
Abstract
Background:
Patients from low-income, minoritized communities have limited access to outpatient breastfeeding support with International Board Certified Lactation Consultants (IBCLCs). Telelactation may increase access particularly when appointments can be self-scheduled.
Objective:
To describe a medical center-based, outpatient breastfeeding support program that includes telelactation and serves a diverse patient population.
Methods and Study Design:
A retrospective electronic chart review was performed for patients with in-person or telelactation visit types between April 2020 and December 2021. Impact of demographics (language, race/ethnicity, insurance) on scheduling patterns (self-scheduled versus traditionally scheduled), visit reasons, and impact of initial visit type and reason on subsequent follow-ups were determined. Feeding practice-to-feeding goal ratios were compared between initial and last visit to determine if breastfeeding goals were met. Descriptive statistics, linear regression, chi-square, and paired t-tests were performed.
Results:
Two thousand twenty-three patients (37.9% Spanish-speakers, 76.6% Latinx; 8.0% black/non-Latinx, 79.0% publicly insured) made 2,791 visits, of which 50.6% were for telelactation. Self-scheduling resulted in decreased no show rates (25.3% versus 42.8%, p < 0.001). Commercially insured patients had greater odds of self-scheduling versus publicly insured (adjusted odds ratio: 9.22; 95% confidence interval, CI [6.27–13.57]) with no impact of race/ethnicity or language. Reasons for visit differed slightly by initial visit type. Practice-to-feeding goal ratios increased regardless of initial visit type: telelactation visit (0.84 to 0.88 [difference 0.04; 95% CI: 0.006–0.066; p = 0.017]); and in-person visit (0.77 to 0.84 [difference 0.07; 95% CI: 0.044–0.11 p < 0.001]).
Conclusions:
Telelactation as part of a medical center-based outpatient breastfeeding support program is a promising modality for both initial and follow-up visits. Self-scheduling decreased no show rates.
Background
While the importance of breastfeeding for infant and maternal health is firmly established, national breastfeeding rates do not meet recommendations.1–3 Significant disparities exist, with lowest rates among low-income and minoritized women. Moreover, women from all socioeconomic backgrounds fall short of meeting their personal breastfeeding goals. 4 Common breastfeeding issues, such as difficulty with latch, nipple pain, and concerns regarding milk supply in the early postpartum period, contribute to early cessation of breastfeeding. 5 It has been estimated that 90% of women report developing breastfeeding issues in the first postpartum week. 6 When not addressed in a timely manner, breastfeeding success is undermined. Improving access to and availability of high-quality, timely breastfeeding support are critical to helping women meet their breastfeeding goals and increase both breastfeeding duration and exclusivity.7,8
International Board Certified Lactation Consultants (IBCLCs) are highly trained experts in breastfeeding management; however, many women do not have access to outpatient breastfeeding support with IBCLCs, particularly those with public insurance and in low-income, minoritized communities.9,10 Telelactation, providing breastfeeding support via a video visit, has shown early preliminary success. Currently, the majority of large-scale telelactation services in the United States are privately run and marketed direct-to-consumers. Several studies focused on the use of direct-to-consumer platforms in various settings, such as one small rural hospital in Pennsylvania 11 and via WIC,12–14 and other small exploratory studies focused on telelactation provided as part of clinical care.15,16 A recent review highlighted that the most effective outpatient breastfeeding support is that in which the health care system is involved. 17 No studies to date have described a medical center-based telelactation program open to a diverse patient population.
We describe an outpatient telelactation program developed and implemented at a tertiary care academic medical center in New York City, which serves a diverse patient population in terms of race/ethnicity, language preference, and insurance type. The objectives of this study were to characterize (1) usage patterns, (2) reasons for visits, (3) breastfeeding practices and goals at the time of visit, and (4) patient demographics of those who sought care in an outpatient breastfeeding support program that includes telelactation.
