
Abstract
Introduction:
Seventy percent of countries follow the World Health Organization International Code of Marketing Breast Milk Substitutes that prohibits infant formula companies (IFC) from providing free products to health care facilities, providing gifts to health care staff, or sponsoring meetings. The United States rejects this code, which may impact breastfeeding rates in certain areas.
Objective:
We aimed at gathering exploratory data about interactions between IFC and pediatricians.
Methods:
We distributed an electronic survey to U.S. pediatricians asking about practice demographics, interactions with IFC, and breastfeeding practices. Using the zip code of the practice, we obtained additional information from the 2018 American Communities Survey, including median income, percent of mothers who had graduated college, percent of mothers working, and racial and ethnic identity. We compared demographic data for those pediatricians who had a formula company representative visit versus not and those who had a sponsored meal versus not.
Results:
Of 200 participants, the majority reported a formula company representative visit to their clinic (85.5%) and receiving free formula samples (90%). Representatives were more likely to visit areas with higher-income patients (median = $100K versus $60K, p < 0.001). They tended to visit and sponsor meals for pediatricians at private practices and in suburban areas. Most of the reported conferences attended (64%) were formula company-sponsored.
Conclusion:
Interactions between IFC and pediatricians are prevalent and occur in many forms. Future studies may reveal whether these interactions influence the advice of pediatricians or the behavior of mothers who had planned to exclusively breastfeed.
Introduction
Physician interaction with pharmaceutical companies has been regulated in recent decades due to its known influence on physician behavior.1,2 Providing free samples to physicians has proven to be extremely profitable for pharmaceutical companies. 3 Studies have shown that physicians are more likely to prescribe a drug received as a free sample, 4 even if it is irrational or not their first choice. 5
Similarly, pharmaceutical company-sponsored conferences in promotion of a drug have a predictable effect: prescribing of that drug increases significantly afterward. 6 Physicians consistently report that they believe their own prescribing behavior is unaffected by pharmaceutical companies; they simultaneously report that other physicians, in fact, are influenced. 7 The fact that physicians are apparently blind to their own susceptibility to influence underscores the strong and surreptitious impact of product promotion.
Like pharmaceutical companies, infant formula companies (IFC) promote their products to pediatricians with free samples, gifts, and conference sponsorship. As a result, sales and advertising by IFC have paralleled the trajectory of pharmaceutical companies. From 2005 to 2019, global formula sales doubled, with a total revenue of $55.6 billion in 2019. 8 It has been estimated that IFC spent $51 on marketing for every baby born worldwide in 2015. 9 Notably, in 1981, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) passed the International Code of Marketing Breast Milk Substitutes (“The Code”) in an effort to curtail the impact of IFC on breastfeeding rates around the world.
The Code passed with 118 votes in favor and one vote against, the United States (U.S.), and was adopted by the World Health Assembly (WHA).10,11 In 2016, further recommendations from the WHA stated that IFC should not provide free products to health care facilities, provide gifts to health care staff, or sponsor meetings. 12 Today, the United States remains one of only 30% (58/194) of WHO Member States, and a prominent outlier in the global north, without any laws to enforce The Code. 13
There are several reasons why relationships between IFC and pediatricians should be investigated. These interactions may impact breastfeeding rates in the United States as a whole or selectively for certain groups. Even as breastfeeding rates in the United States improve, disparities between breastfeeding rates for Black versus White infants continue to be substantial, independent of socioeconomic and demographic factors. 14 Targeted marketing of certain demographic areas by IFC could potentially influence breastfeeding rates, and pediatricians may play a role.
According to market research in the United States of 581 mothers not participating in Supplemental Nutrition Program for Women, Infants, and Children (WIC), 48% of mothers reported that they chose their first formula based on an obstetrician, pediatrician, or other clinician recommendation (Ravel Market Research, e-mail communication, October 2021). A 2022 study of 1800 women in eight countries commissioned by the WHO and UNICEF reported that health care workers are the main source of information regarding infant feeding practices. In addition, for the 300 health professionals surveyed, free samples, gifts, funding for research, and sponsored conferences were determined to be highly influential. The study found that health professionals repeat formula company marketing messages to women, knowingly or unknowingly. 15
We are aware of no studies to date that quantitatively or qualitatively report how pediatricians interact with infant formula company representatives (IFCR). We aimed at gathering exploratory information about the prevalence of contact between general pediatricians in the United States and IFCR, which areas IFCR are more likely to visit, and how this might relate to clinical practice and breastfeeding rates in that area. Although no baseline data exist on this topic, we hypothesized that interactions with IFCR would be prevalent, as 77% of physicians accept free drug samples from representatives. 3
Disparities in breastfeeding rates are likely multi-factorial and interdependent, but we conjectured that IFCR visits may be one factor. As such, we suspected that IFCR would be more likely to visit lower- income areas. Although many low-income patients qualify for free formula through WIC, the program is designed to cover only 80% of infants' needs and their families must purchase some formula.
