
Abstract
Background:
The aim of the study was to determine the effect of tea tree oil and coconut oil applied to the nipples during the early postpartum period on nipple crack formation.
Methods:
This randomized controlled experimental research included a total of 90 women in the research sample abiding by the research criteria, with 30 each in the intervention groups (coconut oil or tea tree oil application) and 30 in the control group. Women in the intervention groups applied coconut oil or tea tree oil to the nipples on the 3rd, 7th, and 10th days postpartum, whereas the control group did not have any intervention. Data in the research were collected with the Descriptive Information Form for Mothers, Early Postpartum Period Breast Problem Assessment Form, and Visual Analog Scale (VAS). Analysis of data used the chi-square test, Kruskal–Wallis test, and Friedman's test.
Results:
Mean age of women participating in the research was 28.23 ± 5.21 years. The differences between the groups applying coconut oil and tea tree oil on the 3rd, 7th, and 10th days postpartum and the control group were significant in terms of incidence of nipple cracks. In addition, the difference in mean VAS points for nipple pain in the groups using coconut oil and tea tree oil and the control group was found to be statistically significant (p < 0.05).
Conclusions:
According to the research findings, coconut oil and tea tree oil were determined to reduce nipple crack formation and nipple pain. It is recommended to increase the use of coconut oil and tea tree oil related to breast problems in nursing care during the postpartum period.
Clinical Trials Registration Number:
Introduction
During breastfeeding, nipple cracks are the most frequently encountered breast problem. The incidence of nipple cracks in the first 7 days varies from 15% to 80% globally.1,2 A study performed in Turkey reported this rate was 24.5%. 3
The most common causes of nipple cracks in the postpartum period along with nipple pain, reddening of breast tissue, white cracks, or bleeding 1 are mistaken breastfeeding techniques and not performing correct nipple care.4,5 In addition, the use of a breast pump with excessive pressure, the infant pulling off the nipple, tongue tie, and candida infections may cause nipple cracks.6,7
Some applications and cosmeceutical products were reported for use in prevention and treatment of breast problems in the postpartum period. The most frequently used among these are tea compresses, local hot and cold application, mint juice, lanolin and hydrogel dressings, olive oil, raw onion, henna, lipstick, butter, coconut oil, cream, and mevzer oil.8–11 Coconut oil, assisting in preserving the moisture content of skin and containing saturated fat, is a fully natural moisturizer nourishing the skin without damage. 12 Coconut oil increases protective barrier functions on the skin, has anti-inflammatory and antibacterial properties, and was reported to have active protective effect against Candida albicans. 13
Tea tree oil, another herbal product, contains terpinen-4-ol and cineol responsible for antimicrobial and antifungal activity.14,15 It simultaneously has natural antibiotic properties. 16 It is reported to provide natural vitality to the skin. 14 Owing to having similar properties to lanolin pomades used to prevent cracks forming on the nipples, tea tree oil is thought to be effective in preventing nipple cracks. In addition, positive results were reported from the treatment of nipple cracks with coconut oil 5 ; however, there is no study encountered about preventing nipple cracks.
Nipple cracks are the most common cause of women stopping breastfeeding. 17 Cessation of breastfeeding deprives the infant of essential nutrients, growth factors, and important immunological components in breast milk. 18 It is important to inform pregnant cases before birth about nonpharmacological (breast milk, etc.) and pharmacological (lanolin, madecassol, etc.) methods and effects when applied to nipples before and after birth. 19
In recent years, use of herbal products has increased in our country as well as all over the world. When the literature was examined, no study was found on the dermatological use of coconut oil and tea tree oil in the postpartum period and the prevention of nipple cracks. For this reason, this study is thought to contribute to the literature about preventing nipple cracks during breastfeeding.
Materials and Methods
Research aim
To determine the effect of tea tree oil and coconut oil applied to the nipples in the early postpartum period on formation of nipple cracks.
