
Abstract
Background:
Idiopathic granulomatous mastitis (IGM) is a chronic inflammatory condition of the mammary gland that presents as a painful mass, and it must be distinguished from both infectious mastitis and breast cancer. When diagnosed during lactation, it can result in significant distress and early weaning. Injection of triamcinolone has been used as a successful treatment method, but safety in breastfed infants has not been established.
Methods:
We present a case of a lactating patient who received a direct injection of triamcinolone (dosage 40 mg) in her breast to treat IGM after failure of oral corticosteroids. Breastmilk samples were expressed by the patient 0, 1, 4, and 24 hours after the procedure, and then daily for 1 week. All the samples were analyzed using liquid chromatography mass spectrometry. The patient was supported by a breastfeeding and lactation medicine clinic.
Results:
After injection of triamcinolone into the granulomatous mass, breast milk samples were collected and analyzed. No samples were found to contain triamcinolone. A temporary but significant decrease in milk production was noted after injection, though only a slight decrease had been noted with 6 weeks of systemic corticosteroids. With support, the patient rebuilt milk production and continued to breastfeed from both breasts.
Conclusion:
Triamcinolone was not found in any milk samples (≥0.78 ng/mL) following therapeutic injection of the affected breast. The patient was able to continue breastfeeding from the affected breast with intermittent symptoms.
Introduction
Idiopathic granulomatous mastitis (IGM) is a chronic inflammatory disease of the mammary gland that presents as a painful mass. In clinical practice, it must be distinguished from both infectious mastitis and inflammatory breast cancer. 1 While not malignant, when diagnosed during lactation it can result in significant distress due to diagnostic uncertainty, a lack of management consensus, 1 maternal pain, and the effect of treatments on milk production.1,2 This combination can lead to early weaning, which affects both maternal and infant health.
Triamcinolone injections into the affected breast have been used to successfully treat this condition,2,3 but the safety for the breastfed infant has not been established. Triamcinolone is a glucocorticoid with anti-inflammatory and immunosuppressant activity, used to treat various disorders topically, in injected form and systemically. 4 It has a low molecular weight of 434 kDa, high oral bioavailability, and, for breastfeeding purposes, a relatively long half-life of 18–36 hours. 5 Because of the possible risk of growth restriction, and suppression of endogenous corticosteroid production, it has been proposed that weaning from breastfeeding is required from the injected side. 2
Case Presentation
Our patient was a 43 yo Gravida 2 Para 2 Caucasian female who delivered 3 weeks prior a child by repeat c/s for preeclampsia with severe features at 31 + 6 weeks' gestation. Her history included infertility and use of donor egg for in-vitro fertilization, hypothyroidism controlled with levothyroxine, anemia, and a body mass index of 39. She had a history of uncomplicated breastfeeding with her first child for 18 months. The patient developed a red, painful breast mass in the late second trimester of her pregnancy, and after a mammogram and ultrasound showed “ductal debris,” it self-resolved in 3 weeks.
After her preterm birth, she was pump-dependent and struggled with low milk supply, for which she was referred to the inpatient Breastfeeding and Lactation Medicine service (BFLM), a high-risk interprofessional service supporting lactating families, both inpatient and outpatient. A left-sided breast mass was noted 4 weeks after delivery, and it was treated as a clogged duct. At that time, the patient also noted a partial inversion of her left nipple, which was interfering with establishing feeding at the breast.
Physical exam showed asymmetry with her left breast mildly larger than her right, a large firm mass in the left breast from 11 to 1 o'clock, which was mildly tender with no erythema or fluctuance, and bilateral nipple damage likely due to pump use. Presumed diagnosis was plugged duct from improper flange side and nipple shield use leading to milk stasis, and a recommendation was made to use gentle lymphatic drainage massage, decrease in flange size to 21 mm, ice, ibuprofen, sunflower lecithin, and observation for mastitis.
Four days later, the mass was smaller but still present, nipples were improved, and milk production was increased from 15 to 30 mL per pump session. Milk production continued to improve until a full supply was achieved. Due to persistence of the mass, despite clinical resolution of pump damage and milk stasis, imaging was ordered and cephalexin (500 mg qid) was started. On ultrasound, an abscess was identified and 6 mL was drained. The patient reported improvement in discomfort. Breast fluid cultures were positive for 1+Corynebacterium species with a negative gram stain, including for acid-fast bacteria.
A core needle biopsy showed fibroglandular breast tissue with lactation change and acute, chronic, and granulomatous inflammation with numerous multinucleated giant cells and no evidence of malignancy. The differential diagnosis based on pathology was reported to be lactation abscess and cystic neutrophilic granulomatous mastitis. Based on evidence review, doxycycline was suggested, although the patient was reticent to use this due to her infant's prematurity and she did not start the medication. After some initial improvement, she stopped cephalexin. However, the patient continued to experience burning/aching pain and itching over the course of the next 4 weeks, and after swelling and erythema (dark red flush) worsened, she resumed cephalexin with doxycycline to broaden coverage, which improved mass size and symptoms but did not resolve them (Figure 1, Left).