Methods
A survey was developed to query general pediatricians in the United States about their interactions with IFC. Survey questions were created in three domains: practice demographics, IFC interactions, and breastfeeding knowledge (Table 1). For coding of responses, the conference website was used to determine if it was sponsored by IFC. For the question about resources, “Hale's,” “Lactmed,” or other impartial established resources were coded as acceptable; “Google” was coded as unacceptable. For the question about whom do patients call for timely advice, “our office's lactation consultant,” “La Leche League,” or equivalent responses were coded as acceptable. The study was determined to be exempt from in-depth reviews by our institutional IRB.
Survey Question Domains
Imagine you encounter the following at your practice: you are seeing a full-term baby for an initial visit at 3 days of life. She has been exclusively breastfeeding with a good latch and normal voids and stools but appears jaundiced to the level of the umbilicus. You will not be able to see the baby for a follow-up visit until 4 days later as your office will be closed for a holiday weekend. What would you recommend?
AAP, American Academy of Pediatrics; IFC, infant formula companies; PAS, Pediatric Academic Societies; WIC, Supplemental Nutrition Program for Women, Infants, and Children.
The survey was distributed in a stepwise manner to the following groups to obtain a representative sample of U.S. pediatricians: “Practicing Pediatricians” Facebook Group, American Academy of Pediatrics (AAP) Section on Administration and Practice Management, AAP Committee on Practice and Ambulatory Medicine, Yale Medicine-affiliated pediatricians, and Ohio State AAP. The survey was distributed in stages from October 5, 2020 to May 11, 2021. Participants were incentivized with the possibility of winning one of two $100 Amazon gift cards.
After collection of survey data, the zip code of the participants' pediatric practices was used to obtain additional demographic data. Data on women aged 15–50 years who had given birth in the past 12 months were extracted from the 2018 American Communities Survey (ACS), 16 including the percent who had graduated college, percent working, and racial and ethnic identity. Median household income of each zip code from the 2018 ACS was extracted based on the entire population in that zip code.
We a priori estimated that acquisition of responses from 200 participants would give us the width of 0.14 in the 95% confidence interval around a projected 0.70 proportion of respondents with a visit from IFCR. Unadjusted between-group comparisons were analyzed using Chi-square or Fisher's exact tests for categorical data and Mann-Whitney U-test for continuous data; Pearson correlation coefficient (r) was used to associate two continuous variables.
Median exclusive breastfeeding percent was compared by IFCR visit (yes/no) or sponsored meal (yes/no), using a quantile regression, adjusting for type of practice (private/other) and percent of WIC recipients. The latter were chosen among candidate covariates from the unadjusted associations with exclusive breastfeeding, avoiding multicollinearity among covariates and keeping the total number of covariates between 3 and 4 to avoid model overfitting.
Due to the explorative nature of this study, we did not set a strict alpha level of 0.05 but interpreted our findings within the magnitudes of effect sizes and directions of associations. Statistical analyses were performed using SAS 9.4 (Cary, NC) and R software version 4.0.5 (2021).
Results
The survey was sent to 6290 pediatricians. With 200 usable responses, the overall response rate was 3%. Participants represented a total of 26 states and were from a variety of practice types: private practices (69.5%), academic-affiliated practices (11.5%), combined private and academic practices (4.5%), federally qualified health centers (6.0%), and military bases (0.5%).
Participants were representative of general pediatricians in the United States in terms of age and location based on information from the 2016 AAP Periodic Survey data reported in Sisk et al, 17 which includes post-residency AAP pediatricians (Table 2). Our participants may represent a slightly older and more suburban demographic than the AAP Periodic Survey. Overall, the patient population of respondents was similar to the general U.S. population.
