
Abstract
Background:
Breastfeeding rates have stagnated recently despite recommendations to breastfeed until age 2 years. Antenatal breast milk expression (ABME) is a method used to prepare the breast for breastfeeding. However, there is limited evidence available on the benefits, risks, and impact of ABME on maternal–infant breastfeeding dyads.
Methods:
This review identified and summarized studies on women who engaged in ABME and their personal experiences. Databases searched included PubMed MEDLINE, Web of Science, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and EMBASE. Initially, abstracts and titles were reviewed, and then, full-text studies were screened for inclusion by two blinded authors. Two authors assessed the quality of the studies using a standardized tool, two authors completed data extraction, and one author completed data harmonization into tables.
Results:
A total of 1,410 studies were identified (after duplicates removed) and 10 citations qualified for the inclusion criteria. Only two studies received an overall rating of strong quality and low-risk bias. The selected articles varied in primary outcomes; however, main focuses were experiences, knowledge, and perspective after practicing ABME. Data varied on timing of ABME, but most studies started between 34 and 36 weeks. The average amount of expressed milk was reported in four studies but was variable.
Conclusions:
This systematic review found that the literature is limited regarding ABME, and most studies were focused on women with diabetes. The current limited evidence suggests that ABME may be a helpful tool in improving maternal breastfeeding confidence and breastfeeding outcomes. Negative side effects reported related to ABME included difficulty learning the technique, discomfort, and feeling of awkwardness while expressing. Future research should focus on higher quality studies regarding use of ABME, proper teaching of ABME technique, and the use of ABME to improve breastfeeding outcomes in diverse populations of maternal–infant dyads.
Introduction
Breastfeeding is the recommended sole source of nutrition for infants from birth to 6 months and continued up to 2 years with the introduction of complementary foods at 6 months.1–3 However, many mothers struggle to overcome the barriers to breastfeeding. Antenatal breast milk expression (ABME) is a method used to prepare the breast for breastfeeding. 4 ABME consists of expression and storage of milk usually starting between 36 and 37 weeks of gestation. Antenatal milk can be used as supplementation in many situations such as for infants with hypoglycemia, hyperbilirubinemia, or other situations in which formula supplementation is recommended. Pregnant women who express colostrum antenatally have reported enhancement of milk production after birth and prevention of delayed onset of lactogenesis II. 4 While ABME is a known practice that has been implemented by midwives historically, there is insufficient evidence-based research on the benefits and risks of this practice on both mothers and infants to advise it as a standard practice.
The limited research currently available on ABME is focused on mothers with complications during pregnancy such as gestational diabetes or preeclampsia in which there is usually a known reason for delayed lactogenesis II. In 2017, Forster et al published a study in which they found no harm in advising women with diabetes and minimal other pregnancy complications to express colostrum antenatally at 36 weeks pregnant and to use the milk for their infants with hypoglycemia after birth. 5 A case presentation published in 2018 by Demirci et al found that breastfeeding may be one way to counteract the negative cardiovascular sequelae of preeclampsia; however, since women with preeclampsia are at risk of premature cessation of breastfeeding, the study goes on to state that additional research is needed to address ABME as an intervention for mothers with preeclampsia and women at risk for delayed lactogenesis II. 6
In addition to using ABME to address medical complications in pregnancy that can lead to delayed lactogenesis II, there are few studies that have considered the use of ABME to boost confidence in women who want to breastfeed.7,8 The prenatal education available on ABME is limited and not standardized in existing medical practices. Current research does not address if ABME increases intention to breastfeed and to exclusively breastfeed in women with uncomplicated pregnancies, or women with known complications leading to early cessation of breastfeeding.
This systematic review was designed to gather all current evidence and existing prenatal education on ABME. The purpose was to determine what current research reveals as benefits and risks, how it affects maternal confidence with breastfeeding, and identify gaps in current research regarding ABME.
Materials and Methods
Inclusion and exclusion criteria
The study designs considered in this review included randomized controlled trials, quasi-experimental trials, retrospective studies, interviews, and surveys. Studies focusing on ABME and personal experiences with ABME were included. Studies were excluded if the focus on colostrum expression was postnatal or if the outcome assessment was not focused on ABME benefits, risks, experiences, and education.