Research hypotheses
Research type
This was a randomized controlled experimental study. This randomized, controlled single-blind study was completed in the Gynecology and Obstetrics ward of a private hospital in the Black Sea region of Turkey from January to December 2021.
Research population and sample
The population for the study comprised birthing mothers admitted to the Gynecology and Obstetrics ward of a private hospital in the Black Sea region of Turkey. The G-Power 3.1.9.2 program was used for sample determination in the population. Based on the study by Sağlık and Kısacık, the effect size was 0.5 and to obtain 95% confidence and 95% power, it was determined that each group should contain 27 women for a total of 81 mothers to be adequate. 20 Considering data loss during the study process, 10% above the calculated sample size was included and the study included a total of 90 mothers abiding by the research criteria (Fig. 1). Before consent was obtained from the participants, it was questioned whether they would use any agent on the nipple. Those who stated that they did not intend to use it were included in the study. During data collection, six women from the control group were excluded from the study because they stated that they used pharmacological agents. Instead, six participants were included in the study again.
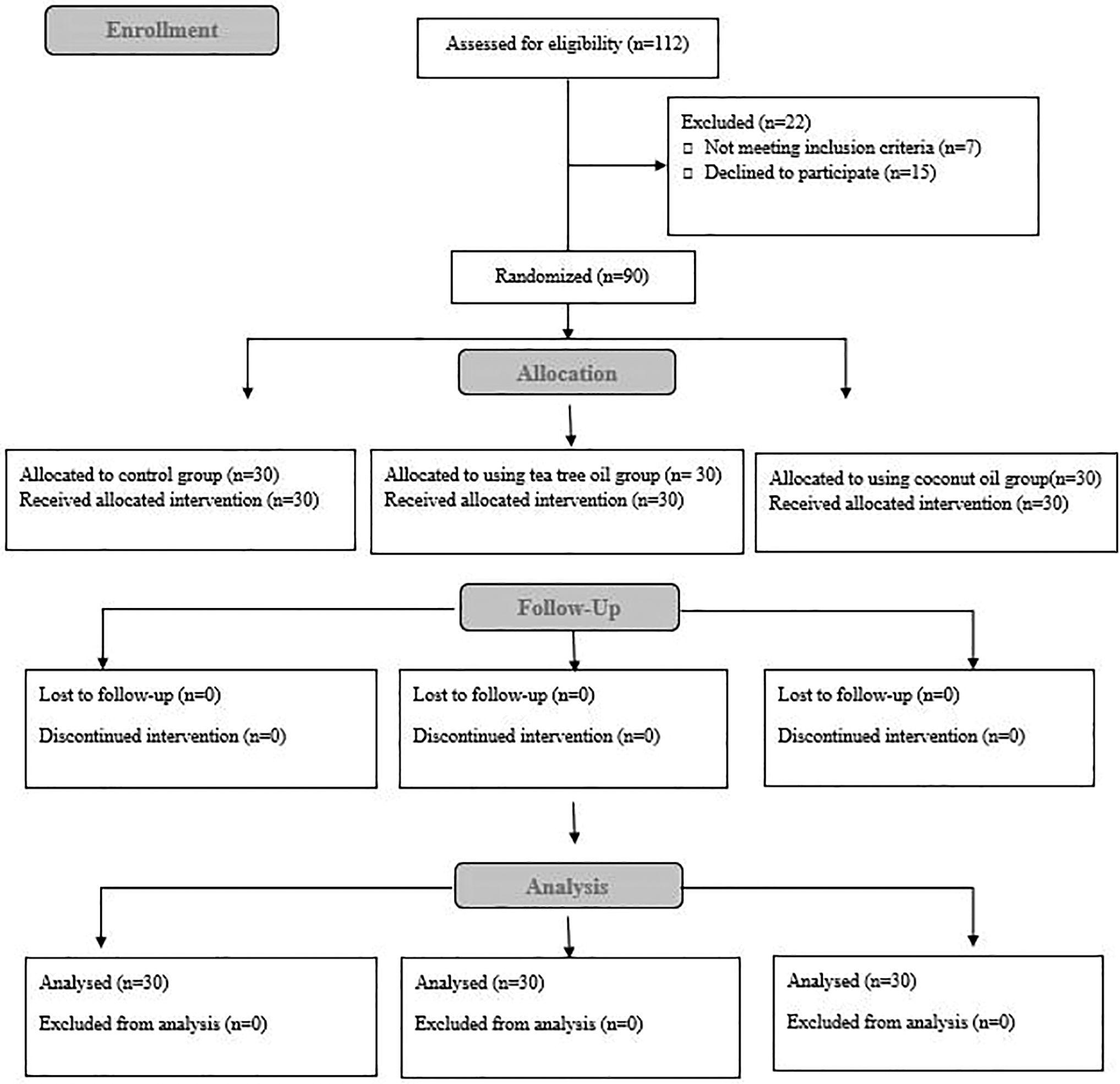
Consort flow diagram.