Demographic Data of Pediatrician Participants and Comparison to American Academy of Pediatrics Periodic Survey
Eighty percent of participants reported having attended a conference in the past 5 years. Of those conferences reported, 64% received sponsorship from IFC. Notable exceptions were lactation and breastfeeding-specific conferences.
Of the 189 participants who reported whom patients call for timely lactation support, 5 (2.6%) reported that they were certified lactation consultants and 36 (19%) reported that they personally offer timely lactation support. Seventy-nine (42%) reported that patients may call their office for lactation support, and of those, 38 participants (20%) specified that they have lactation consultants at their office.
Most participants reported a visit to their practice from an IFCR (85.5%) and reported receiving free formula samples in the past 5 years (90%). Forty-three percent reported receiving a sponsored meal. Many reported receiving free merchandise (27.5%).
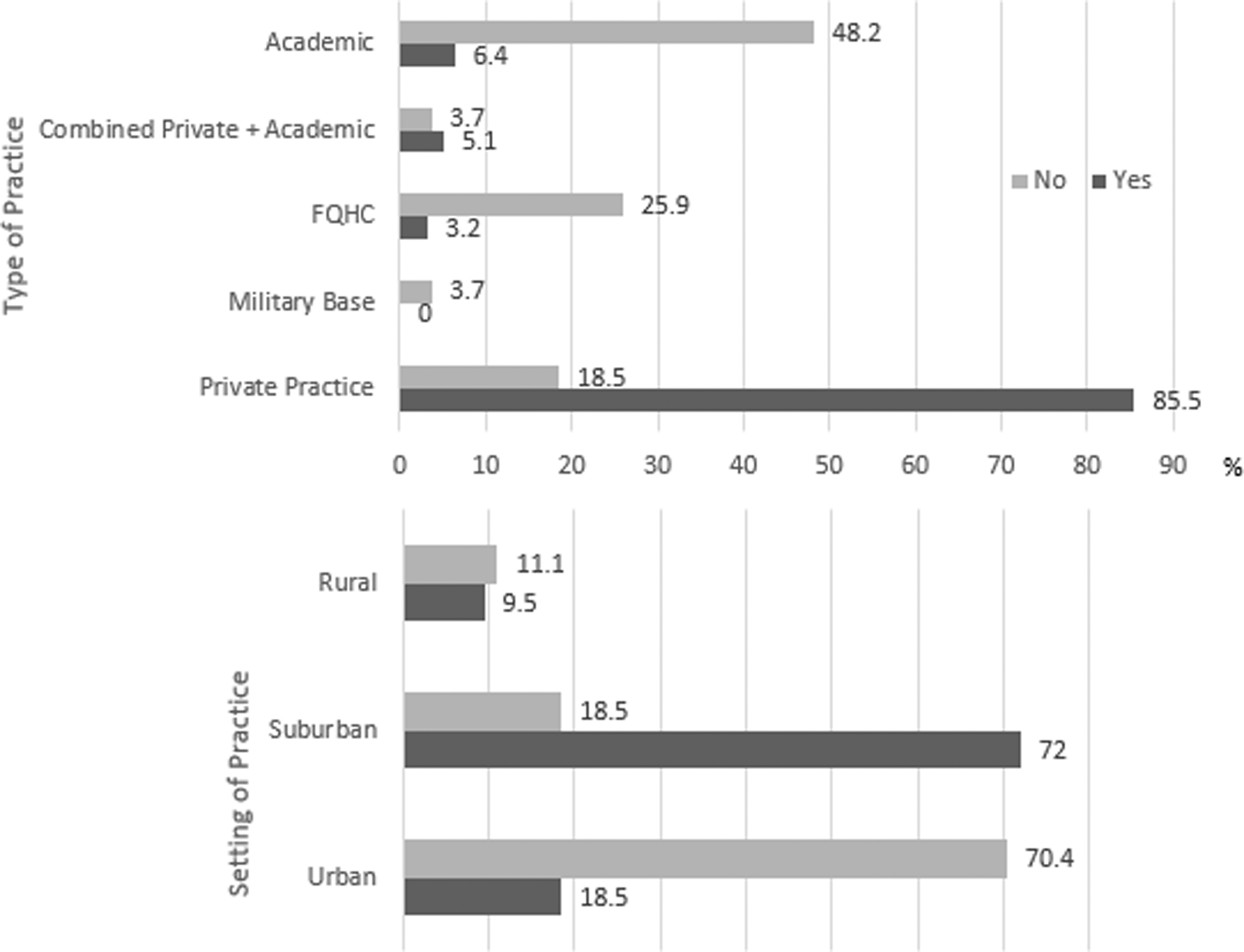
Those who answered “Don't Know” regarding an IFCR visit or sponsored meal (n = 8 for each) were excluded from statistical analysis. Pediatricians who reported higher exclusive breastfeeding rates and practiced in higher-income areas were more likely to report IFCR visits (Table 3). Those practices with IFCR visits had fewer Black and Hispanic patients in the surrounding area (Table 3). Pediatric practices with visits from IFCR were more likely to be in suburban areas (p < 0.001) and more likely to be private practices (p < 0.001, Fig. 1). Practices of pediatricians who received an IFC-sponsored meal demonstrated similar trends (Fig. 2).