Selection of articles
The original search was performed by a medical librarian (L.B.) and included the following databases: PubMed MEDLINE, Web of Science, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and EMBASE (Fig. 1). All databases were searched from inception to March 21, 2021. Search terminology included any controlled headings when available and keywords around the topics of (breastfeeding, colostrum, or lactation) and (education, training, or consulting) and (nutrition or diet) and (expression, storage, or pumping) (Table 1).
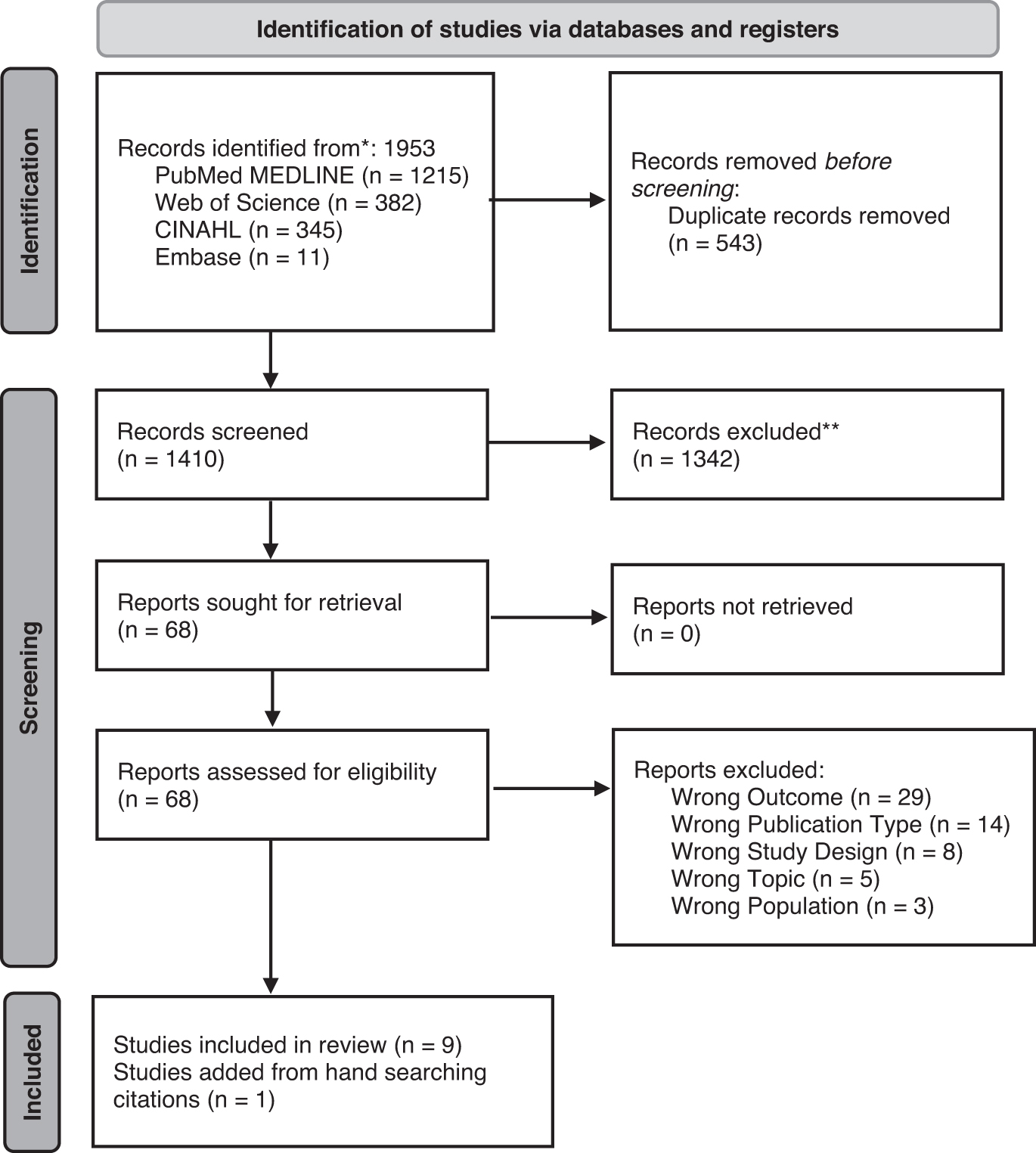
PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases and registers only. Source: Page et al. 25 For more information, visit: http://www.prisma-statement.org
PubMed Search
Citations from identified articles were downloaded from databases and combined in the EndNote X9 software (Clarivate, Philadelphia, PA, USA) for deduplication and then loaded into the online systematic review software Rayyan (Rayyan, Cambridge, MA, USA). Deduplication of citations was carried in both EndNote and Rayyan. Initial screening of titles and abstracts was conducted by three authors. Full-text screening was conducted to exclude articles due to wrong outcome, wrong publication type, wrong topic, wrong population, or wrong study design. Literature screening of the selected articles was performed to ensure that all possible citations were included.
