
Abstract
Objective:
This study investigated changes in sodium concentrations in human milk from mothers of premature infants using different breast pumps for 14 days postpartum, and the correlation between the sodium concentration in mother's own milk (MOM) and the volume pumped.
Study Design:
This randomized controlled study recruited 66 mothers of premature infants delivered in our hospital from February to December 2018, and we assigned them to three groups using an envelope method. In intervention group 1, a hospital-grade electric breast pump was used from postpartum day 1 to 14; in intervention group 2, a hospital-grade electric breast pump was used on postpartum days 1 to 5 and a normal personal electric breast pump on postpartum days 6 to 14; in the control group, a personal normal electric breast pump was used from postpartum day 1 to 14. Data recorded included the breast milk volume pumped and milk sodium concentration.
Results:
The average daily volume of MOM pumped differed statistically (p < 0.05) between the intervention and control groups at postpartum days 7 and 14. The average daily volume pumped did not differ between intervention groups 1 and 2 by postpartum day 14 (p > 0.05). However, the time taken for the sodium concentrations to normalize differed significantly (p < 0.01). At postpartum day 5, the sodium concentrations of 73% of intervention group 1 and 2 mothers were within normal limits, and they were maintained until day 14. In comparison, only 41% of the controls had normal MOM sodium levels on day 5, and they were still high on day 7 in 27.3% of controls.
Conclusions:
In the early stage of lactation initiation (within 5 days postpartum), using a hospital-grade electric breast pump promotes lactation in mothers who deliver prematurely and the sodium concentrations normalize more quickly. Sodium can be used as an objective biomarker of MOM to evaluate the possibility of delayed lactation in mothers of premature infants, and it could assist interventions in the early postpartum period.
Trial Registration:
Chinese Clinical Trial Registry, ChiCTR2200061384.
Introduction
Premature delivery is a global public health issue, 1 and the main cause of death in children under 5 years old worldwide. 2 For premature infants, mother's own milk (MOM) is prescribed for immune replacement therapy 3 ; its other bioactive and nutritional properties specifically reduce death and preventable morbidities in preterm infants such as necrotizing enterocolitis, bronchopulmonary dysplasia, etc.4,5
Interventions within 1 hour postpartum and frequent milk sucking (≤8 times/24 hours) are necessary in mothers of premature infants to produce colostrum and establish secretory activation. 6 Studies indicate that lactation induction by a breast pump is more effective than by hand. 7 However, many clinics lack breast pumps. 8
Lactogenesis is divided into lactogenesis I and II. Lactogenesis I begins during pregnancy; mammary gland epithelial cells start to differentiate into lactocytes, between which tight junctions (TJs) have not yet formed, whereas the paracellular pathways (PCPs) open. At this stage, the mammary gland secretes a small amount of colostrum rich in bioactive substances. Lactogenesis II is reached when milk secretion is clinically activated following delivery; TJs form between secretory cells and the PCPs close gradually. 9
Acinar milk is sequestered from the cellular matrix, with no exchange of substances inside and outside of acini. The increased osmotic pressure of acini leads to water influx, mammary gland activation, and copious milk secretion. The onset of copious milk secretion that occurs after 72 hours postpartum is called delayed lactogenesis, 10 which is prevalent in preterm mothers. 11 Without effective interventions, secondary lactation failure occurs. Electric breast pumps facilitate milk secretion and accelerate lactogenesis. 12
It is difficult to predict whether breastfeeding will be successful, and secretory activation normal, at 1 week postpartum because these outcomes depend heavily on maternal perception and breast pump assistance. Therefore, effective methods to determine high-risk individuals (i.e., those with delayed or failed lactogenesis) are important, especially for preterm mothers with early signs of insufficient lactogenesis. 13 Secretory activation is closely related to TJ closure in mammary gland epithelial cells, 14 and the concentrations of biomolecules in breast milk change during lactogenesis II (e.g., increased lactose and decreased sodium). 15
Such changes can occur 36 hours before the surge in milk volume, and a drop in the sodium concentration predicts successful lactation. 16 A prolonged time for sodium concentrations to fall or elevate indicates lactogenic malfunction or failure. Studies have attempted to quantify secretory activation by analyzing breast milk biomarker concentration curves, 17 and to identify individuals at high risk of delayed or failed lactogenesis.