Type (

Type (
Characteristics of Patients at Practices With/Without Visits from Infant Formula Company Representatives
IFCR, infant formula company representatives; IQR, interquartile range; WIC, Supplemental Nutrition Program for Women, Infants, and Children.
Pediatricians who did not have visits from IFCR reported similar levels of knowledge about quality resources (72.4% versus 77.8%, p = 0.53) or hotlines for lactation assistance (86.2% versus 92.4%, p = 0.28) to those who did have visits from IFCR. The same was true for pediatricians who did versus did not report receiving a sponsored meal. In a hypothetical scenario of breastfeeding jaundice, pediatricians whose clinics were visited by IFCR were not more likely to advise formula supplementation (86.7% versus 88.9%, p = 1.00), but those who reported receiving an IFC-sponsored meal tended to recommend supplementation (Table 1,*) more often (17.5% versus 7.9%, p = 0.05).
The percentage of WIC participants was negatively correlated with exclusive breastfeeding rates (r = −0.46, p ≤ 0.001). Private practice was positively correlated with exclusive breastfeeding rates (median = 55% in private practice and median = 34% in other types, p < 0.0001). When adjusted for type of practice and percent of WIC recipients, exclusive breastfeeding rates were similar between practices with IFCR visits (median = 42.7%) and practices without IFCR visits (median = 45.1%, p = 0.61), indicating that the observed difference in median exclusive breastfeeding rates in Table 3 may be explained by the types of areas IFCRs visited.
Discussion
The results of this study suggest that the interaction between IFC and U.S. pediatricians are ubiquitous, with an overwhelming majority of participants reporting IFCR visits and receiving free samples. More pediatricians report having IFCR visits than report having a lactation consultant in their office. In this preliminary assessment, IFCR tended to visit higher-income areas, suburban areas, and private practices, which also had higher exclusive breastfeeding rates. The adjusted analysis suggests that differences in exclusive breastfeeding rates between the two groups can be explained by type of practice and proportion of WIC recipients.
Most pediatricians know of quality resources for lactation assistance, but only 40% reported that patients contact their office for lactation support. This disconnect requires further exploration as to whether the pediatricians' interaction with IFCR and specifically the free formula samples affect the patients' perception of the pediatrician as a lactation resource. This likely is compounded in practices with a higher proportion of WIC recipients having fewer resources for lactation support in their offices. Further, this provides information about where to direct advocacy efforts to improve breastfeeding rates in lower-income areas, such as increased office lactation support.
There are several possible explanations for IFCR tending to visit and sponsor meals for physicians at private practices and in suburban areas. First, some academic practices may not allow IFCR visits due to prohibition of pharmaceutical detailing by some academic medical centers. By the same token, practices affiliated with Baby Friendly Hospitals (590 U.S. hospitals, 18 29.1% of live births 19 ) may not allow IFCR visits or free samples. Second, IFCR may visit these areas due to their higher exclusive breastfeeding rates at 3 months.
Because the number of women who are exclusively breastfeeding drops off over time, IFC have an opportunity for customer acquisition, with the goal to have breastfeeding mothers switch to formula sooner and choose their brand. The IFC are aware that 57% of mothers start using formula earlier than planned and by an average of 3–4 months (Ravel Market Research, e-mail communication, October 2021). Third, lower-income areas with a higher proportion of patients receiving WIC are a saturated market.
