
Abstract
Aim:
To compare the effect of different analgesic regimens on the time to initiate breastfeeding (BF) and ambulation after cesarean section (CS).
Methods:
This prospective, double-blinded, placebo-controlled randomized study included 300 women (20–40 years of age) of the American Society of Anesthesiologists status 1 or 2 with singleton term pregnancies scheduled for CS under spinal anesthesia. Women were allocated to three groups of 100 each by computer-generated randomization. As an adjunct to 1,000 mg intravenous acetaminophen, Group 1 received 100 mg rectal diclofenac, Group 2 received 100 mg rectal tramadol, and Group 3 received rectal glycerin suppository. The time to initiate BF and ambulation was compared between different analgesic regimens and corelated with pain score.
Results:
BF (both with and without support) was initiated significantly earlier in Groups 1 and 2 as compared with control Group 3 (p < 0.001). A significantly shorter time was taken to initiate BF without support in Group 1 as compared with Group 2 (p = 0.028). The time to start ambulation (both with and without assistance) was significantly lower in Groups 1 and 2 as compared with Group 3 and in Group 1 versus Group 2 (p < 0.001). A significant positive correlation was found between the time to initiate BF with support and ambulation without assistance and postoperative pain score at 0, 1, and 6 hours.
Conclusion:
Effective post-CS analgesia affects early initiation of BF and ambulation in the immediate postnatal period. The inclusion of rectal diclofenac suppository in post-CS analgesic regimens is a promising approach to postoperative delivery care.
Introduction
Early initiation of breastfeeding (BF) and early ambulation are the two essential postpartum activities after a cesarean section (CS). Early initiation of BF, defined as the start of BF within 1 hour after delivery, is one of the key components of optimal BF recommendations by the World Health Organization. 1 It constitutes an important element of essential newborn care, has innumerable benefits for both the mother and her baby, and has been shown to decrease neonatal mortality substantially. 2 Despite these recommendations and recognized benefits, different studies demonstrate that it is not universally practiced by mothers, especially in developing countries.3–7 The global statistics suggest that only around 42% of all newborns were put to the breast within an hour of birth. 4 Early ambulation further improves BF, minimizes postoperative complications, such as venous thromboembolism, and contributes to speedy recovery after CS. 5
Post-CS pain is one of the most commonly cited reasons for late initiation of BF and delayed ambulation.6,7 Postoperative pain and stress stimulate the release of dopamine and dynorphin in the body and have an inhibitory effect on the production of prolactin and oxytocin.8,9 Moreover, pain affects the mother's functional ability, mobility, and bonding with her newborn. All these factors thereby reduce the mothers' intention and initiative to BF early. Recent guidelines recommend long-acting neuraxial opioids (e.g., morphine) and adjunctive drugs such as acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and opioids (oral or parenteral) for post-CS analgesia.10,11 However, the use of rectal NSAIDs and rectal tramadol for post-CS pain has not been much studied.12–14 The influence of pain relief in the immediate postoperative period on early initiation of BF and early ambulation following a CS is an understudied subject. The present study aimed to evaluate the post-CS pain intensity in different analgesic groups and its influence on the time to initiate BF and ambulation in the immediate postnatal period.
Materials and Methods
This single-centric, prospective, double-blinded, placebo-controlled randomized study was conducted in the department of Obstetrics and Gynecology at a tertiary teaching institute in India between September 2018 and July 2019. After approval from the Institutional Ethics Committee and obtaining informed written consent, pregnant women scheduled for CS under spinal anesthesia were recruited for the study.
Sample size
To the best of the authors' knowledge, there has been no such similar previous study so far. The sample size was calculated through power analysis determined by reviewing study by Karlström et al who determined the association between post-CS pain intensity and women's ability to BF and care of her newborn. 15 With a power of 80% (β = 0.20), confidence interval of 95%, and an error margin of α = 0.05, the sample size computed using the Open Epi program was 74. A total of 100 women were included in each group.