Assessment of study quality and risk of bias
Study quality and risk of bias were assessed by two independent reviewers (S.S. and M.C.) using the National Collaborating Centre for Methods and Tools Quality assessment tool for quantitative studies. 9 This tool includes ratings (weak, moderate, and strong) for the following components: selection bias, study design, confounders, blinding, data collection methods, and withdrawals and dropouts. Studies were rated weak if two or more components were weak, moderate if only one component was weak, and strong if no components were weak. Inconsistencies were resolved with reviewer discussions to ensure a high agreement of ratings.
Data extraction and synthesis
For primary data extraction, each citation was evaluated systematically by one reviewer (S.S.). Two additional reviewers supplemented the initial data extraction with additional information (A.A. and M.C.). The original data were harmonized into four tables (Tables 1–4) by one reviewer (A.A.) that were confirmed by a second author (M.H.). Discrepancies between the reviewers regarding selection process, data extraction, synthesis, and interpretation were discussed by lead authors (A.A. and S.S.) to reach a final agreement.
Results
A total of 1,953 records were identified from PubMed MEDLINE (Table 1), Web of Science, CINAHL and EMBASE, of which 543 duplicates were removed (Fig. 1). After review of 1,410 records by co-authors (A.A., M.C., and S.S.), 68 reports were included and retrieved. Of these, 59 were excluded based on the exclusion criteria (outcome n = 29, publication type n = 14, study design n = 8, topic n = 5, and population n = 3). Data from the remaining nine reports were included in the review. An additional report was added from citation reviews, for a total of 10 studies meeting the inclusion criteria (Table 2).
Characteristics of the Included Studies
ABME, antenatal breast milk expression; EMR, electronic medical record; RIFS, Regional Infant Feeding Study.
Data were extracted from one randomized controlled trial, 5 three retrospective studies,10–12 four qualitative studies,7,8,13,14 one survey study, 15 and one case report study 6 (Table 2). Five studies focused on women with diabetes mellitus (type 1, type 2, or gestational),5,11–13,16 and most studies included only singleton and live births. Only one study surveyed either the mother or the father expecting a child or with a child younger than 1 year. 15 All other studies enrolled only mothers. Data collection methodologies varied across studies, with some using survey, 6 interview,6–8,16 electronic medical record data extraction,5,6,10–12 ABME logs, 6 or questionnaires.5,17
Following the ratings of the six steps in the National Collaborating Centre for Methods and Quality assessment tool for quantitative studies, 9 the design quality and risk of bias for each study were evaluated and are presented in Table 3. Two of the included studies received an overall rating of strong quality and low-risk bias;5,11 two studies received an overall rating of moderate quality and medium-risk bias;10,16 and six studies received an overall rating of weak quality and high-risk bias.6–8,12,13,15 The most common issues identified were related to selection bias, design, and blinding.
Quality Assessment of the Included Studies
Across studies, 69% of eligible participants were included in the analyses (Table 4). Sample size was small for five studies (N < 20 participants),6–8,13,16 medium for one study (N = 94), 12 and large for four studies (ranging between N = 294 and N = 688).5,10,11,15 Most studies reported hand expression initiation at or around 36–37 weeks of gestation.5–8,12,15,16 Other studies reported hand expression initiation between 34 and 36 weeks, 11 20 and 36 weeks, 10 or did not report time of initiation. 13 In one study, the number of women who engaged in ABME was unknown. 10 Some studies purposefully recruited women who had engaged in ABME, and therefore, they reported that all women (100%) engaged in ABME.13,14 On average, 36.5% of women engaged in ABME in the eligible survey, retrospective and qualitative studies.6–8,11,12,15 The single identified randomized controlled trial conducted in Australia demonstrated that for women who were randomized to antenatal expression group, 86% engaged in ABME compared with only 10% in the standard of care group. 5
Antenatal Breast Milk Expression Data Collection Compilation from the Included Studies
Unknown size of syringes.
