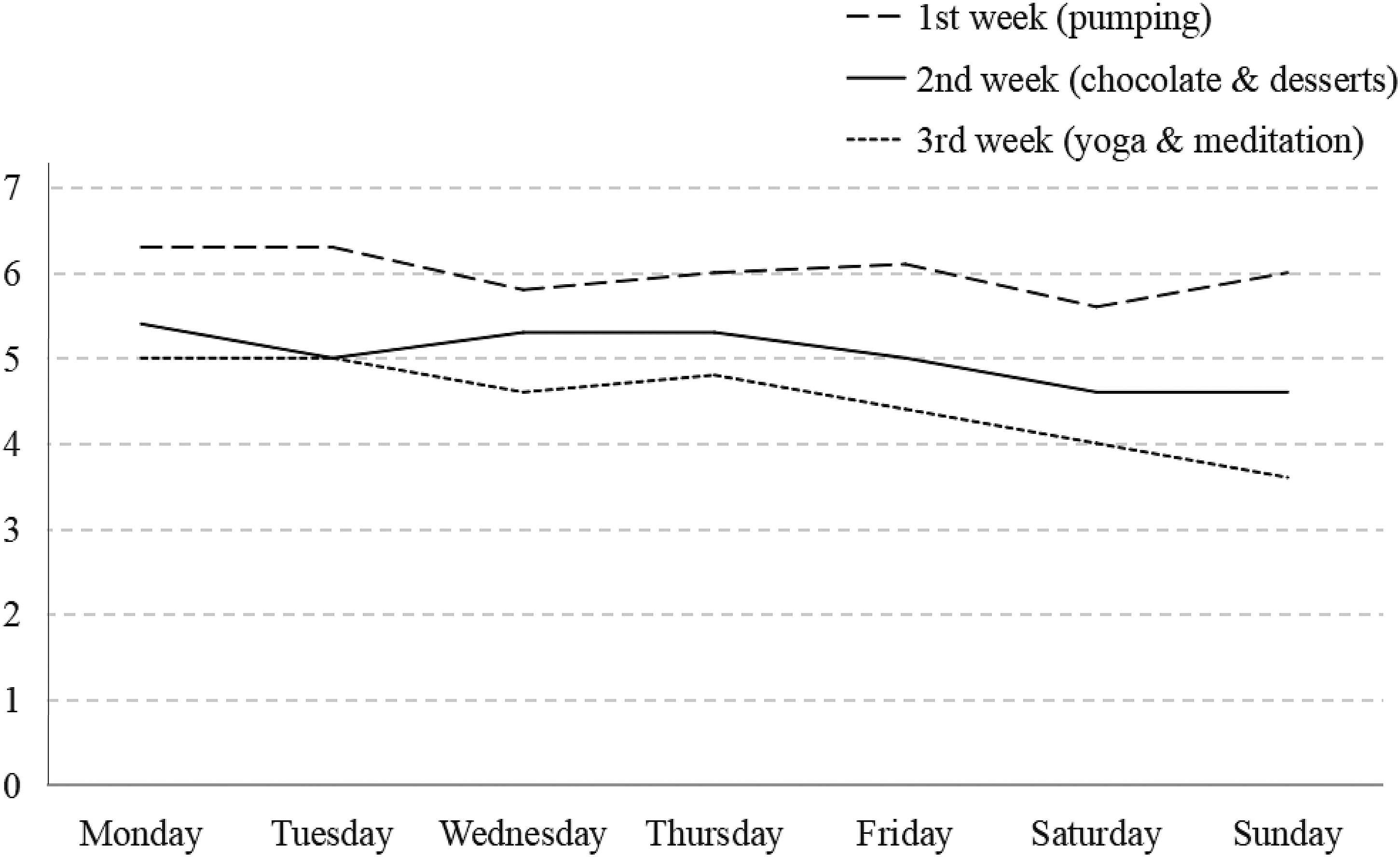
The effects of the three ways on the intensity of symptoms.
Discussion
The mechanism of D-MER
The physiology underlying the D-MER response may be relevant to hormones. The abnormal activity of dopamine possibly triggers the D-MER when the milk ejection reflex is activated; therefore, D-MER is a physiological response rather than a psychological response in lactating women. 2 D-MER is perhaps mediated by dopamine. The levels of oxytocin and prolactin both elevate in lactating women. When the milk ejection reflex is triggered, oxytocin level raises immediately to cause milk ejection, whereas dopamine levels quickly drop to let prolactin increase to cause milk production. The abrupt decrease in dopamine of some women in turn likely results in unpleasant feelings associated with D-MER. Lactating women are not usually aware of this response during breastfeeding.