The inclusion criteria included singleton term pregnancy (37–42 weeks' period of gestation), age group 20–40 years, American Society of Anesthesiologists physical status classification grade I–II, and use of Pfannenstiel incision during surgery. The exclusion criteria comprised any coexisting medical condition (morbid obesity; gastric ulcers; cardiac, renal, or respiratory disease), history of chronic pain, known allergy to study drugs, any complication during surgery, second-stage CS, and subsequent use of another method of anesthesia during CS. Women were randomly allocated to one of the three groups of 100 each using a computerized random number table to receive an adjunctive analgesic drug in the form of a rectal suppository after cesarean delivery. Spinal anesthesia was administered using hyperbaric bupivacaine (2 mL [10 mg] bupivacaine 0.5% plus fentanyl citrate 0.5 mL [25 μg] intrathecally). Group 1 received 100 mg diclofenac suppository, Group 2 received 100 mg tramadol suppository, and Group 3 received glycerin suppository as placebo.
All women were given 1,000 mg intravenous (IV) acetaminophen in the postoperative recovery room, which was repeated after every 8 hours for 24 hours. Figure 1 illustrates the consort flow diagram of the study process. The mean time (hours) to initiate BF and ambulate with or without support was calculated in the three groups by monitoring the patients and by asking the patients at hourly intervals. To correlate these findings with postoperative pain, the pain assessment was performed using a 1–10 visual analog scale (VAS) [0 = no pain and 10 = worst pain) at 0, 1, 6, 12, 18, and 24 hours after the surgery (0 hours was the time of arrival of the patient to postoperative recovery room). The investigators assessing all the parameters were blinded to study group allocation. Side effects, if any, were noted. The outcome measures were:
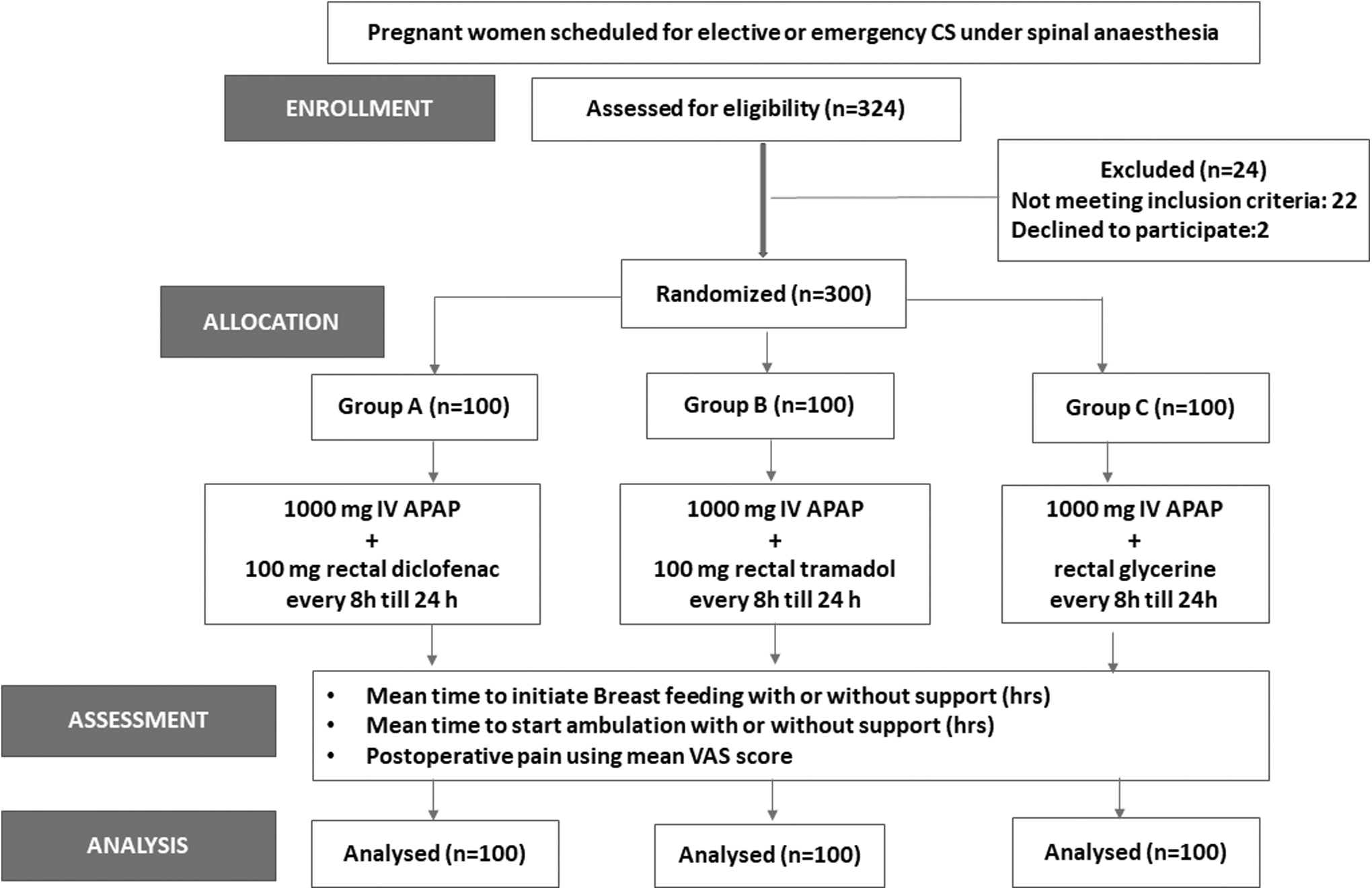
Consort flow diagram. APAP, acetaminophen; CS, cesarean section; IV, intravenous; VAS, visual analog score.