Mothers who are thought to have successfully completed secretory activation may remain at risk of early insufficient lactogenesis 17 ; this randomized controlled study monitored preterm mothers using different breast pumps for 14 days postpartum. By analyzing sodium concentrations before and after secretory activation, we investigated the relationships among sodium concentration, milk volume, and lactogenesis in preterm mothers after maternal–infant separation, to facilitate prospective, personalized, and efficacious interventions for lactation.
Methods
Study design and participants
This single-center randomized controlled study enrolled 66 mothers of premature infants delivered at a tertiary obstetrics and gynecology hospital in Zhejiang Province, China between February and December 2018. Data were collected over 14 days postpartum. In our hospital, mothers were given comprehensive breastfeeding support in the Obstetrics Department and neonatal intensive care unit (NICU) during both hospitalization and postpartum. Breastfeeding support involves outpatient services, specialized staff at the breast milk bank, food-grade milk storage containers, special refrigerators for breast milk, and breast milk analyzers.
The inclusion criteria were willingness to breastfeed, infant gestational age of 28–35 weeks, anticipated NICU stay of ≥15 days, and mother aged 20–40 years. The exclusion criteria were positive for human immunodeficiency virus, syphilis, hepatitis B, active tuberculosis, or other contagious diseases; expected stillbirth; potential severe contradictions to breastfeeding (major physical, surgical or infectious diseases); puerperal mothers with abnormal mammary gland maturation; and a history of psychosis or severe cognitive impairment.
Participants were excluded from the analysis if they showed poor compliance, refusal to cooperate, or voluntary dropout; newborns for whom treatment was abandoned, and those who died after birth, were also excluded, along with cases with incomplete observations for any reason.
The study was approved by the Ethical Committee of the Women's Hospital School of Medicine (20170185). The study was registered in the Chinese Clinical Trial Registration System (www.chictr.org.cn; ChiCTR2200061384). Randomization was completed by a blinded research assistant using opaque sealed envelopes. After providing informed consent, the puerperal mothers were divided randomly into three groups (all n = 23).
Intervention group 1 used a hospital-grade electric breast pump on postpartum days 1–14. Intervention group 2 used a hospital-grade electric breast pump on postpartum days 1–5, and personal electric breast pumps on days 6–14. The control group used a normal electric breast pump on postpartum days 1–14.
Interventions
The enrolled preterm mothers were given evidence-based lactation care and support by the NICU nurses. All mothers were educated on breastfeeding and breast pump use 1 hour after delivery. Mothers in intervention group 1 were shown how to stimulate lactogenesis using a hospital-grade electric breast pump, signed a rental contract with research staff before leaving the hospital, and used the hospital-grade electric breast pump at home until postpartum day 14.
The hospital-grade electric breast pump programs used were “INITIATE” and “MAINTAIN.” 18 INITIATE was used before the mother pumped ≥20 mL during three consecutive pumping sessions. MAINTAIN mode was used thereafter. If there was delayed secretory activation, the MAINTAIN program was automatically switched on after 5 days postpartum, in combination with maximum optimal negative pressure to assist pumping. 19
Mothers in intervention group 2 used the hospital-grade electric breast pump when in hospital or at home (if hospitalized for <5 days), and then switched to a standard household breast pump until day 14. The controls used only a household breast pump for 14 days. Mothers were encouraged to pump milk every 2–3 hours (8–12 times per day). When milk was still flowing, the mother continued pumping for 2 minutes after the flow of milk ceased.
Milk volume was quantified with medical scales by mothers after each completed pumping session. Milk expression was documented meticulously for 14 days after delivery (the first 24 hours postpartum was day 1). Pumping times, pumping length, milk volume from each breast, swelling before and after pumping, and the pumping method were recorded on a logbook that was given by the research nurse.