Methods
Study setting and sample
This study took place at an academic medical center in Northern Manhattan, with ∼6,300 annual births with a relatively even mix of Medicaid-insured and commercially insured patients. At the time of hospital discharge, parents of newborns either schedule an appointment with their private pediatrician or are provided with an appointment in our medical center's Newborn Clinic (NBC). NBC provides the first outpatient visit within 3–5 days of life for newborns with Medicaid who do not have a private pediatrician or who plan to establish their medical home in one of the medical center's outpatient primary care sites. Approximately 2,000 newborns receive care in the NBC annually.
Outpatient breastfeeding support for patients born at the medical center is available with a team of two registered dietitians who are IBCLCs (RD/IBCLC) and one pediatrician who is an IBCLC (MD/IBCLC), via both in-person and telelactation visits. In-person RD/IBCLC visits are available at the time of a newborn's NBC appointment so that any woman noted to be having breastfeeding issues, questions, or concerns could meet with the RD/IBCLC immediately after the NBC appointment. Approximately half of all NBC patients meet with the RD/IBCLC at the time of their NBC appointment. In-person visits with the MD/IBCLC are available at one of the medical center's general pediatrics faculty practices, which care for patients who are primarily commercially insured. Visits with the MD/IBCLC do not occur at the time of a scheduled newborn visit at the practice, but rather require women to make a separate visit for that appointment.
Starting in March 2020, telelactation appointments have been offered for all patients born at the medical center, or who receive pediatric primary care in one of the medical center's outpatient primary care sites or faculty practices. This program was designed as an outpatient breastfeeding support service for patients at the medical center. Thus, promotion of this program through patient education primarily occurred at the time of birth hospitalization and pediatric and postpartum obstetric visits at the medical center practices. Patient education included informing women that they could obtain a telelactation appointment via referral from their infant's primary care provider or by calling the telelactation scheduler to make an appointment.
As of June 2021, women could self-schedule a telelactation appointment via the HIPAA compliant, electronic health record (EHR) integrated, bilingual MyChart app if their infant was less than 12 months of age. At this time, patient education was adjusted to include information on self-scheduling. Telelactation visits are performed on women's personal devices via the MyChart app. After the initial visit, women are eligible to schedule subsequent follow-up appointments with the same IBCLC, either via self-scheduling, calling the telelactation scheduler, or calling the faculty practice office.
At the time of the breastfeeding support visit, the IBCLC characterized and recorded the reason(s) for the visit in her encounter note via a dropdown menu that included prepopulated reasons for the visit (e.g., breast pain, latching difficulties, general breastfeeding education) and one “other” box that enabled the IBCLC to enter a free-text reason for visit. The IBCLC also recorded the woman's self-reported feeding goals and feeding practices using a 5-item scale: exclusive formula, formula>breastfeeding, formula = breastfeeding, breastfeeding>formula, and exclusive breastfeeding. Telephonic interpreter services were available for all visit types as needed.
To address any privacy issues, telelactation visits were performed solely using the telehealth platform contained within the MyChart app, the HIPAA-compliant app that is fully integrated with the medical center's EHR and on which all video visits at the medical center are performed. At the time of the telelactation visit, women sign a consent form via MyChart to partake in the video visit. To ensure privacy, the IBCLC performed the visit in a private office or examination room behind closed doors on a hospital-issued computer or iPad. Women chose the location at their home in which they were most comfortable performing the visit.
Analysis
A retrospective electronic chart review was performed for all patients who had either an in-person or telelactation visit between April 2020 and December 2021. Patient-level data were coded in self-reported race/ethnicity (Hispanic/Latinx, black/non-Latinx, white/non-Latinx, other); insurance type (commercial versus public); and preferred language (English, Spanish, other). Visit-level data included age of infant at time of the visit, visit type (initial versus follow-up), reason(s) for visit, and feeding goals and practices. All recorded reasons for visits were captured by the 12 categories listed in Table 3. Feeding practices and goals were each assigned a numerical value ranging from 1 to 5, where 1 = exclusive formula, 2 = formula>breastfeeding, 3 = breastfeeding = formula, 4 = breastfeeding>formula, and 5 = exclusive breastfeeding.