Primary outcomes
To compare the mean time to initiate BF with or without support among the three groups.
To compare the mean time to ambulate with or without assistance among the three groups.
Secondary outcomes
Correlation of time to initiate BF with or without support with VAS score.
Correlation of time to ambulate with or without assistance with VAS score.
Ethics considerations
The research was conducted in accordance with the Helsinki Declaration. Ethics approval for the study was obtained from the Biomedical Research Ethics Committee of the Pt. B.D. Sharma Postgraduate Institute of Medical Sciences, Rohtak, Haryana, India.
Statistical analysis
Data were analyzed with Statistical Package for Social Sciences (SPSS) version 22.0 (IBM Corp., Armonk, NY). Continuous variables were calculated as mean ± standard deviation or median and range as appropriate and compared with the use of the Student's t test or Mann–Whitney test. Categorical variables were calculated as a number (%) and compared using the Chi-square test or Fisher's exact test as appropriate. All tests were two-sided, and a p-value of <0.05 was considered statistically significant.
Results
The results are shown in Tables 1–3.
Demographic and Baseline Characteristics in Three Groups
Socioeconomic status classified according to modified Kuppuswami scale.
BMI, body mass index; CS, cesarean section; SD, standard deviation.
Time Taken (Hours) to Initiate Breastfeeding and Ambulation and Visual Analog Score in Three Groups
Bold values depicts statistically significant value (p-value < 0.05).
BF, breastfeeding; SD, standard deviation; VAS, visual analog score.
Correlation of Different Variables with Visual Analog Score During First 6 Hours
Bold values depicts statistically significant value (p-value < 0.05).
BF, breastfeeding; VAS, visual analog score.
Patient demographics
Patient demographics and baseline characteristics were comparable among the three groups as shown in Table 1.