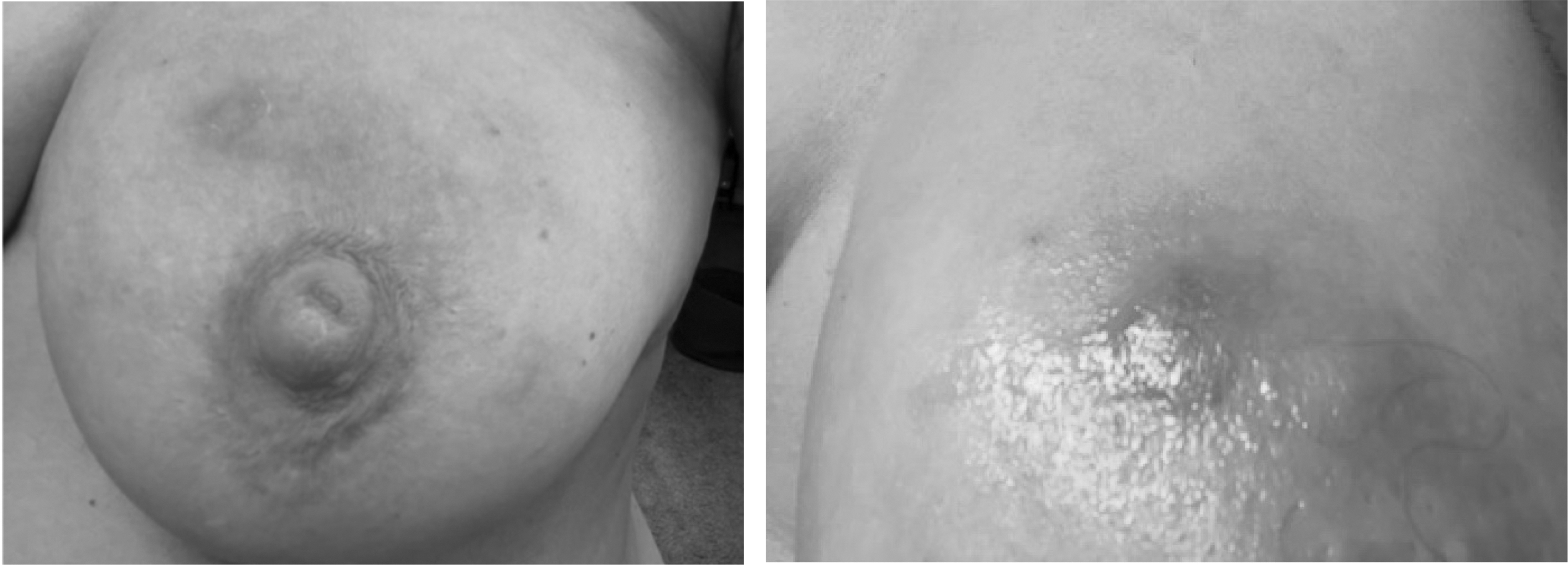
Idiopathic granulomatous mastitis, left breast, pre-procedure left: at presentation, right: worst inflammation before injection.
Based on the waxing and waning subacute and chronic course, a presumptive diagnosis of IGM was made. Her breast surgeon recommended a systemic course of corticosteroids (methylprednisolone 24 mg with taper/Medrol Pak©), to complete the doxycycline course and follow up with repeat imaging. The patient reported improvement of pain, which quickly resumed at the end of the corticosteroid course. She was placed on a longer course of corticosteroids (prednisone 30 mg for 3 days then tapering 5 mg weekly over 6 weeks) and reported only a slight decrease in milk production.
Two weeks later, the patient developed two new areas of erythema on her breast (Figure 1, Right). Aspiration from these areas was negative (culture, gram stain, and acid fast bacilli), and she decided to proceed with the triamcinolone injection with her breast radiologist. The patient was injected with 1 mL of triamcinolone acetonide 40 mg/mL (Kenalog-40) mixed with 3 mL of 2% lidocaine (Kenalog-40). The current recommendation was to stop providing breastmilk from the injected breast after injection. 2
However, due to the paucity of evidence, the unlikely mechanism of distribution into breastmilk, and the possibility of the need for repeat injections, we established a method to collect and measure milk triamcinolone levels after the injection. We recommended 24 hours of cessation of breastfeeding after injection from the affected breast, while continuing regular milk expression and storage.