MOM samples
Mothers were provided with pre-weighed (to the nearest 0.1 g) MOM storage containers. After filling, the containers were brought to the NICU. The researchers took 1–2 mL of breast milk from the storage bottle twice a day, and they added four samples per day (from the left and right breasts, about 12 hours apart) to graduated centrifuge tubes (weighed to the nearest 0.1 mL) for the first 14 days postpartum.
Not all mothers had sufficient MOM for twice-daily sampling, especially for the first few days after delivery; we always prioritized MOM for infant feeding when volumes were low, and we did not take samples in such cases. Each MOM sample was labeled (name, time, and date) and stored in a freezer at −20°C to ensure sample integrity.
Laboratory analysis of MOM biomarkers
“Selective ion testing” was used to analyze the MOM sodium concentration
(HORIBA, Japan); this method has been validated in the context of flame photometry of milk according to national food safety standards. 20 Frozen samples were thawed for 1 hour at 37°C and shaken to mix the milk; then, 0.5 mL was pipetted onto a “sodium ion selective” electrode sensor pad. The value was recorded, and the sensor pad was then cleaned with ultrapure water and wiped with disposable paper before the next measurement. All samples were tested twice; if the two results differed by >10%, the test was repeated and the mean of the two measurements was used in the analysis.
Data acquisition
The primary outcome was the changes in sodium concentration in MOM in preterm mothers. The secondary outcome was the daily milk volume by postpartum day 14. Trained researchers also recorded the mother's age, gestational week, mode of delivery, and prenatal body mass index (BMI), as well as the infant's birth weight and Apgar score.
Statistical analysis
Data were analyzed using SPSS software (ver. 22.0; IBM Corp., Armonk, NY). Numerical data are presented as percentages (%) and were analyzed using the chi-square test. Continuous data are presented as the mean ± standard deviation (
All clinical and laboratory data were entered into Excel (Microsoft). Pumped MOM volume and sample characteristics were summarized with descriptive statistics. The mean daily values of each biomarker were calculated by averaging the results of both daily MOM samples (when there was more than one sample on a given postpartum day; 00:00–23:59).
Res ults
General information about the study subjects
Initially, 69 puerperal mothers consented to participate, but one dropped out due to a surgical condition, one was lost to follow-up halfway through the study, and another had poor compliance. The study enrollment flow chart is shown in Figure 1. Sixty-six preterm mothers completed the study; their mean age was 29.83 ± 4.04 (range: 20–40) years. There were 25 primiparas (38%) and 41 multiparas (62%); 48 mothers had singleton pregnancies, 18 had twin placentas, and 23 had experience of breastfeeding (35%). The delivery was vaginal in 17 (26%) cases, and cesarean in 49 (74%). The gestational age of the premature infants was 32.22 ± 1.55 (range: 29–35) weeks, and their mean birth weight was 1767.95 ± 279.23 (range: 1,000–2,500) g.

Flowchart of study enrollment.
The gestational week, age, BMI, breastfeeding experience, mode of delivery, gravidity, birth weight, and Apgar scores of the preterm babies did not differ statistically among the three groups (p > 0.05) (Table 1).
Subject Characteristics (N = 66)
BMI, body mass index; SD, standard deviation.
Daily milk volume by postpartum day 14 in the three groups
The daily average milk volume increased steadily over the first 14 days postpartum in all three groups (Fig. 2). In the intervention group 1, 21 (95%) mothers successfully “came to volume” (milk volume ≥500 mL/day on postpartum day 14) 21 within 14 days; 18 (82%) mothers in intervention group 2 came to volume, whereas this was the case for only 10 (45%) control mothers. The daily milk volume differed among the three groups between postpartum days 6 and 14 (p < 0.05). The average daily MOM pump volume differed statistically among the three groups at postpartum days 7 and 14 (p < 0.05) (Table 2).
