
Abstract
Background:
The ability to complete nipple feedings is one of the discharge criteria for most premature neonates. The Infant Driven Feeding (IDF) program suggests a system of objective promotion of oral feeds in premature infants. There is a lack of studies systematically studying the effects of IDF on the provision of breast milk.
Methods:
This was a retrospective study of all premature infants born before 33 weeks and birth weight of <1,500 g admitted to a level IV neonatal intensive care unit. Infants on IDF were compared with those not on IDF.
Results:
A total of 46 infants in the IDF group and 52 in the non-IDF group met the inclusion criteria. A higher number of infants in the IDF group breastfed at first oral attempt (54% versus 12%). Forty-five percent of IDF mothers completed a full 72 hours of protected breastfeeding at the start of oral feeds, and IDF infants had earlier removal of nasogastric (NG) tube. There was no difference in the provision of breast milk and/or breastfeeding on discharge between the two groups. There was no difference in the length of stay between the two groups.
Conclusion:
The IDF program attempts to streamline the promotion of oral feeds in very low birth weight infants. Higher incidence of breastfeeding at the start of oral feeds and earlier removal of NG tube did not translate into higher provision of breast milk on discharge in very low birth weight infants in the IDF group. Prospective randomized trials are needed to validate cue-based infant driven feeding programs and their effects on the provision of breast milk.
Introduction
All premature infants admitted in a neonatal intensive care unit (NICU) need to demonstrate a few basic physiological skills before they are deemed safe to be discharged home with their parents.1–3 Out of these skills, the ability to orally feed is one of the most important criteria used to determine the ability to go home.3–6 Time of onset and maturation of skill to orally feed in preterm infants is highly variable, with studies suggesting starting points of post-menstrual age of 30 weeks to up to 45 weeks gestation. 2
Oral feedings initiation and advancement protocols vary between NICUs. Provider driven, volume based, and time cycled feedings protocols, which are primarily based on infant gestation and weight, are the most frequently used traditional methods. 7 Often, preterm infants require nasogastric (NG) tube feedings before developing feeding independence and the transition to independent oral feeding can present with many challenges.
The progression from NG tube feedings to oral feeding is driven by the infant's neurodevelopmental maturity. The aim of feeding advancements during the NICU stay focuses on avoiding stress related to feeding, while maintaining positive feeding experiences for the preterm infants and parents as much as possible.8–11
Cue-based oral feeding initiation and advancement has the potential to decrease the infant's stress, overfeeding, and potentially decrease time to achieve full oral feeds.7,11 There is evidence to suggest that maturation of suck-swallow-breathing reflex in premature infants can be enhanced by earlier introduction of sucking practice where an infant controls flow of the feedings.
The Infant Driven Feeding (IDF) program is composed of three behavioral assessments: feeding readiness, quality of feeding, and caregiver support. Each assessment includes five categories and is intended as a method of communication among caregivers regarding the infant's readiness and progression toward independent oral feeding.12,13
Literature on the implementation of IDF is scant and littered with variable methodologies.11,13,14 There is also conflicting evidence on the effects of the IDF program on the provision of breast milk in very low birth weight infants.6,7,15 Early provision of breastfeeding and mother’ own milk have been shown to improve the odds of provision of breastfeeding and mother's own milk on discharge in infants admitted to the NICU. 16 Improving the provision of breast milk in the NICU is challenging and requires a systematic approach, which includes improving communication, protocol-based advancement of earlier oral feeds, and addressing barriers.17–19
A cue-based IDF program has been adopted across NICUs7,13,15; an infant driven feeding program was implemented at our Level IV NICU, giving us the opportunity to study the effects of IDF on the provision of breast milk. Our aim was to determine the outcome of the provision of breast milk in premature infants who were <33 weeks and weighed <1,500 g after the implementation of the IDF program.
Methods
The Institutional Review Board for the protection of human subjects at the Texas Tech University Health Sciences Center in El Paso, TX, approved this retrospective chart review study with a waiver of consent. IRB No. E22012.
This was a single-center study conducted at an academic level IV NICU.
We analyzed neonates admitted to the NICU between January 2019 and August 2021. Neonates with a birth weight of <1,500 g and birth gestation <33 weeks were included in this study.
We then divided these neonates into two groups: infants admitted before the implementation of the IDF program (non-IDF) and infants admitted after implementation of the IDF program (IDF). The transition/rolling out period of this program included several interdisciplinary meetings and educational sessions with bedside nurses, speech therapists, and neonatologists. Infants admitted during the 6 months of introduction/transition and rolling out period were excluded from the study.