However, because dopamine in women with D-MER drops too low or too fast in the central nervous system, they unavoidably experience a wave of negative emotions, which explains that negative emotional responses are attributed to abnormal dopamine activity.2,3 In addition to the dopamine factor, the negative emotions of lactating women may also be related to the following factors: increased nipple sensitivity during pregnancy, increased energy expenditure during lactation, insufficient nutrition and sleep, and hormonal imbalance. 6 Moreover, factors such as dehydration, caffeine intake, and mental stress may influence D-MER symptoms.7–9
Different from the viewpoint mentioned previously, a study summarizes the role of oxytocin, the most plausible hormone directly responsible for D-MER symptoms. 9 Oxytocin and prolactin are two hormones that release in response to breastfeeding, Oxytocin is released immediately in response to suckling, and prolactin is released more gradually to cause milk production. In the first few minutes of breastfeeding, oxytocin is released in several pulses while prolactin is still low. Prolactin is low in the first 10 minutes and then gradually rises. The symptoms of D-MER- map perfectly to oxytocin, not prolactin. The release speed and time of the two hormones suggest that oxytocin is the most plausible hormone related to D-MER.
There is no evidence as to why some lactating women experience D-MER, whereas others do not. In addition, nonlactating women, perimenopausal women, and even men have experienced similar negative emotions of D-MER when nipples are stimulated. The symptom above is dubbed “sad nipple syndrome” by some netizens, and the mechanism of this syndrome and its relationship with D-MER are not yet clear. 2
The assessment tool of D-MER
Heise and Wiessinger developed the spectrum of D-MER as a tool to evaluate D-MER symptoms. 2 Unlike the general scales with a continuum of numbers, the spectrum of D-MER divides symptoms into three distinct and different emotions (depression, anxiety, anger), and the intensity of each kind of emotion varies from mild to moderate to severe degrees. Ureño et al. revised the spectrum of D-MER. 7 The intensity of depression, anxiety, and anger are redefined with a number ranging from 1 to 10, and the higher the score, the more severe the unpleasant emotion. The intensity of 1 to 3 indicates mild D-MER, a rating of 4 to 7 indicates moderate D-MER, and the score of 8 to 10 indicates severe D-MER.
To easily record and track the D-MER intensity symptoms of participants, the D-MER intensity spectrum of this study was adapted and simplified from Heise and Wiessinger 2 and Ureño et al. 7 The simplified D-MER scale is a self-assessment tool with a continuous number from 0 to 10: mild level is lower than 3, moderate level is from 3 to 7, and severe level is ≥7 (Fig. 1). Lactating women can mark the intensity of D-MER symptoms according to their feelings. In addition, the simplified D-MER scale is just a subjective and convenient way to record mothers' feelings, it can be only used as a screening tool for the intensity of emotion and not as a formal diagnostic tool.
Differences between D-MER, PPD, and breastfeeding aversion and agitation
D-MER is different from peripartum depression (formerly postpartum, PPD) and breastfeeding aversion and agitation (BAA). PPD is depression that generally occurs after childbirth. PPD is a type of perinatal mood disorder, which is a complex mix of physical, emotional, and behavioral changes that happen in some women. To be diagnosed with peripartum depression, symptoms must begin during pregnancy or within 4 weeks following delivery. 10 BAA is a negative emotion caused by breastfeeding, it may well be both physiological and psychological, especially for women who constantly experience any activity that causes nipple pain or uncomfortable sensations. 6 The BAA symptoms are featured with anger and agitation while breastfeeding and cause irritating skin sensations. However, mothers are possibly still willing to breastfeed. Being different from D-MER, BAA can happen at any point in the breastfeeding journey. 11
Compared with PPD and BBA, the most obvious differences are that D-MER only occurs just before milk release and lasts for a short time (within a few minutes), and dissipates by the time milk actually releases. D-MER is not an affective or psychological disorder but a physiological issue probably caused by hormones. Lactating women may suffer from D-MER and other negative feelings simultaneously. 9 In a word, PPD has a very large and comprehensive literature, and there are many ways for us to learn about it. However, D-MER and BAA are still in the early stages of knowledge development, further studies are needed to fill the significant gap in the literature around D-MER and BAA. The specific characteristics and differences between D-MER, PPD, and BAA, are given in Table 1.