We assessed the impact of demographics (language, race/ethnicity, and insurance type) on scheduling patterns using chi-square and multivariate analyses. We described the common reasons for visit and conducted linear regression analyses to assess the impact of initial visit type and reasons for visit on a number of subsequent follow-up visits. As an attempt to determine if the woman was meeting her breastfeeding goal, the study authors created a practice-to-goal ratio tool, calculated by dividing the feeding practice value by the feeding goal value.
This is a nonvalidated tool that was used solely for this study as an attempt to characterize how close a woman's reported feeding practices were to her reported breastfeeding goals. We proposed that a practice-to-goal ratio of 1 indicated that feeding practice and goal were identical and she was meeting her breastfeeding goal; a ratio less than 1 indicated breastfeeding less than desired; and a ratio greater than 1 indicated breastfeeding more than desired. We defined a feeding practice-to-goal ratio between 0.8 and 1.2 as “at or close to meeting breastfeeding goal.” Analyses were completed using SPSS v.28 (IBM Corporation, Armonk, NY). This study was approved by the Columbia University Institutional Review Board with a waiver of consent.
Results
During the study period, 2,023 patients made 2,791 breastfeeding support visits, which were fairly evenly split between in-person (n = 1,378, 49.4%) and telelactation (n = 1,413, 50.6%) visits. Overall, half (50.3%) of patients had at least one telelactation visit. Nearly all (93.1%) in-person visits were new patient/initial visits, whereas telelactation visits were more closely split among new patient/initial (52.4%) versus follow-up visits (47.6%). Patients used both in-person and telelactation visit types for new patient/initial and follow-up visits in various combinations (Table 1).
Usage Patterns for In-Person and Telelactation New Patient and Follow-Up Visit Types
On a visit level, while the majority of patients who made a breastfeeding support visit were publicly insured, English speakers, and Hispanic/Latinx, significant differences among demographic breakdowns were noted between those who made in-person versus telelactation visits (Table 2). When compared with in-person, fewer telelactation visits were for those who were publicly insured (59.9% versus 90.9%) and Hispanic/Latinx (61.4% and 85.4%), while more visits were for those who were English speakers (68.9 and 51.7) (p < 0.001).
Visit-Level Demographic Characteristics of Patients Who Made Breastfeeding Support Visits
The median age of the baby at initial visit varied significantly between in-person and telelactation (age at in-person visit, 5-day interquartile ratio (IQR 4, 6) versus at telelactation visit, 13 days (IQR: 8, 25) (p < 0.001).
Self-scheduling telelactation
Since self-scheduling was enabled, 23.9% (n = 338) of all telelactation visits were self-scheduled, with the majority (77.9%, n = 263) for initial visits. On a regression model, those who were commercially insured had nine times greater odds of self-scheduling versus those publicly insured (adjusted odds ratio: 9.22; 95% confidence interval, CI [6.27–13.57]); there was no impact of race/ethnicity and language. Self-scheduling resulted in a significant decrease in no show rates (25.3%) compared with traditionally scheduled telelactation appointments (42.8%), (p < 0.001).
Reasons for breastfeeding support visits
The most commonly cited reason for initial in-person and initial telelactation visits was general breastfeeding support (36.3% and 56.9%, respectively) (Table 3). The next three most common reasons differed slightly between visit types, with latching problems and milk supply concerns common for both in-person and telelactation. Pumping and breast milk storage questions/concerns were common for telelactation and nipple pain for in-person visits.
Reasons for a Breastfeeding Support Visit
More than one reason could be selected per visit.
Denotes the top 4 most commonly cited reasons for a breastfeeding support visit.