Infant driven feeding
The IDF method is composed of three behavioral assessments: feeding readiness, quality of feeding, and caregiver support. Each assessment includes five categories and is intended as a method of communication among caregivers regarding the infant's readiness and progression toward independent oral feeding. This program was implemented for infants born <33 weeks gestation. The IDF program was subdivided into two parts:
IDF assessment period: This is the time in the life of a premature infant when oral feeding assessment checks can be started. To qualify to start IDF assessment, an infant has to meet the following criteria
Be at 32 weeks corrected gestation
Require respiratory support of 2 L per minute or less
No other medical indication for non-initiation of oral feeds.
Attached is the feeding initiation protocol. Figure 1.
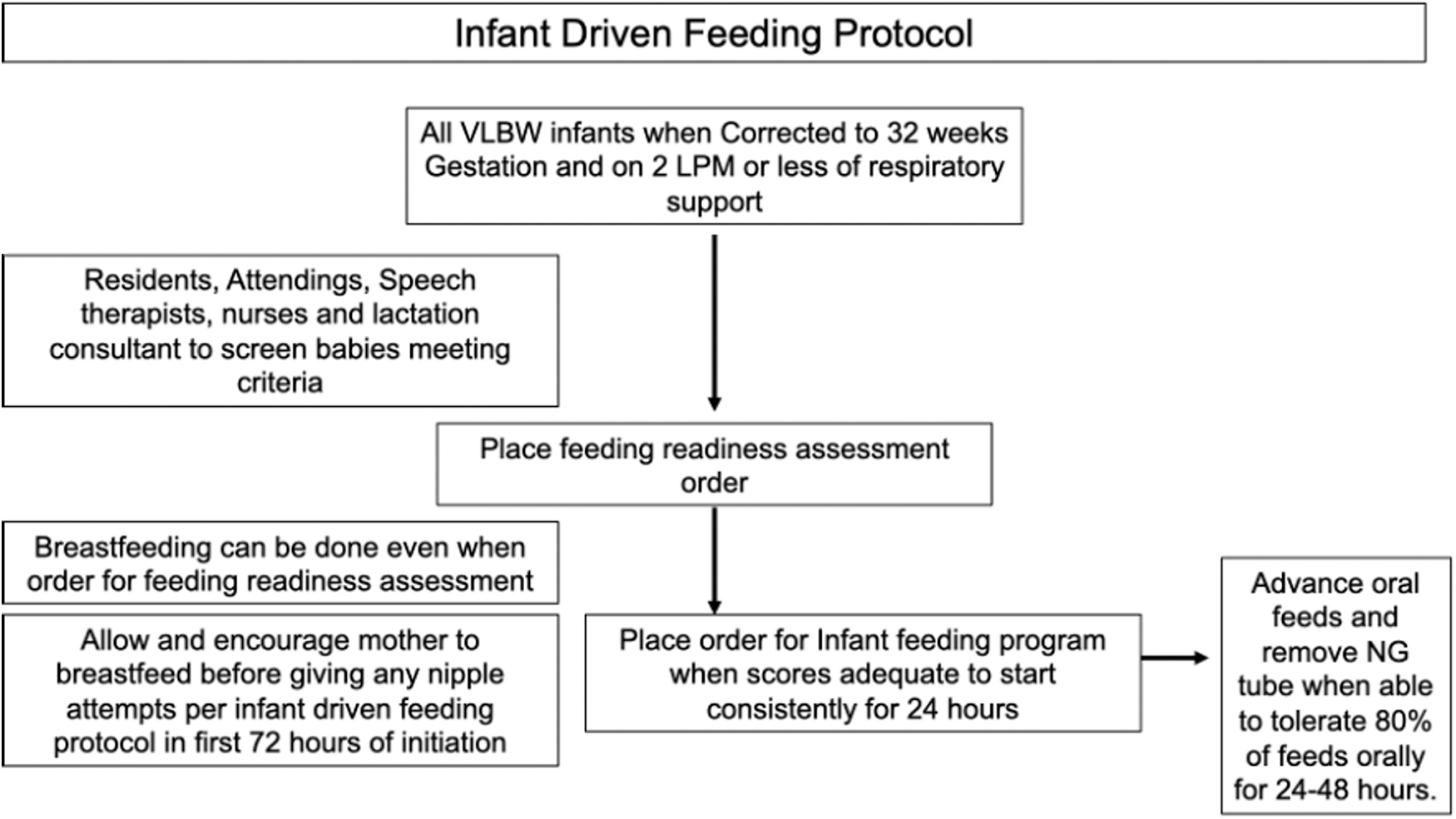
Infant driven feeding program protocol. LPM, liters per minute; VLBW, very low birth weight.
Once an infant meets the earlier cited criteria, bedside nurses and speech therapists begin feeding readiness scoring. Bedside caregivers then document feeding readiness score (range 1–5) every 3 hours and continue to gavage feed until readiness scores are in the range of 1–2 for 48 hours for >50% of the time. At this point, an order for infant driven feeding protocol is placed.