The Characteristics and Differences Between Dysphoric Milk Ejection Reflex, Postpartum Depression, and Breastfeeding Aversion and Agitation
BAA, breastfeeding aversion and agitation; D-MER, Dysphoric Milk Ejection Reflex; PPD; postpartum depression.
Potential effects of D-MER
Although there is lack of experimental and epidemiological research on D-MER, we have learned from limited published studies that there are potential consequences of D-MER for women. First, the benefits of breastfeeding to maternal and child health have been recognized globally, which not only promotes the growth of infants but also prevents breast cancer and ovarian cancer in women. 12 Nevertheless, some lactating women with D-MER tend to resist breastfeeding owing to the negative emotions, 4 and they might choose to stop breastfeeding reluctantly or wean early to extricate themselves from unpleasant emotions.2,7 Second, under the moral requirements of society and family for “a good mother,” the thought or action of stopping breastfeeding probably makes mothers feel guilty and shamed. 13 Consequently, some mothers continue to breastfeed even if they suffer from great pressure and negative emotions.
In addition, the negative emotions affect the close relationship between mother and infant. Some might feel worthless and do not want to stay with their babies, 14 whereas some may even have the impulse or behavior to hurt infants.5,15 Finally, women with D-MER experiencing a range of negative emotions may possibly end in depression and even result in self-harm or suicidal tendencies. 3
Alleviation and treatments in D-MER
Medical therapy
Increasing and maintaining dopamine levels may effectively reduce maternal D-MER symptoms. Medications that may increase dopamine levels and be effective at relieving D-MER symptoms for some women include Bupropion, B-vitamin complex, Pseudo-ephedrine, Rhodiola rosea root supplement, and placenta encapsulation.2,7 At present, no controlled studies have confirmed the specific effect of medical products in treating D-MER. Meanwhile, as pseudo-ephedrine and placenta encapsulation are suspected to cause drops in milk supply, the utilization of these medications should be cautious. A study shows that nicotine (smoking) can also alleviate some women's D-MER symptoms, but it is not recommended owing to its harm to health. The study also finds that chocolate intake can alleviate symptoms in some women. 2 It is possibly related to stimulating the release of endorphins in the brain that can relieve stress and make people feel good. 16
Self-regulation and lifestyle changes
D-MER symptoms might be alleviated through self-regulation and changing lifestyles. Reading books, watching TV, listening to music, aromatherapy, chatting, and other entertainment activities during breastfeeding might distract mothers' attention to symptoms.2,7 Maintaining a healthy lifestyle is important for lactating women against negative emotions. Thus, mothers should moderately increase water intake and exercise regularly, ensure adequate sleep and reduce caffeine intake.7,8 Research indicates that insulin levels may be linked to serum oxytocin. Breastfeeding may also be related to high insulin levels, and women's negative emotional symptoms can be eased by regulating blood glucose by reducing carbohydrates and increasing protein in their diet.9,17
Psychological stress is one of the key factors to affect human health, which emphasizes the necessity of relieving pressure and striking a balance between work and rest. Lactating women should find proper ways to relieve pressure and maintain an optimistic attitude, we know this helps with depression and would help here too. Mindfulness is efficacious in relieving stress, which advocates focusing on the present moment, accepting ourselves completely, and learning to not dwell on negative thoughts that float through our minds. Meditation and breathing are very important parts involved in mindfulness, the negative emotions and symptoms might be effectively relieved through meditation and proper breathing pace.9,18
Emotional support and help from family
The emotions like unhappiness, sadness, and worry in lactating women seriously affect breastfeeding, and the family plays a critical role in increasing maternal self-confidence.19,20 Although effective family support for women with D-MER has not been confirmed, the following points may help improve D-MER symptoms. Insecurity may exacerbate women's D-MER symptoms. Families and friends, who are close to lactating women, should fully appreciate what mothers have done for their infants during lactation, and it is beneficial that families give emotional support unconditionally to lactating women. 21
What is significant is the awareness of D-MER, that it is not a psychological problem but is more likely caused by the misfiring of oxytocin or the abnormal activity of dopamine. If necessary, the family members should accompany lactating women and chat with them more to create a more safe, healthy, and comfortable environment for mothers and infants. 9 In addition, research has shown that skin-to-skin contact has a strong anti-stress effect on both the mother and baby, promoting emotional bonding effectively. 22 Therefore, it may be efficacious in easing stress and anxiety for mothers to have more skin-to-skin contact with their babies.