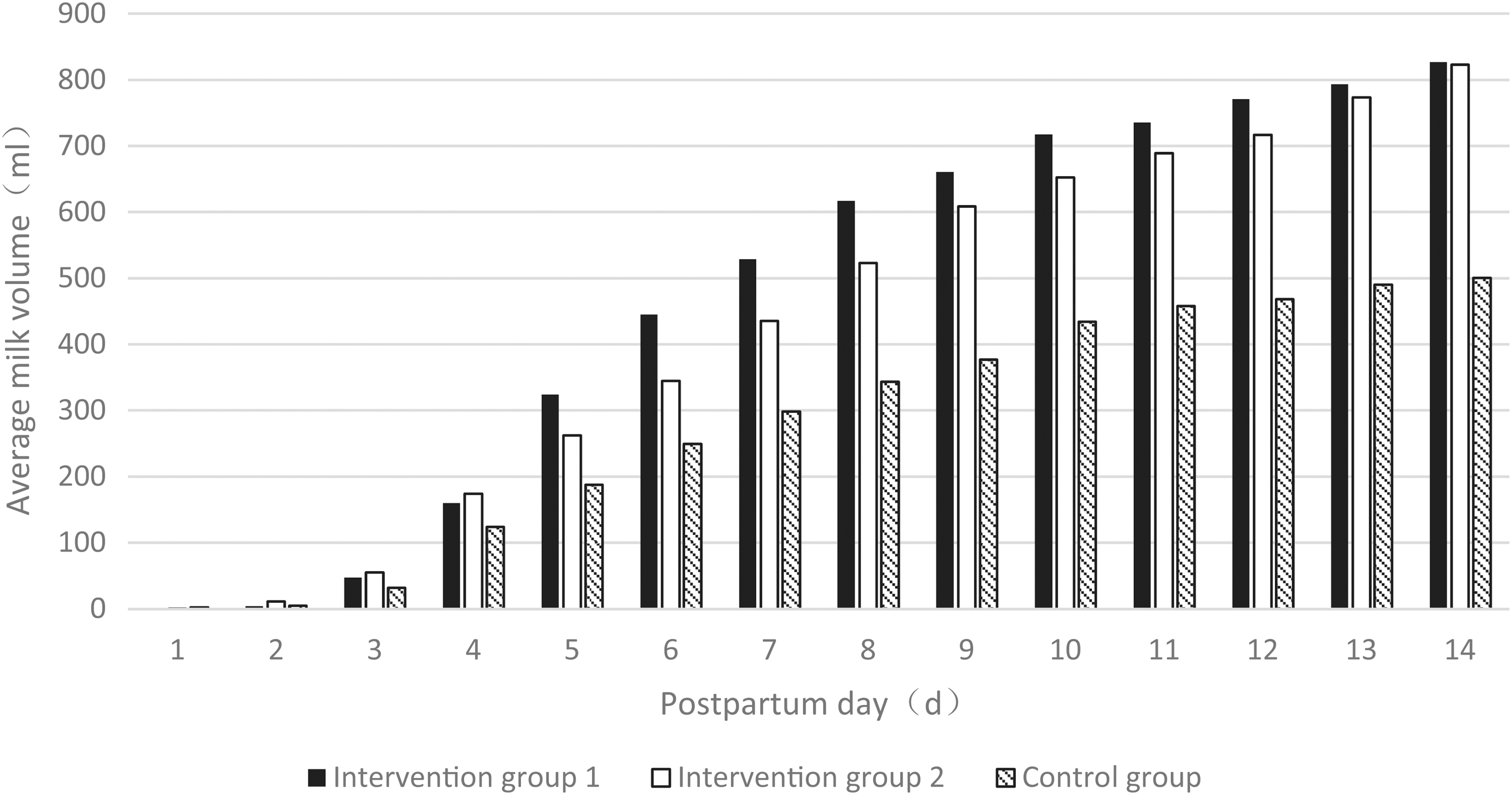
Daily average milk volume within 14 days postpartum in three groups.