Materials and Methods
The patient collected her milk samples from the affected left breast soon after injection (time zero), 1 hour later, 4 hours later, and then daily at the same time of day for 1 week. She was instructed to donate 10 mL of pumped milk into a sample container and ship frozen milk, to The InfantRisk Center associated with Texas Tech University. Quantification of triamcinolone was determined by liquid chromatography mass spectrometry using an Agilent Zorbax column. Isocratic elution was followed using water and acetonitrile with a flow rate of 0.5 mL/min.
The precursor-product ion transition for triamcinolone acetonide m/z 435.2 > 415.1 was used. Milk samples were extracted using protein precipitation. Blank milk containing no drug concentration was spiked with appropriate concentrations of triamcinolone and internal standard for determining the calibration curve (range 0.78–100 ng/mL and r2 = 0.99). The lower limit of quantification for this assay was 0.78 ng/mL.
Results
Triamcinolone acetonide was measured in all of the milk samples up to 1 week. No triamcinolone was observed in any of the collected samples. After the injection, the patient reported intense aching pain for 24 hours, which felt better with heat and acetaminophen. She then had significant improvement in the size and pain of the mass (Figure 2, Left). Her milk production decreased on the injected left side: She had originally been able to express 60 mL on that side with an electric breast pump, and after was only able to express 10 mL. Her milk supply on the affected side recovered over the course of 2 weeks.

Post-injection improvement in inflammation left: Post-injection, right: later fistulae formation.
Production on the unaffected right side did not diminish. Her previously inverted nipple everted. The patient continued oral prednisone with a long taper of 5 mg weekly (total 8 weeks of oral corticosteroids—methylprednisolone followed by prednisone). Six weeks later, she reported pinpoint areas of mild erythema and drainage consistent with fistulae, which appeared when pumping at work, rather than when breastfeeding at home. Repeat ultrasound showed minimal fluid underlying the two new areas of fistula (Figure 2, Right). Given clinical improvement, the decision was made to stop subsequent injections. The patient remained stable and continued breastfeeding from both breasts at the 6 month follow-up visit.
Discussion
Our case demonstrates many features common to IGM, including a waxing/waning course, difficulty with definitive diagnosis, and the difficulty of treating a disease when management strategies remain controversial. 3 Our patient's initial fluid aspiration was positive for Corynebacterium, an association that has been previously described but is poorly understood. 6 Despite its benign nature, our lactating patient experienced significant pain and discomfort, with a major impact on the breastfeeding journey due to both symptoms and treatment. This patient was very motivated to continue breastfeeding and continuously sought to assess her options with respect to her ability to feed her child at the breast.
Consistent with prior findings, her milk supply was minimally affected by systemic corticosteroids. 7 However, the patient experienced a significantly decreased supply following triamcinolone injection. Decreased milk production has been reported with injection of depot forms of both methylprednisone and triamcinolone into other body parts (e.g., joints)7–9 ; our finding suggests that it may also occur after injection into the breast. Therefore, it may be preferable to begin management of IGM in lactating patients with systemic steroids rather than injection to avoid milk production concerns. Also novel is the report of nipple inversion that everted after injection.
Collaborative work with pharmacological researchers adds important data to treatment recommendations for lactating patients in that no triamcinolone was found in the milk at any time after injection. Though it is possible that different injection methods, patient physiologies, and breast pathologies may limit the generalizability of this finding, it is a reassuring finding for lactating patients with this condition.
Key features that led to a successful outcome in this case included very frequent communication with the BFLM team, in which the BFLM providers served as the “primary care” for the patient's illness course, helping with imaging appointments, referrals, coordination of care between multiple subspecialists, prescribing of the injectable triamcinolone, testing of the breastmilk for medication passage, and in the case of this patient's goals, preservation of breastfeeding.
Conclusion
A highly sensitive and specific laboratory methodology found no triamcinolone levels in the milk of the affected breast after triamcinolone injection for the treatment of granulomatous mastitis. A collaborative and patient-centered approach led to a positive outcome in our patient with IGM while lactating. Further research is warranted to determine whether our finding is replicable in other patients, and whether treatment with systemic or injected corticosteroids (or a combination of the two) results in better outcomes in lactating patients with IGM.
Footnotes
Acknowledgments
The authors would like to acknowledge the collaboration of the patient, her breast radiologist, and the lactation staff at the Breastfeeding and Lactation Medicine clinic.
Authors' Contributions
C.R.-C.: conceptualization, investigation, writing original and review, visualization, supervision; P.D.: methodology, validation, analysis, writing original and review; K.P.: conceptualization, investigation, resources; K.S.: conceptualization, investigation, writing review; T.H.: methodology, validation, supervision, writing review.
Patient Consent
Patient consent to publish, including photos, was obtained. The authors are grateful for her contribution to the literature and, thereby, the care of other patients.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this report.