Inclusion criteria for the research
Mothers who volunteered for participation, could speak Turkish, were aged from 18 to 35 years, with new and live birth after 37 weeks, without flat or small nipple problems, without previous breast operations, able to apply correct breastfeeding methods, and with infants with birth weight of 2,500 g and above were included in the study.
Exclusion criteria for the research
Mothers who could not breastfeed, had stillbirth, had to use pharmacological agents, and who had infants with congenital anomalies preventing breastfeeding were not included in the study.
Randomization
The study included women admitted on Mondays into the first intervention group, women admitted on Wednesdays to the second intervention group, and women admitted on Fridays to the control group to ensure randomized sample selection.
Data collection tools
Collection of data in the research used the descriptive information form related to the mother developed by the researchers in line with the literature and with expert opinion, the Early Postpartum Period Breast Problems Assessment Form, and the Visual Analog Scale (VAS).
Descriptive information form related to the mother
This form created by the researchers comprised 11 questions about sociodemographic characteristics like mother's age, educational level, income level, and employment status and also about type of birth, frequency of breastfeeding, when breastfeeding began, and previous breastfeeding history.
Early postpartum period breast problems assessment form
This form was prepared to assess whether there were cracks around the nipple and comprised one question asked on postpartum days 3, 7, and 10.
Visual analog scale
The VAS developed by Gablenz et al is a visual scale to assess the severity of pain. 21 The scale has Cronbach alpha coefficient of 0.916. Adaptation of the scale to Turkish and validity and reliability studies were performed by Yaray et al and the VAS was reported to have Cronbach alpha coefficient of 0.965 and high reliability. 22 It is assessed on a line with 10 cm length marked at 1 cm intervals. On the scale, 0 cm represents no pain, 5 cm moderate levels of pain, and 10 cm unbearable pain. The scale was used to assess the severity of nipple pain perceived by mothers.
Research procedure
First Interview: Within the first 24 hours after birth, mothers were interviewed, communication numbers and written consent were obtained, and the descriptive information form related to the mother was applied.
Second Interview: On the 3rd day postpartum, mothers were interviewed by telephone and the VAS and early postpartum period breast problems assessment form were applied.
Third interview: On the 7th day postpartum, mothers were interviewed by telephone and the VAS and early postpartum period breast problems assessment form were applied.
Fourth interview: On the 10th day postpartum, mothers were interviewed by telephone and the VAS and early postpartum period breast problems assessment form were applied.
Intervention and control group protocols
Control group: They were told that no intervention would be performed, and that they should not use any application like herbal or chemical oils, creams, medications, and so on, on the nipples during the first 10 days postpartum.
Intervention groups: They had the application method along with information about the oil to be used explained and given in written form, as shown hereunder.