Average Daily Milk Volume in Three Groups at Postpartum Day 7 and 14
Changes in sodium concentration in MOM
In total, 2,370 MOM samples were collected (mean = 36 [range: 24–48] samples per mother). None of the 66 preterm mothers provided an MOM sample on postpartum day 1; 9 mothers provided their first MOM sample at day 2, 26 (39%) on day 3, and 29 (44%) on days 4–6. As some of the preterm mothers had little breast milk initially, MOM collection was preceded by the feeding of premature babies.
Figure 3 shows the change in median sodium level of MOM during the first 14 days postpartum in the three groups. In this study, the MOM sodium concentrations in the three groups were in the normal range on 4.45 ± 1.37, 4.95 ± 1.25, and 5.95 ± 1.88 days, respectively (p = 0.006). Although there was a significant difference between the intervention and control groups (p < 0.05), there was no difference between the intervention groups (p = 0.282).
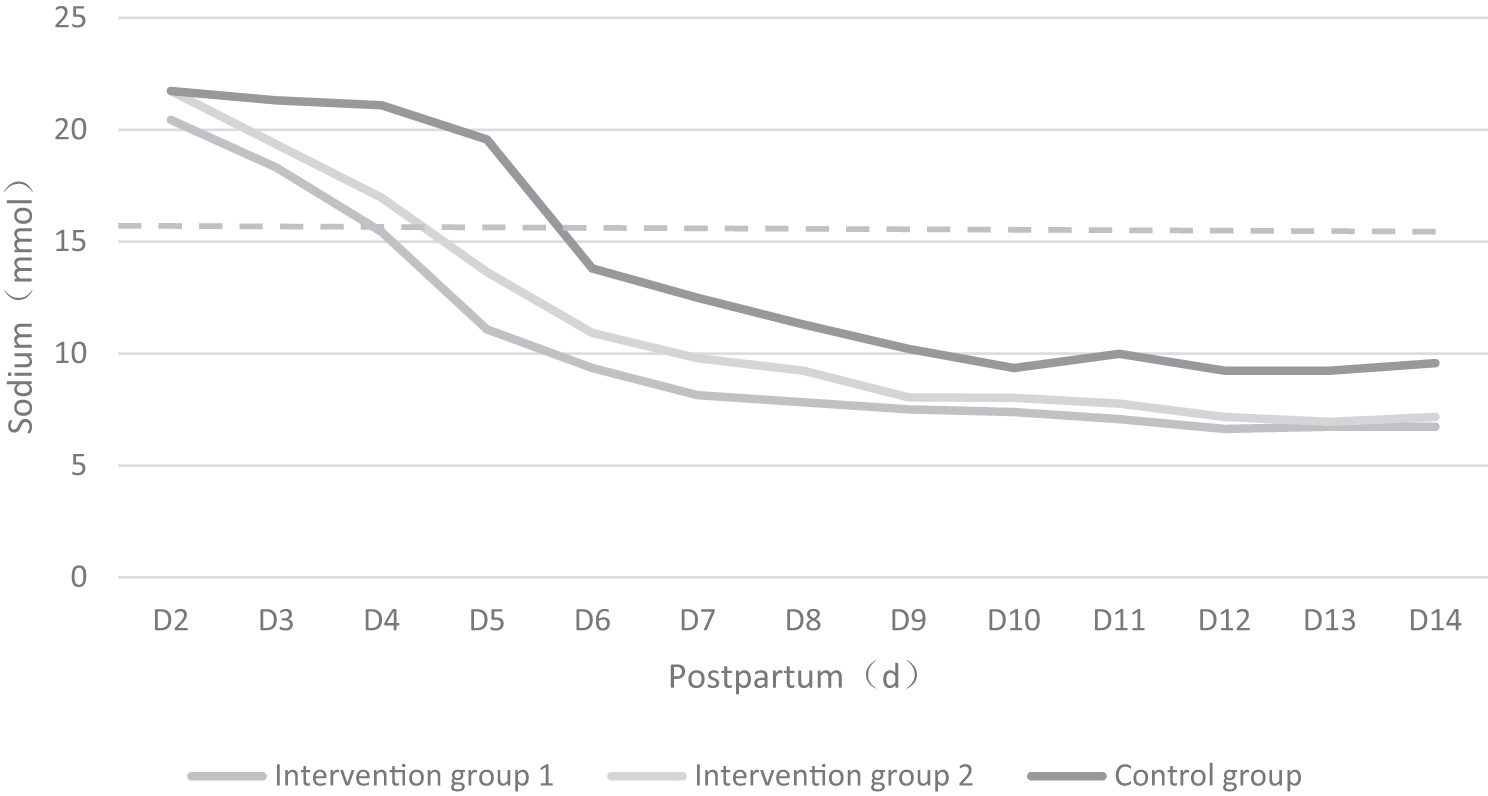
Sodium concentrations in MOM within postpartum day 14 among three groups. MOM, mother's own milk.