Study outcomes
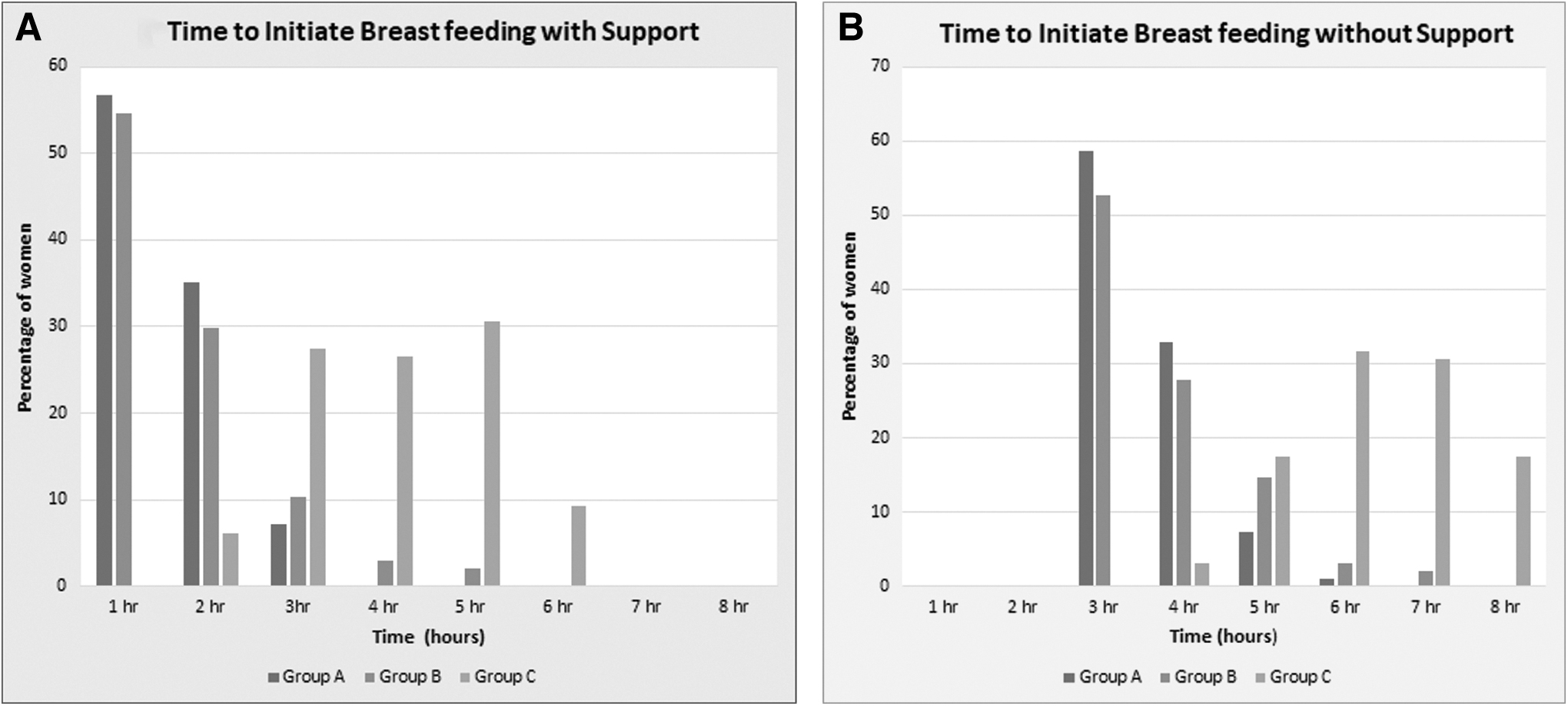
Overall, the rate of early initiation of BF within an hour after CS in the study group was quite low (36.0%). However, more than 50% of women in Groups 1 and 2 initiated BF with support at 1 hour (Fig. 2A) and without support at 3 hours (Fig. 2B). BF (both with and without support) was initiated significantly earlier in Groups 1 and 2 as compared with control Group 3 (p < 0.001) (Table 2). The intergroup analysis between Groups 1 and 2 showed a significantly shorter time taken to initiate BF without support in Group 1 (p = 0.028).
The time to start ambulation (both with and without assistance) was significantly lower in Groups 1 and 2 as compared with control Group 3 and in Group 1 versus Group 2 (p < 0.001) (Table 2).
The mean VAS score after CS was significantly lower in Groups 1 and 2 versus Group 3 at all times. The intergroup analysis between Groups 1 and 2 showed a comparable VAS score during initial 6 hours followed by a significantly lower VAS score at 12 and 18 hours (Table 2).
Correlation coefficient
On correlation analysis, there was a significant positive correlation between the time to initiate BF with support and ambulation without assistance and postoperative pain intensity at 0, 1, and 6 hours as shown in Table 3.