Although WIC only covers 80% of an infant's formula needs, 20 whichever company is awarded a state's WIC contract receives shelf visibility, brand loyalty, and perceived endorsement from WIC. 21 Though little published information is available, IFC likely have data on patients' parents' patterns of behavior surrounding infant feeding that is not available to pediatricians.
We acknowledge several limitations of this exploratory study. Due to a low response rate, likely a consequence of electronic distribution, survey respondents might potentially be a non-representative sample of U.S. pediatricians. However, we attempted to limit bias in the invitation process via distribution to broad outpatient pediatric groups, rather than lactation or academic-oriented listservs. Due to pediatricians' appreciation for breastfeeding and professional ethos, it is possible that our study actually underestimates the true prevalence of IFC and pediatrician interaction. Finally, we do not suggest that the associations reported here are causal, but those associations are, nonetheless, of interest for future studies.
As previously stated, numerous studies of interactions with drug companies have shown that contact influences prescriber behavior.1–6 Thus, implementation of evidence-based strategies to increase breastfeeding prevalence and duration likely involves limiting formula company contact with health care providers. Brazil, which is substantially aligned with the Code, has succeeded in improving breastfeeding rates even during economic growth and urbanization. 22
Similarly, implementation of the 10 Steps to Successful Breastfeeding through the Baby Friendly Hospital Initiative, including adhering to the WHO Code, has demonstrated success in the United States and abroad. 23 The 2022 report by the WHO and UNICEF urges health care professionals throughout the world to pass and enforce domestic legislation aligned with The Code. 16 However, the United States, remains antipathetic to The Code: as recently as the 2018 WHA meeting, which was attended by formula company lobbyists, American delegates opposed a resolution to promote breastfeeding.24,25 Thus, guidance or laws at the federal level remain highly improbable.
In 2022, the AAP released a policy statement titled “Health Care Clinicians Product Promotion by Industry,” which advises pediatricians and other clinicians to educate themselves about how they might be influenced by industry and to be wary of the marketing potential of commercially-funded continuing medical education. 26 The policy does not provide any guidance on pediatrician behavior with respect to interactions with IFCR, accepting free formula samples, or attending formula company-sponsored conferences.
Thus, the interactions reported in this survey do not violate any professional guidelines or laws, although they would violate The Code and federal laws in most other countries. Most importantly, larger studies are needed to document the pervasiveness of formula company interaction with pediatricians and how breastfeeding rates may be affected at the individual and population level.
Conclusion
In the first study of pediatrician and IFC interaction in the United States, survey results suggest that interactions between pediatricians and IFC and their representatives are ubiquitous. The IFCR tend to visit pediatric practices that serve higher-income patients, which are also in areas with higher exclusive breastfeeding rates. The impact of IFCR on patients receiving formula, specifically whether formula is received sooner or when it was not planned, requires further study.
Footnotes
Authors' Contributions
K.M.W.: contributed to conception and design; contributed to acquisition, analysis, and interpretation of data; drafted the article; critically revised the article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. M.R.M.: contributed to conception and design; contributed to analysis and interpretation of data; critically revised article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. V.S.: contributed to conception and design; contributed to analysis and interpretation of data; critically revised article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. S.C.H.: contributed to conception and design; contributed to analysis and interpretation of data; critically revised article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. S.N.T.: contributed to conception and design; contributed to analysis and interpretation of data; critically revised article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Ethical Approval
The study was determined to be exempt from an in-depth review by Yale School of Medicine institutional review board.
Availability of Data and Material
All survey data are available on request. The 2018 ACS data from the U.S. Census are publicly available, but they can also be sent on request.
Disclosure Statement
K.M.W., M.R.M., and S.N.T. all have spoken at academic conferences funded by formula company education funds. S.N.T. is the principal investigator on institutional research grants from Ferring Pharmaceuticals, Pfizer, and Prolacta Bioscience. S.N.T. is the principal investigator on a study funded by Beth Israel Deaconess Medical Center with initiation of funds from Mead Johnson Nutrition. S.N.T. has written chapters for a book and participated in education related to the book that was funded indirectly by Reckitt. V.S. and S.C.H. report no conflicts of interest.
Funding Information
Incentives for survey completion are funded by the Division of Neonatal-Perinatal Medicine at Yale School of Medicine. The authors report no external funding sources.