We categorized the 66 mothers into 6 groups of 11 according to the milk volume for 14 days postpartum, and we analyzed the sodium level and milk volume in the groups with the highest and lowest milk volumes. The sodium level showed the opposite trend to the milk volume.
In the group with the highest milk volume (Fig. 4), the sodium level fell dramatically and leveled off after day 4. The daily milk volume exceeded 500 mL on postpartum day 6 and increased to 1322.72 mL on day 14. By contrast, in the group with the lowest milk volume (Fig. 5), the sodium concentration decreased more gradually, indicating delayed lactogenesis and prolonged or incomplete PCP closure. On postpartum day 14, the daily milk volume was 266.64 mL (<500 mL/day).

Group with the highest milk volume (n = 6).
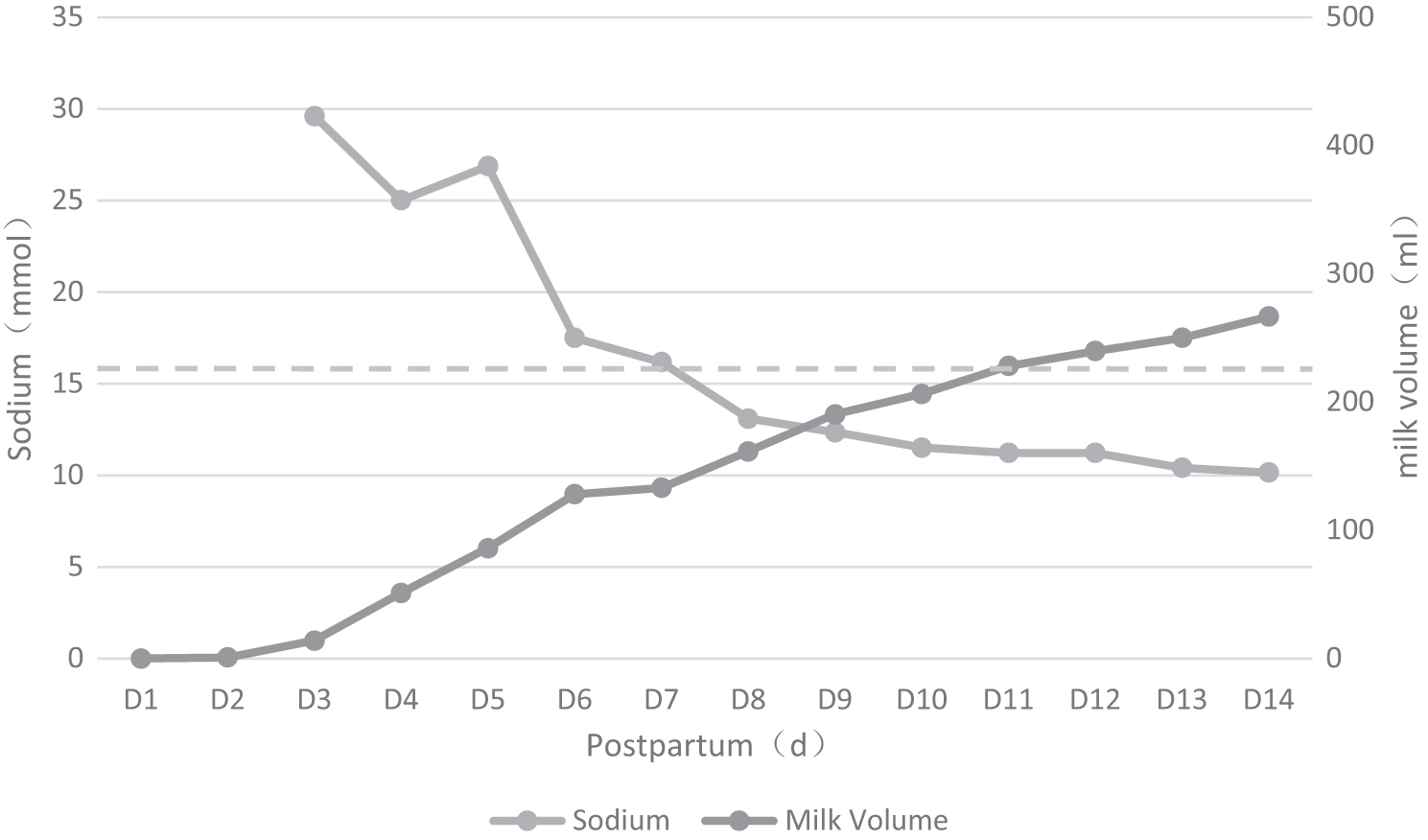
Group with the lowest milk volume (n = 6).
Discussion
This is the first Chinese study to measure MOM sodium concentrations and milk volume for 14 days postpartum in the mothers of premature infants. We investigated the effects of three pumping methods on lactogenesis in preterm mothers and sodium fluctuations in breast milk. Sufficient breast milk production occurs when the milk volume is ≥500 mL/day on postpartum day 14, and it predicts sustainable breastfeeding at NICU discharge. 22
We found that the daily average milk volume of the 66 preterm mothers increased continuously for 14 days after delivery, although the milk volume at day 14 in the control group was low compared with the intervention groups, implying that the hospital grade breast pump improved milk secretion during postpartum lactation (14 days after delivery). 12 And most importantly, the different pump regimens of breast pump use play an important role in these processes, which allowed us to study the role of sodium concentration as a marker for measurement.