While the majority of women made only one visit to the program, 25.0% made more than one. On a stepwise linear regression model, reasons for the initial visit that were more likely to result in an increased number of follow-ups included infant weight concerns (Beta: 0.59; 95% CI [0.30–0.89]), mastitis (Beta: 0.80; 95% CI [0.27–1.33]), nipple pain (Beta: 0.13; 95% CI [0.043–0.22], and latching problems (Beta: 0.09; 95% CI [0.012–0.18]). Telelactation as the initial visit type was also associated with a small increase in the number of follow-up visits (Beta: 0.12; 95% CI [0.038–0.19]).
Feeding practices and feeding goals
A range of feeding practices and feeding goals were noted among women who made telelactation and in-person visits, as demonstrated in pictorial form in Figure 1. Slightly more than half of women were at or close to reaching their breastfeeding goals at initial visits (66.1% for telelactation and 56.7% for in-person visits) (Fig. 2). There were a very small number of women with ratios >1, indicating that they were breastfeeding more than desired at the time of the initial telelactation and in-person visits: 1.1% versus 1.9%, respectively.
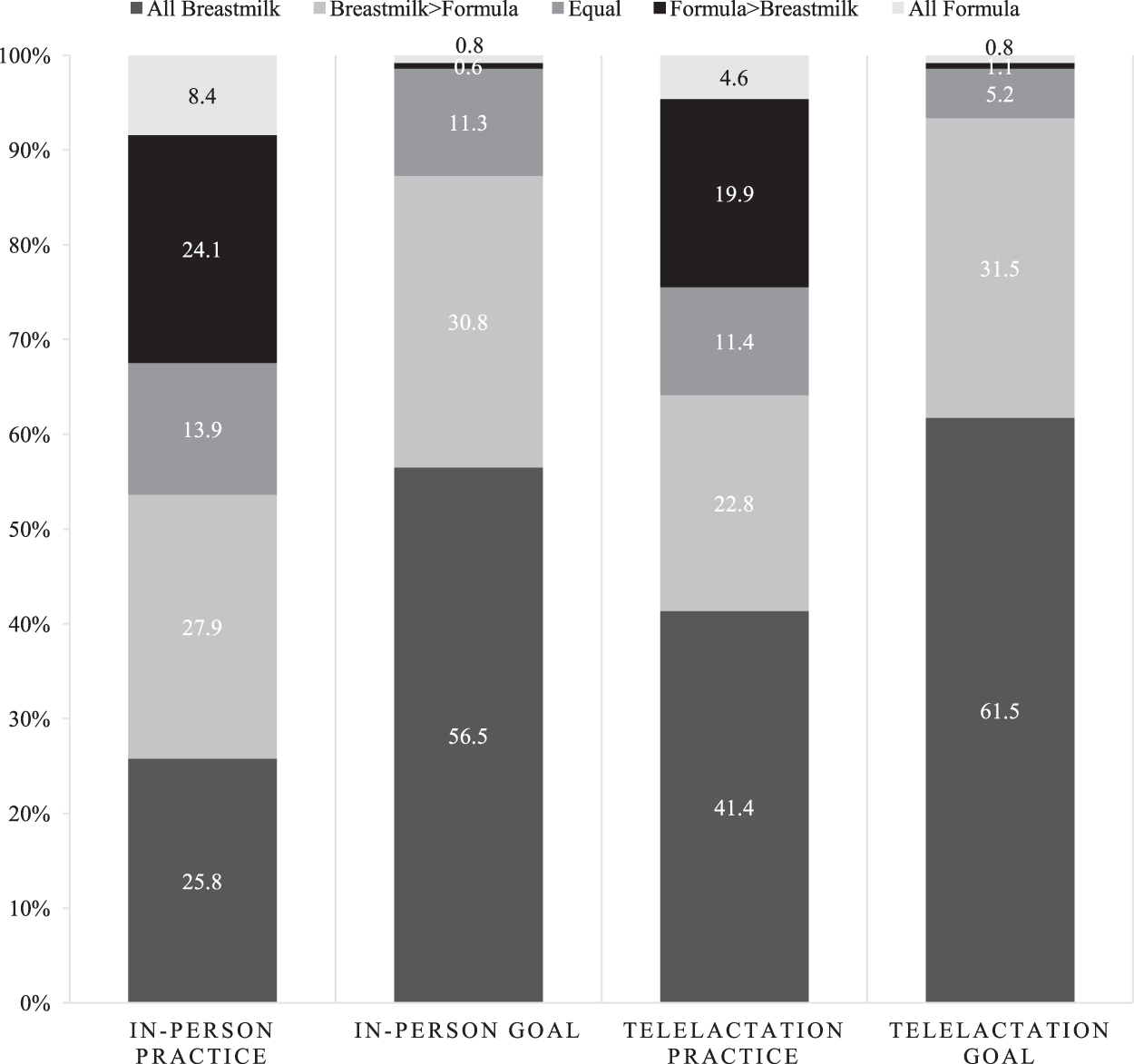
Pictorial representation of infant feeding practices and goals by visit type.