✓ Wash hands with soap before each feed
✓ Wash nipples with water
✓ After feeding, wash hands and apply two drops of oil, coconut oil in the first intervention group and tea tree oil in the second intervention group, to the index finger and spread on the areola and nipple
✓ Leave the nipple to dry for a few minutes
✓ Continue this application for 10 days.
Ethical aspect of the research
The study began after receiving institutional permission and ethics committee permission dated February 27, 2020 and numbered 2020-27 from Hitit University Non-Interventional Research Ethics Committee. The study was completed according to the 1975 Declaration of Helsinki revised in 2000 and written informed consent was obtained from people included in the study.
Statistical analysis of data
Analysis of data used the SPSS 21 (SPSS, Inc., Chicago, IL) program. For analysis of data, descriptive statistics are given as mean and standard deviation for continuous variables and as frequency and percentage for categorical variables. Skewness-kurtosis values and the Shapiro–Wilk test were used to assess whether data displayed normal distribution. Comparisons of independent groups of categorical variables used the chi-square test, whereas comparison of ranked data between groups used the Kruskal–Wallis test. Friedman's test was used to assess variability within and between groups for two-way repeated-measures numerical variables. The p value for significance level was taken as 0.05.
Results
In the study, the mean age of women in the control group was 28.23 ± 5.21 years with mean partner age of 32.03 ± 5.46 years; mean age of women in the tea tree group was 31.20 ± 6.59 years with mean partner age of 32.36 ± 8.82 years; and mean age of women in the coconut oil group was 32.00 ± 5.47 years with mean partner age of 33.90 ± 6.01 years.
In the control group, 53.3% of mothers and 46.7% of partners were undergraduates or above, 70% had income perception of being equal to expenditure, and 60% were employed. In the group using tea tree oil, 46.7% of mothers and 40% of partners were high school graduates, 56.7% had income perception of being equal to expenditure, and 60% were employed. In the group using coconut oil, 53.4% of mothers and partners were high school graduates, 56.7% had income perception more than expenditure, and 63.3% were employed.
In the control group, 76.7% of mothers had cesarean births, 63.3% gave birth to their first child, 70% began breastfeeding within the first 10 minutes, 43.3% had breastfeeding frequency of once every 1–2 hours, and 45.4% had nipple cracks from during previous breastfeeding. In the group using tea tree oil, 53.3% of mothers had vaginal birth, 40% had their first child, 53.3% began breastfeeding within 10–30 minutes, 46.7% had breastfeeding frequency of once every 1–2 hours, and 46.1% were identified to have nipple cracks during previous breastfeeding. In the group using coconut oil, 50% of mothers had vaginal birth, 56.7% had their first child, 70% began breastfeeding in 10–30 minutes, 36.7% had breastfeeding frequency of once every 1–2 hours, and 72.2% had nipple crack formation during previous breastfeeding.
When investigated in terms of breastfeeding frequency, the difference between the groups was found to be significant (p < 0.05), whereas the differences between the groups in terms of age, educational level, partner age, partner educational level, income perception, employment status, type of birth, number of children, duration to starting breastfeeding and nipple crack formation during previous breastfeeding were not identified to be statistically significant (p > 0.05) (Table 1).
Distribution of Mothers According to Some Sociodemographic and Obstetric Characteristics
Coconut oil applied group.
Tea tree oil applied group.
p < 0.05.
KW, Kruskal Wallis.
In the control group in our study, nipple cracks were observed in 46.7% of mothers on the 3rd day, 66.7% of mothers on the 7th day, and 60% on the 10th day. In the group using tea tree oil, nipple cracks were observed in 13.3% of mothers on the 3rd day, 13.3% of mothers on the 7th day, and 3.3% of mothers on the 10th day. In the group using coconut oil, nipple cracks were identified in 6.7% of mothers on the 3rd day, 13.3% of mothers on the 7th day, and 13.3% of mothers on the 10th day. In the research, the differences in nipple crack formation on the 3rd, 7th, and 10th days in the intervention and control groups were found to be statistically significant (p < 0.05) (Table 2). The differences on the 3rd, 7th, and 10th days were identified between the control group and tea tree group and the control group and coconut oil group.