One woman was not able to obtain colostrum.
N = 1.
<20 Times (N = 154), >20 times (N = 134).
ABME, antenatal breast milk expression.
Women allocated to the antenatal expression group received all standard care plus instructions on hand-expressing breast milk. 5 They were encouraged to hand express twice per day for no more than 10 minutes until admission for delivery. 5 Most studies did not report the average times women expressed milk antenatally.8,10–13,15 When reported, women antenatally expressed milk on average 17 times6,7,16 to obtain on average 2.9 mL per ABME session.5–7,16 One study reported that women obtained 6.1 syringes on average, although the syringe volume and average ABME times were not available, and therefore, total volume per session could not be calculated. 8 One study reported ABME times as a categorical variable, which could not be compared with other studies. 5 Caution should be taken in interpreting results from the volume expressed as one study reported results for only one participant. 6
Two studies identified that ABME may improve breastfeeding outcomes, 8 or breastfeeding initiation, 10 whereas one study reported no association between ABME and initiation of breastfeeding 12 (Table 5). The randomized controlled trial study demonstrated a moderate association between ABME and exclusive breastfeeding during the first 24 hours of life for first parity women only. 5 Three studies found that lactation consultants played an important role in ABME, both antenatally and postnatally. Women were more likely to engage in ABME if they attended a lactation consultation antenatally, 11 and if they engaged in ABME, they were more likely to seek postpartum lactation support 18 or seek additional education postpartum. 13
Significant Findings of Antenatal Breast Milk Expression Experiences from the Included Studies
ABME, antenatal breast milk expression; BMI, body mass index; NICU, Neonatal Intensive Care Unit.
Three studies focused on infant outcomes and ABME. There were no differences in infant outcomes between women who engaged in ABME compared with those who did not (hypoglycemia or blood glucose at 3, 12, or 24 hours, 11 Neonatal Intensive Care Unit admissions,5,12 or gestational age 12 ). Infant formula was provided in 25% of babies from women who engaged in ABME versus 57% in babies from women who did not engaged in ABME (p < 0.0001) 11 (Table 5). Women were motivated to engage in ABME by their desire to provide the best for their babies, to reduce formula use, and to avoid birth complication. 13
Five studies reported that women who engaged in ABME had greater confidence antenatally and postnatally,6–8,11 were more physically and psychologically prepared for, 13 and were more likely to commit to 7 breastfeeding. Women felt empowered when they were able to obtain colostrum and mothers were upset if formula was provided instead of using their expressed colostrum in the hospital. 16 Visualization of ABME helped provide reassurance and security for successful breastfeeding.6,7 Most women considered ABME as an acceptable breastfeeding intervention, 6 including first-time mothers. 7 Women with higher body mass index (BMI) were more likely to have heard about ABME and more likely to have a positive opinion about it. 15 One study identified that additional research is needed to evaluate ABME in mothers who develop hypertensive disorders during pregnancy. 6
Women reported that ABME can be embarrassing, awkward,8,13 and is a time-consuming process.13,16 Women felt a sense of failure or guilt as well as relentless anxiety of having insufficient colostrum if they were not able to express colostrum antenatally.13,16 Women were worried that ABME could be or was painful,11,16,19 would lose the “good stuff” (colostrum), 7 would interfere with the natural process of breastfeeding, 19 or initiate labor.7,19
Discussion
This systematic review highlights several limitations to the current research on ABME. The literature is limited with only a handful of studies and even fewer high-quality studies. Our review included 10 articles, the majority of which had a low-quality ranking and high-risk bias. The articles identified as low quality primarily had issues with selection bias, blinding, and study design. While the studies that were not randomized controlled trials were helpful in providing an understanding on perceptions of ABME, the results should be interpreted with caution.