Frequencies of infant feeding practice-to-goal ratio by initial visit type. Size of circle represents percent of total breastfeeding dyads (n = 2,023) with each corresponding feeding practice-to-goal ratio. Ratio = 1 indicated woman reaching her breastfeeding goal.
Among the 505 patients who had follow-up visits, a small increase in practice-to-goal ratio between the initial and last visit was noted regardless of initial visit type. Ratios increased from a mean of 0.84 to 0.88 among women who had an initial telelactation visit versus 0.77 to 0.84 among those with an initial in-person visit.
Discussion
Our study is the first of its kind to describe a large-scale medical center-based outpatient breastfeeding support program that includes self-scheduling telelactation and is available to all patients after delivery. We describe the important role that telelactation played for both new patient and follow-up visits, particularly for a population that historically has not had ready access to ongoing outpatient breastfeeding support with an IBCLC. We demonstrated high utilization of telelactation among a diverse patient population including non-English speakers, publicly insured, and nonwhite patients. This is in contrast to multiple recent studies that have demonstrated disparities in telemedicine utilization among low-income, publicly insured, non-English speakers,18–21 including one at our own institution. 20 Possible explanations for our outcomes include extensive patient education about telelactation at the time of birth hospitalization and discharge calls by the telelactation scheduler to all postpartum women to inform them about the program. Targeted outreach efforts for telehealth initiatives have been described by others as well with similarly positive results.18,22
While our findings support the use of telelactation as a way to reduce disparities in outpatient breastfeeding support, we demonstrated a disparity for non-English speakers, and for self-scheduling in particular, among those who are publicly insured. Given the positive effects of self-scheduling to reduce staffing to schedule appointments, the ability to schedule and cancel appointments in real-time as breastfeeding problems arise and shift, and the reduction in no-show rates in our study, this remains an area that requires further investigation and focus.
Consistent with other studies in the literature,23–26 the most common reasons that women sought breastfeeding support included latching problems, pain, milk supply and pumping/breast milk storage questions/concerns, and general breastfeeding support. While overall the range of issues that women presented with for both telelactation and in-person visits was similar, one notable difference in the top 4 presenting issues for in-person versus telelactation visits was nipple pain. This was a more common presenting issue for initial in-person visit versus initial telelactation. Since nipple pain often presents in the early postpartum period,6,27 the earlier timing of the initial in-person visit versus telelactation visit, demonstrated by babies' younger average ages, may be one explanation for this difference.
An important role for telelactation noted in our study is its ability to provide ongoing follow-up for issues that were addressed in-person initially. Initial visits with presenting issues including infant weight concerns, mastitis, nipple pain, and latching problems resulted in more follow-up visits. This adds to the literature by defining which issues may be considered “more intensive,” requiring ongoing resources to manage. Interestingly, telelactation visits in and of themselves were associated with more follow-up visits. Several possible reasons may include the ease that follow-up could be accessed via telelactation, without having to leave home, or that telelactation as a modality of support required more visits to more fully address a given breastfeeding issue.