Distribution of Mothers According to the Incidence of Nipple Cracks
Coconut oil applied group.
Tea tree oil applied group.
p < 0.05.
In the study, there were statistically significant differences between the intervention and control groups according to mean VAS points for mothers using coconut oil and tea tree oil (p < 0.05). Compared with the control group, the intervention groups were concluded to have reduced nipple pain as the days progressed (Table 3).
Distribution of Mothers' Visual Analog Scale Mean Scores by Days
Coconut oil applied group.
Tea tree oil applied group.
p < 0.05.
VAS, Visual Analog Scale.
Discussion
Problems like nipple cracks and nipple pain are significant in women in the early postpartum period and are a significant obstacle for effective and successful breastfeeding.17,20 In general, nipple pain is reported to be experienced most in the first week postpartum.11,23,24 Treatment of nipples injured at the start of the breastfeeding period is difficult and time-consuming. For this reason, it is very important to prevent nipple cracks before formation. 25 Studies testing the efficacy of topical treatments to prevent nipple cracks in breastfeeding women in the early postpartum period (lanolin, olive oil, breast milk, mint oil, etc.) showed these methods do not only keep the nipple dry and clean, but reduce cracking.9,11 In addition, there is no definite evidence about which method is most effective.
In this study, the effects of coconut oil and tea tree oil in preventing nipple cracks were researched. In our study, mothers in the control group were observed to have proportionally more nipple cracks on all observation days compared with mothers in the intervention groups. The intervention groups applying tea tree oil or coconut oil were determined to have less nipple cracks compared with the control group at significant levels. In the literature, breast milk was reported to be used as an effective natural method for prevention and treatment of both nipple cracks and breast pain owing to it containing anti-inflammatory, antibacterial, and antimicrobial agents.13,26,27 These findings lead to the consideration that tea tree oil with antifungal, antibacterial, and antimicrobial content and coconut oil with anti-inflammatory, and antibacterial content will be effective in terms of preventing nipple cracks, like breast milk.
In this study, the mean VAS points for mothers in the control group were high by significant levels compared with the mean points for mothers in the intervention groups on all observation days. In the study, the intervention groups using tea tree oil and coconut oil were found to have less nipple pain compared with the control group. Some studies applied lanolin cream to the nipples and reported reduced nipple pain.2,28,29 When breast tissue is traumatized, chemicals like histamine and bradykinin are released in this region and cause pain. Lanolin increases healing by preserving the moisture in the injured tissue and reduces the amount and duration of exposure to these chemicals; thus, it may lessen pain. 30 These properties of lanolin support the results that tea tree oil with antifungal, antibacterial, anti-inflammatory, and antimicrobial content and coconut oil with anti-inflammatory and antibacterial content will reduce nipple pain.
Conclusion and Recommendations
The control group, while matched for sociodemographic and obstetric variables, was not randomly selected but was self-selected, raising a concern that there was a hidden selection bias. There is a need for evidence-based nursing practices for initiation of breastfeeding, continuation in a healthy way, and to solve problems related to breastfeeding. In this study, coconut oil and tea tree oil were concluded to each be reliable methods for use to prevent nipple crack formation, reduce nipple pain, and resolve nipple problems. In this context, there is a need for randomized controlled experimental studies with greater scope and larger samples related to lactation and breastfeeding problems.
Footnotes
Acknowledgment
The authors thank the participants for their support of the study.
Authors' Contributions
All authors have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be submitted.
Ethical Approval
The study was initiated after obtaining approval of the Ethics Committee for Non-Invasive Research of Hitit University. Written informed consent was obtained from the fathers included in the study.
Disclaimer
The findings and conclusions in this report are those of the authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.