This review highlights the differences and similarities between other breastfeeding educational resources and ABME education. In addition to standard breastfeeding education, many educational interventions for breastfeeding include the World Health Organization and United Nations International Children's Emergency Fund “Ten Steps to Successful Breastfeeding” and the Baby Friendly Hospital Initiative (BFHI). A previous systematic review has explored the effectiveness of the “Ten Steps” and BFHI. 20 The review concluded that the “Ten Steps” are in need of an update with recommendations on pacifier use and rooming-in to be revaluated.
More importantly, the review identified other factors that influence breastfeeding rates, such as socioeconomic status, ethnicity, depression, obesity, and education.20–22 The review recognized that these factors need to be considered in prenatal breastfeeding education programs. ABME intervention and education does take some of these factors into account—specifically obesity, which is often associated with diabetes, the primary AMBE inclusion factor.5,11–13,16 One article identified by this systematic review looked at both BFHI education and care and antenatal colostrum expression (ACE) education. 23 The results indicated that there was some improvement of breastfeeding rates after birth with both ACE and BFHI education; however, further investigation is needed to see the long-term breastfeeding success rates with these education methods.
While ABME may help improve breastfeeding outcomes and breastfeeding rates, there was a limited amount of literature exploring breastfeeding outcomes and breastfeeding initiation following ABME. Some studies demonstrated a positive outcome after ABME supporting the concept that ABME is beneficial in breastfeeding promotion. 8 However, this is contradicted by the results of another study, which showed that there was no significant correlation between ABME and positive breastfeeding outcomes, such as breastfeeding initiation. 6 The limited and contradictory research exploring AMBE and promotion of breastfeeding demonstrates a need for further exploration on the topic.
Much research on ABME, including the singular randomized control trial, is focused on women with diabetes mellitus. 11 Also, women who had a higher BMI, a risk factor for diabetes, were more likely to have been informed about ABME. 15 Findings in the current research on ABME is biased toward the unique and specific population studied. Yet, ABME may be beneficial for all women, and more studies should focus on other populations. In fact, women who participated in one of the studies believed that information on ABME should be available to all patients. 7
This review demonstrated a large focus of the current ABME literature on the mother's perspective of the topic.6–8,13,15,16 Among the literature, the perspective on ABME was both positive and negative. Several of the articles highlighted increased confidence in breastfeeding or feelings of greater preparation.6–8,13,15,16 Other studies demonstrated a positive relationship between confidence, self-efficacy, and breastfeeding outcomes.3,24 However, for some women, ABME had a contrary impact with a decrease in confidence and feelings of awkwardness.7,8,13,16 One aversion to ABME noted in the literature was fear of initiating early labor. This highlights a need for more research into the physiological and biological outcomes of ABME.
This review is strengthened by its systematic design, careful inclusion of studies, and evaluation of study quality and their risk of bias using published criteria. Its main limitation was the research available, with only 10 studies meeting the criteria, most of which were of low quality or with high-risk bias. The studies identified were also limited by the quality of the research as explained previously.
Conclusions
This review highlights a gap in the literature on ABME with only one randomized controlled trial that was focused on mothers with diabetes. Future studies with larger and more diverse cohorts are needed to gain a better understanding of the impact and outcomes of ABME on breastfeeding. Future studies should focus on ABME intervention in mothers with and without pregnancy complications. The focus should be on both health outcomes of the mother and infant, as well as qualitative measures, such as mothers' perceptions of ABME and her confidence toward breastfeeding. Much of the literature on ABME is focused on the experiences and perceptions of mothers who practice ABME. While this focus is helpful in understanding how mothers can benefit from ABME, a better understanding of the health outcomes of mothers and infants is needed to determine risks and benefits of ABME.
Footnotes
Authors' Contributions
S.S. participated in the literature review, drafted sections of the article, interpreted the data, and reviewed and revised the article. M.C. and A.A. contributed to the literature review, drafted sections of the article, assisted in data interpretation, and reviewed and revised the article. L.B. assisted in generating the search, loading the searing into Rayyan, and reviewed and revised the article. M.H. contributed to the literature review, and reviewed and revised the article. All authors reviewed the article critically for important intellectual content and approved the final article as submitted and agree to be accountable for all aspects of the work.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.