IDF protocol period: When a preterm infant consistently scores less than three points on feeding readiness score for 48 hours, the infant is determined to be ready to initiate oral attempts. We offer a “protected breastfeeding window” of 72 hours to mothers, during which no artificial nipple is introduced for oral feeding attempts. If the mother does not wish to, or is unable to participate in this window, or after completion of the “protected breastfeeding window,” a preterm can be offered artificial nipple feeds. If a mother desires to solely breastfeed, then we do not introduce any artificial nipple for the first 72 hours.
Quality scores (range 1–5) are then documented after the initiation of nipple feed. Infants are orally fed for a maximum of 30 minutes and the remaining volume is gavage fed. The amount of milk taken, amount of gavage fed, as well as the caregiver's techniques are documented (Table 1).
Infant Driven Feeding Program Scorecard
HR, heart rate; IDF, Infant Driven Feeding; RR, respiratory rate; SSB, suck swallow breathing.
Non-IDF group
Infants in this group were from the period before the implementation of the infant driven feeding program. Oral feeds in this group were initiated and advanced based on the discretion of neonatologists, speech therapists, and bedside nursing assessments.
Neonates who either died during hospitalization or were admitted after the first week of life were excluded from this study. All mothers and infants with incomplete data were excluded from the final analysis of this study.
Descriptive statistics (median, 25th, and 75th percentiles for continuous variables; frequencies and percentages for categorical variables) were calculated separately by groups. The student unpaired T-Test, chi-square test, or Fisher's exact test, as deemed appropriate, for categorical variables and the Mann–Whitney test (two-group comparisons) were used to assess statistical significance. A result was considered statistically significant at p < 0.05.
Results
During the study period of January 2019 through August 2021, a total of 109 preterm infants weighing <1,500 g with a birth gestation <33 weeks were admitted to the NICU. Of this, 56 were admitted before the implementation of IDF (non-IDF group) and 52 after the implementation of IDF (IDF group). A total of 47 in the IDF group and 52 in the non-IDF group were included in the final analysis (Figure 2).

Distribution of patients. IDF, Infant Driven Feeding.
There was no difference in age, gravidity, ethnicity, race, maternal morbidities, or educational status of mothers of infants admitted to the NICU in both groups (Table 2).
Maternal Parameters
Gestational or chronic hypertension.
IDF, Infant Driven Feeding.
Gestation at birth was higher in infants in the IDF group (29 ± 2 weeks versus 28 ± 3 weeks). There was no difference in birth weight, sex, or mode of delivery in preterm neonates of both groups. Apgar at 1 minute was higher in the IDF group but there was no difference in 5-minute Apgar (Table 3).
Neonatal Outcomes
High flow nasal cannula—2–3 LPM. Low flow cannula <2 LPM.
CPAP, continuous positive airway pressure; IDF, Infant Driven Feeding; LPM, liters per minute; NIPPV, non-invasive positive pressure ventilation.
First attempts at oral feedings were started at similar ages in both groups (41 ± 29 days versus 39 ± 27 days). Total days requiring NG tube feedings were lower in the IDF group. Corrected gestation at achieving NG tube removal was lower in the IDF group (37 ± 3 weeks versus 39 ± 4 weeks). No difference in the need of NG tube reinsertion in both groups was noted.
When analyzing the type of NG tube feeding before the first oral attempt, we discovered that mothers' own milk and formula were equally given to both groups.
Breastfeeding was recorded in 53% of infants in the IDF group compared with only 12% in the non-IDF group as the method for the first oral feed. Reasons for inability to breastfeed at the first oral attempt were similar in both groups, but in the majority of cases reasons were unknown or unclear from chart review. Forty-five percent of mothers in the IDF group completed full 72 hours of the breastfeeding window. Infants in the IDF group had higher weight (1,957 ± 581 g versus 1,724 ± 391 g) and head circumference (30 ± 2 cm versus 29 ± 2 cm) at the first oral feed attempt (Tables 3 and 4).
Neonatal Outcomes
BPD, bronchopulmonary dysplasia define per NICHD consensus statement; IDF, Infant Driven Feeding; NG, nasogastric; NEC, necrotizing enterocolitis; NICU, neonatal intensive care unit; PBW, protected breastfeeding window; ROP, retinopathy of prematurity requiring intervention; Severe IVH, intraventricular hemorrhage Grade 3 or 4.
Infants in the IDF group were more likely to be on room air or require minimal oxygen support when the first oral attempt was recorded compared with infants in the non-IDF group (Table 3).
There was no difference in major morbidities, including severe intraventricular hemorrhage (Grade 3 or 4), bronchopulmonary dysplasia, necrotizing enterocolitis, retinopathy of prematurity needing intervention, and blood culture positive sepsis (Table 4).