Future research is needed to better understand this finding. Finally, concern has been noted in the literature that not all breastfeeding problems could be adequately addressed by telelactation. 28 Indeed, we found that there were a small percentage of patients who sought in-person follow-up after their initial telelactation visit. Thus, our study supports the need to be able to offer in-person visits as follow-up when necessary as part of a comprehensive breastfeeding support program.
Further research is needed on how best to measure the outcomes of a breastfeeding support program, and on the use and validation of the feeding practice-to-goal tool created for our study. The impact of a breastfeeding support program is often defined by its ability to increase breastfeeding, either by increasing the duration or exclusivity of breastfeeding. This, however, does not take into account the range of feeding goals among women who seek breastfeeding support, as demonstrated in our study, which might not be to exclusively breastfeed. 29 Notably, there was a small subset of women in our study who made a visit because they were breastfeeding more than desired. As opposed to solely focusing on an outcome of increasing breastfeeding duration or exclusivity, measuring a woman's success at reaching her personal breastfeeding goals is an important outcome measure to consider.
To this end, we created a novel feeding practice-to-goal ratio as a measure of women's success at reaching their breastfeeding goals. This tool may help to better capture outcomes of a breastfeeding support program. For example, in our study, we found an association between follow-up visits and women meeting their breastfeeding goals. While we do not know from our data whether follow-up visits more thoroughly addressed the presenting issue or that women who made more follow-up visits were more committed to reaching their breastfeeding goals, the ability to provide ongoing support via follow-up visits is certainly an important aspect of a large-scale breastfeeding support program as evidenced by the use of this novel tool.
Limitations
It is possible that some patients with ongoing breastfeeding issues sought support outside our medical center, and thus, we did not capture all the breastfeeding issues. Given the older age at time of initial telelactation visit, we may have missed the pressing issues known to occur in the first week of life, such as nipple pain, that were noted to be common reasons for in-person visits occurring at the time of the NBC appointment. Thus, the telelactation visit group may have been a self-selected group of women who were more committed to breastfeeding, which their practices may have reflected. Our program was set up for the telelactation appointment to be scheduled through the newborn's MyChart account, necessitating an extra step for granting proxy access to the mother, which often did not happen until after the first outpatient pediatric appointment.
This could have contributed to the older age at time of initial new patient telelactation visit. In the Spring of 2022, automatic proxy access was turned on in our EHR so that women are automatically granted access to their newborn's account and thus able to self-schedule telelactation visits from the moment of hospital discharge. Future research will look to see if automatic proxy access resulted in a shift to earlier telelactation visits and a shift in reasons for visits.
Conclusions
Our study demonstrates that telelactation as part of an outpatient breastfeeding support program is a promising modality for reaching women, providing ongoing support, and addressing common breastfeeding issues and concerns, particularly among those who are publicly insured. Self-scheduling telelactation has many benefits, including reducing no show rates, and more work needs to be done to understand why this option had higher utilization among commercially insured patients. Future research should also include measures of patient satisfaction and how that may differ between in-person versus telelactation visits. Language disparities remain for telelactation, and further research is needed to determine how to optimally reach non-English speakers.
Footnotes
Acknowledgments
The authors wish to thank Sharon Haier, MS, RD, CDN, CDE, IBCLC, Sadye Silva, MPH, RD, CDN, IBCLC, and Jennifer Sanchez for their hard work and dedication at supporting our patients' breastfeeding efforts. The authors also wish to thank NewYork-Presbyterian Hospital and its Ambulatory Care Network for providing support for the telelactation program.
Authors' Contributions
M.E.G. participated in the study's conception, design, and implementation, data collection and analysis, and article writing and review. A.P.S. participated in the study's design and implementation, and analysis. D.K.-F. participated in the study's conception, design, and implementation, data collection and analysis, and article review. J.Z. participated in the study's conception, design, and implementation, and article review. P.T. participated in the study's conception, design, and implementation, and data collection. M.S.S. participated in the study's conception, design, and implementation, data collection and analysis, and article writing and review.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded through a grant from the NewYork-Presbyterian Hospital.