Discussion
We conducted this study to compare the influence of different adjunctive analgesics on the early initiation of BF and early ambulation following a CS. The importance of early postpartum ambulation and BF initiation within an hour cannot be overemphasized. The benefits of these practices to the mother and newborn are immense.16,17 Early initiation of BF not only ensures the intake of the first milk “colostrum” by the newborn but also promotes skin-to-skin contact between mother and baby. It plays a great role in preventing hypothermia, infections, reducing neonatal morbidity and mortality, and improving the overall child's health.18,19 The maternal benefits include reduced risk of postpartum hemorrhage, establishing mother and infant bonding, and promoting exclusive and continued BF for a longer duration.20,21 Early postpartum ambulation enhances recovery, reduces thromboembolic complications, and improves the ability to BF the baby.
Although there are many factors that influence the timing of initiation of BF and ambulation, post-CS pain is one of the most commonly cited reasons.6,7 The present study findings show that ∼28.3% of women experienced a considerable level of pain (VAS ≥4) even 12 hours after CS that needs adequate treatment. A study by Karlström et al has reported that 78% of women had a VAS pain score ≥4 during the first 24 hours after CS. 15 Even with significant levels of pain, the woman is expected to recuperate rapidly and to look after the newborn within a few hours. Optimal pain management post-CS is, therefore, a vital step in enhancing the woman's ability to BF, early ambulate, and improve bonding with her baby. 22
The procedure-specific postoperative pain management (PROSPECT) guidelines for elective CS performed under neuraxial anesthesia recommend the use of multimodal analgesia postoperatively, including regular acetaminophen and NSAIDs, with opioids used for rescue. 23 The American College of Obstetricians and Gynecologists recommends acetaminophen, NSAIDs, and opioids (oral or parenteral) as the standard adjuvant drugs used for post-CS analgesia. 11 The current study findings support the efficacy of a multimodal approach for post-CS pain management as the mean VAS score was significantly lower with the use of adjunctive analgesics versus the control group. The rectal route of adjunctive drug administration was chosen as it is noninvasive, convenient to use, has fewer side effects, and a better safety profile considering the limitation on the use of systemic opioids in BF mothers. 24
The study found that the rate of early initiation of BF and early ambulation was negatively affected by post-CS pain. Women who received rectal diclofenac as part of multimodal analgesia were more likely to initiate BF (without support) and ambulate (without assistance) earlier as compared with rectal tramadol (p = 0.028). Therefore, the inclusion of rectal diclofenac concomitant with IV acetaminophen in post-CS analgesic regimens is a suitable option. It may be of great importance in day-to-day clinical practice, especially in low-resource countries, as rectal diclofenac is cost-effective, convenient to use, and without opioid-related side-effects. This, potentially, can have a positive impact on reducing the rates of delayed BF among post-CS mothers and optimizing maternal and neonatal health.
The strength of the study includes its randomized double-blinded and placebo-controlled study design. To the best of the authors' knowledge, this is the first study to investigate the effects of an analgesic intervention on rates of early BF and ambulation post-CS. There are certain limitations of the study, which include first, relatively smaller sample size. Second, besides postoperative pain score, other possible factors affecting the practice of early BF and ambulation post-CS (such as availability of supporting hospital staff, maternal breast problems, prelacteal feeding, and poor hospital practices) also need consideration. Third, the use of just the VAS score for pain intensity assessment. Although VAS is one of the most commonly used pain intensity rating scales, recent research has identified the Numerical Rating Scale and Faces Pain Scale-Revised as more appropriate measures of pain intensity in nonwestern populations. 25 Further studies with a larger sample size, assessment of other contributory factors, and the use of more objective pain assessment tools are recommended.
Conclusion
Effective post-CS analgesia is an important factor that affects early initiation of BF and ambulation in the immediate postnatal period. The benefits are evident irrespective of whether BF and ambulation are initiated independently or with assistance. The inclusion of rectal diclofenac suppository in post-CS analgesic regimens is a promising approach to postoperative delivery care.
Footnotes
Acknowledgment
The authors would like to thank all the women who participated in the study.
Authors' Contributions
R.H.: Conceptualization (lead); review and editing (equal); and supervision. N.M.: Conceptualization (supporting); writing—original draft (lead); and writing—review and editing (equal). P.P.: Software (lead); formal analysis (lead); and writing—review and editing (equal). H.M.: Methodology (lead); and writing—review and editing (equal). V.S.: Writing—original draft (supporting); and writing–review and editing (equal).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.