Professional guidance and treatment from medical staff
Midwives and health professionals lack comprehensive scientific knowledge of D-MER, and many medical workers are even unfamiliar with D-MER, which has adversely affected breastfeeding-related health services. 5 To provide professional services based on the specific mental and physical needs of lactating women, health professionals should carry out more scientific research by incorporating the psychological, environmental, and cultural aspects of lactating women. Health education and guidance should be carried out for mothers with mild-to-moderate D-MER, and mothers should be encouraged to record and track the occurrence of D-MER symptoms, and focus on things that may alleviate their symptoms. Women who suffer from severe D-MER need to receive prescription treatment or other professional therapies.
Furthermore, the peer-support groups may be conducive to mothers' breastfeeding endeavors and could enable them to understand and handle their unpleasant emotions in a safe and shared environment. Apart from easing mothers' negative emotions, peer-support groups can also improve the breastfeeding rate.15,23 Therefore, professionals need to carry out peer support programs to promote the health status of lactating women.
In summary, the symptoms of D-MER may be improved through many ways. According to published research,2,7,8,24 the things and their possible effects on D-MER are sorted out and classified as given in Table 2. There are four kinds of activities (solitude, alcohol, pumping versus feeding at the breast, and dietary changes) that might have dual effects on women with D-MER. These activities may alleviate mothers' symptoms. In contrast, they may also exacerbate the symptoms of some mothers. The reason may be related to the differences in physical fitness, dietary habits, and lifestyles among lactating women. Further research and exploration are needed to investigate the specific reasons for this issue.
Things and Their Possible Effects on the Symptoms of Dysphoric Milk Ejection Reflex
D-MER, Dysphoric Milk Ejection Reflex.
Conclusions
D-MER has become a concern of the public and health care professionals. Unpleasant experiences of breastfeeding caused by D-MER may impact maternal and child health in the short and long term. Mothers with D-MER have to struggle with negative emotions alone owing to lack of awareness and knowledge about it. Moreover, because medical workers have a limited understanding of scientific and clinical knowledge regarding D-MER, it is not easy for mothers to gain access to professional guidance and treatments. Therefore, the general public should be informed of the knowledge of D-MER. First, D-MER is different from psychological disorders like PPD. The misfiring of oxytocin or the abnormal activity of dopamine may be responsible for the D-MER response in lactating women. In addition, the severity of D-MER symptoms can be evaluated by the assessment tool of the D-MER spectrum.
Mothers with mild-to-moderate D-MER can relieve their symptoms through self-regulation, lifestyle changes, and professional guidance, whereas mothers with severe D-MER need to receive professional treatments. Further researches on the theory and interventions of D-MER are necessary, and it will enrich breastfeeding knowledge and help health care workers develop systematic and scientific guidance and treatments to provide more professional and effective treatments for lactating women.
Published studies of D-MER have offered some hypotheses about the mechanism of D-MER from the perspective of hormones, and some studies have pointed out that D-MER may be effected by stress. Because some mothers with D-MER describe their emotions and feelings differently from each other, more attention should be paid to whether D-MER is affected by factors such as aspects of physiology, psychology, culture, and society except for the hormone factor. Furthermore, nonlactating women, perimenopausal women, and even men and children have experienced similar negative emotions of D-MER, the reason and its relationship with D-MER need to be proved by further studies. Finally, the unpleasant experience of breastfeeding caused by D-MER affects maternal and child health, but there is no relevant research on the intervention of it. Hence, intervention studies should be carried out on lactating women with D-MER in the future. Resolution of these issues requires the joint efforts of breastfeeding-related educators, researchers, and medical workers, so as to improve breastfeeding support services and promote the physical and mental health of lactating women.
Footnotes
Authors' Contributions
H.L. contributed to literature search, study design, investigation, data collection, analysis, article writing and editing (the whole process of this study). J.L. recruited participants, carried out adaption of the assessment tool, offered advice on analysis, and revised the article. X.L. provided supervision and suggestions for investigation and analysis, and revised the article. H.L. carried out literature search and study investigation. All authors approved the final article as submitted.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.