Sodium was used as a biomarker of secretory activation because it can be rapidly and accurately measured, and the concentration is not affected by the mother's diet, method of milk expression, or sample collection time (foremilk versus hindmilk); moreover, it is a universally used lactation marker.23,24 Morton reported that sodium concentrations ≤16 mmol/L (368 ppm, 1 mmol = 23 ppm) on postpartum days 3–8 were normal, whereas interventions were needed in cases with higher levels. 25
In this study, MOM samples received within 24 hours were not substantially different between the left and right breasts (p > 0.05), similar to a study of MOM biomarkers in the context of premature delivery. 24 However, that study only collected data for 5 days after delivery. Another study assumed that sodium levels dropped drastically when the milk volume surged at the onset of lactation. 26 In line with this, we found that the sodium concentration decreased in all three groups of preterm mothers over time. Specifically, in intervention groups 1 and 2, the MOM sodium concentrations fell rapidly during the first 4 days after delivery, whereas the milk volume increased.
By contrast, the sodium decreased more gradually in the control group and normalization was delayed compared with the intervention groups. On postpartum day 7, the MOM sodium levels leveled off and were sustained in all three groups. Typically, sodium concentrations decrease rapidly during the first 3 days postpartum, and abnormal rebound at day 7 is considered a risk factor for the cessation of breastfeeding. 27
Thus, sodium levels in early postpartum lactogenesis are an adjuvant marker of milk volume to identify and manage mothers in this high-risk population. The higher the initial sodium concentration, the more time is needed for it to fall to normal levels and the lower the possibility of coming to volume, which makes interventions that lead to a rapid decrease in sodium concentrations to seem most effective.