There was no difference in the type of milk provision on discharge between the two groups. There was also no difference in the length of stay or discharge weight between the two groups (Table 4).
Discussion
Our study is one of the few studies detailing the effects of implementation of an infant driven feeding program on the provision of breast milk in very low birth weight infants. This study shows that a structured roll out of a cue-based infant driven feeding program can potentially increase rates of direct breastfeeding at first oral attempts, with 53% of infants in the IDF group attempting breastfeeding at the first oral feed and 45% of infants receiving exclusive breastfeeding during the first 72 hours of the first oral attempts.
However, this did not translate into increased provision of breast milk at discharge in very low birth weight infants. This leads us to believe that although earlier attempts at breastfeeding are desirable, that may not convert into higher provision of breast milk after discharge due to other unquantifiable variables such as personal beliefs, environmental barriers such as transportation and financial security, partners' involvement, and/or cultural beliefs.15,20,21 This study also indicates that improving breastfeeding is not a singular event and needs a multiprong approach. 22
A prospective study examining these effects could potentially shed light on the reasons and give direction for improving the provision of breastfeeding. We are planning to study this in the next phase of our project.
The non-IDF group infants, when started on oral feeds, were on higher respiratory support compared with the IDF group. Infants in the non-IDF group were more likely to be on high flow nasal cannula at flow of 2–3 L per minute of respiratory support when initiating oral feeds. Initiation of oral feedings while on respiratory support is a common practice in preterm infants.23,24
The potential adverse effects of oral feedings while on significant respiratory support (continuous positive airway pressure) have been reported,25,26 but whether oral feeds on high flow nasal cannula leads to any adverse effects remains largely unknown. 27
This study shows that the infants in the IDF program initiated oral feeds later but had earlier removal of the NG tube, and earlier achievement of complete oral feeds. But it was also noted that infants in the IDF group were of higher birth gestation and had higher weights at the start of oral feed attempts. We think this difference is the most likely reason for earlier achievement of oral feeding in the IDF group.
It is a known fact that oral feeding skills are directly related to gestation 28 ; however, results of this study are in line with previous publications, indicating the usefulness of readiness scale and objective support techniques such as the IDF program, which may also have played a role in easing infants' transition to complete oral feeds. What we also deduced from the results is, although the IDF group infants were NG tube free earlier, that did not result in a reduction in length of stay.
Major morbidities such as intraventricular hemorrhage, bronchopulmonary dysplasia, necrotizing enterocolitis, and retinopathy of prematurity are some of the primary determinants of length of NICU stay for preterm infants.29,30 We found no difference in major morbidities between the two groups.
A study conducted by McCain et al suggests shorter time to achievement of oral feeds with cue-based feeding. 14 A few quality improvement projects have shown similar results of earlier achievement of full oral feeds with IDF cue-based feeding. 13 This finding suggests structured cue-based feeding; although it might be desirable to streamline oral feeding advancement, earlier achievement of oral feeds may not increase the odds of earlier discharge from the NICU. It may be worth assessing post-discharge feeding preferences, speech, and cognitive outcomes in this high-risk group of preterm infants in the IDF group.
There are several limitations to our study. First, this is a retrospective chart review study that inherently can only demonstrate association. Second, sample size in our study is small and has potential to confound results. However, our results align with associations found in other published studies. Third, although the IDF program does provide an objective guide for progression of oral feeds, these assessments depend on the staff doing the assessments, and our study did not determine the effects of the IDF program on the flow of care provided by nursing staff.
Does IDF negatively impact care burden on bedside care providers such as nurses and on parents, or does it improve the flow of care in the NICU, will be worth further exploration. Future direction for research on this topic must include the effects of IDF on the flow of care at the bedside and post-discharge outcomes.
Conclusion
The IDF program attempts to streamline the promotion of oral feeds in very low birth weight infants. Although there was an indication of higher incidence of breastfeeding at the start of oral feeds and earlier removal of the NG tube, that did not translate into higher provision of breast milk on discharge in very low birth weight infants. Prospective randomized trials are needed to validate cue-based infant driven feeding programs and their effects on the provision of breast milk.
Footnotes
Acknowledgment
The authors want to thank the Biostatistics department of Texas Tech University Health Sciences Center for their help in analyzing data.
Authors' Contributions
Conceptualization: A.P.S. and S.P.; Methodology: A.P.S., S.P., and D.R.; Formal Analysis: A.P.S.; Data Curation: A.P.S. and S.P.; Writing—Original Draft Preparation: A.P.S., S.P., D.R., N.D., and C.J.; Writing—Review and Editing: A.P.S., S.P., D.R., N.D., and C.J.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.