The quantity and timing of normal biomarkers for secretory activation are closely related to successful lactation in the critical postpartum period. Other studies measuring MOM biomarkers in preterm mothers found that mothers with higher pumping frequencies during the first 14 postpartum days had more MOM biomarkers with normal concentrations and higher pumped milk levels, which indicates a dose-response relationship between the number of normal MOM biomarkers and pumped MOM volume at postpartum day 5.17,28
In our study, 75% of the preterm mothers in intervention groups 1 and 2 had normal sodium concentrations 5 days after delivery, which were maintained until day 14. By contrast, only 41% of MOM in the control group had normal sodium levels at postpartum day 5; in 27.3% of the controls, the MOM sodium concentrations were still higher than normal concentration on day 7. One case (15%) showed no signs of sodium normalization between postpartum days 1 and 14; her first MOM sample was collected on day 4.
There was a difference in milk volume among the three groups on postpartum day 14, which indicated that when lactogenesis biomarkers are in the normal range at an earlier stage of the critical postpartum period, milk secretions will be higher such that lactation is more likely to be successful. Persistently high sodium concentrations suggest impaired milk production and an increased risk of failed lactogenesis.
When the study population was grouped according to milk volume for up to 14 days postpartum, we discovered a relation between changes in sodium concentration and milk volume. In the group secreting the least milk, we observed fluctuating sodium levels up to 14 days after delivery, which implied a rebound of sodium concentrations, reopening of the PCPs, and reduced milk production. The PCP closure is closely related to milk volume; as the TJs between lactocytes close, the blood–milk barrier forms, the milk sodium content plummets, and milk volume increases dramatically.
Note that PCP closure is dynamic and reversible, 17 and early postpartum and normal MOM biomarker levels do not necessarily mean that sodium concentrations will remain unchanged. Changes in the timing, rate, and sustainability of sodium concentrations are linked to (and vary dynamically with) milk volume. The mothers of premature infants who did not come to volume had a longer median time until sodium level normalization.
This study had several limitations. First, breastfeeding was prioritized over sample collection, which resulted in relatively few samples for analysis in the first 1–2 days. In addition, this study was conducted at a single tertiary hospital, due to limited human, financial, and time resources. A larger study is needed to confirm the results. Nevertheless, in view of the results, a science-based intervention for breast milk feeding care for preterm mothers after maternal separation is within reach.
In conclusion, we found the following. First, continuous use of a hospital-grade electric breast pump in the early postpartum period stimulates milk secretion in preterm mothers, and helps the MOM sodium concentration to normalize, which highlights the importance of the type of breast pump for secretory activation. Second, the change in sodium concentration by 14 days postpartum directly influenced the clinical evaluation of postpartum secretory activation, and it reflected the dynamic nature of PCP closure.
Third, mothers with higher initial sodium levels are more likely to show failed lactogenesis if the sodium concentrations remain elevated, or plateaus, over the long term. We postulate that the sodium concentration can be used clinically of insufficient and impaired lactogenesis, such as gland maldevelopment, low frequency of milk sucking, and breast edema. By predicting the likelihood of sufficient milk secretion and pumping efficiency, and determining the optimal follow-up time before symptoms develop, active intervention during the early lactogenesis period can benefit high-risk individuals (i.e., those for whom secretory activation is difficult) in terms of ensuring ample milk secretion within 14 days after delivery.
Footnotes
Acknowledgments
The authors are thankful to all their participants for their valuable contribution to this study.
Authors' Contributions
S.Y. contributed to designing the study, conducted the statistical analysis, drafted, edited, submitted the manuscript, and revised the article. Q.L. assisted in designing the study and revising the manuscript, collected and registered the clinical data. H.W. contributed to the implementation. X.X. read and critically revised the manuscript and contributed to the concept and management of the research. All the authors interpreted the data, revised the manuscript, and read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.