
Abstract
Introduction:
Breast engorgement (BE) is a problem that affects many women, especially in the first days of breastfeeding, producing inflammatory symptoms. Nonpharmacological therapies are inexpensive, safe, and can produce symptom relief.
Objective:
This study aims to analyze the safety of therapeutic ultrasound regarding possible risks of overheating and the effects of its use alone and associated with lymphatic drainage (LD) in women.
Material and Methods:
Effectiveness is measured through thermography, visual analog scale, and six-point scale of BE. This is a nonrandomized clinical trial with a sample of 34 in the ultrasound group (G1), 28 in the ultrasound and LD group (G2), and 37 in the control group (G3).
Results:
The mean reduction for engorgement was 1.3 ± 0.8 to G1, 1.4 ± 1.0 to G2, and 1.2 ± 0.9 to G3 according to the six-point scale. The mean reduction for pain level was 3.6 ± 2.1 to G1, 4.0 ± 3.1 to G2, and 4.0 ± 2.2 to G3 according to the visual analogue scale.
Conclusion:
It was observed that all therapies were effective in reducing the level of engorgement, according to the six-point scale. However, combined ultrasound and LD therapy has been shown to be more effective in reducing the level of pain. Brazilian Registry of Clinical Trials (RBR-6btb6zz).
Introduction
Exclusive breastfeeding for the first 6 months of life is associated with significant benefits for the mother–baby dyad. 1 It is estimated that breastfeeding could prevent 13% of deaths in children under 5 years of age worldwide from preventable causes.2,3 Despite its importance, the breastfeeding process is often challenging given that some disorders can complicate its establishment and continuation. Major breastfeeding-related challenges include low milk production, nipple trauma, breast pain, mastitis, and breast engorgement (BE).1,4,5
BE is defined as the swelling and distension of the breasts, usually in the early days of lactation, caused by vascular dilation as well as the arrival of early milk and processes such as increased vascularization, edema, and obstructed lymphatic system drainage.4,6 Traditional treatment involves maintaining consistent breastfeeding habits to balance consumption and production. Depending on the patient's clinical condition, other procedures such as massage and medication are indicated.3,5
Lymphatic drainage (LD) is a gentle manual technique applied to the surface of the skin and the anatomical lymphatic pathways of the body. Typically, it commences proximally and centrally before progressing distally in segments, with the massage being performed in the direction of the lymphatic flow.7,8 The physiological effects of LD include improved blood circulation and LD, resulting in reduced tissue swelling. 9 Drug treatment, however, focuses only on the symptoms of engorgement and not the cause. In addition, drugs are not always efficient, can be costly, and may have side effects. The use of antibiotics for inflammatory mastitis disrupts the breast microbiome and increases the risk of progression to bacterial mastitis. Furthermore, the nonselective use of antibiotics promotes the development of bacterial resistance. 4
There are alternative treatments, such as cryotherapy, compression, and therapeutic ultrasound (TUS). However, these have varied protocols that are controversial and often lack scientific evidence. 4 TUS is a nonpharmacological method widely used by physical therapists in the treatment of various disfunctions.4,10 Its interaction with biological tissues, such as reflection, refraction, absorption, cavitation, scattering, and wave attenuation, produces effects that can be classified as thermal or nonthermal. The ultrasonic frequency in commercial devices is usually 3 MHz, with the ability to reach 1–2 cm deep, and 1 MHz, which can reach 3–5 cm deep. The intensity can vary between 0.5 and 2.0 W/cm2 for thermal therapy and between 0.1 and 0.3 W/cm2 for nonthermic therapy. 11
The use of TUS has long been advocated in the management of BE; in some cases, its efficacy has been reported in its treatment. However, some of these studies had limitations in terms of research design, documentation, or sample size. Recommendations were made to conduct randomized trials with dosage modifications. 12
Thus, this study aimed to verify the effects of TUS alone versus its association with breast LD in women with BE and analyze the safety of the possible risks of ultrasound overheating through thermography.
Materials and Methods
This nonrandomized clinical study was conducted at the Bárbara Heliodora Maternity and Luís Augusto Hidalgo de Lima Basic Health Unit in Rio Branco, Acre, Brazil. Data were collected between April 2021 and March 2022. This study was approved by the Research Ethics Committee of Fundação Hospitalar do Acre (3.054.081 and 85405318.0.3001.5009).
Sample allocation in each group was performed without blinding the participants and therapist. The study included 99 lactating women with unilateral or bilateral BE, primiparous or multiparous women after vaginal or cesarean delivery, mothers of full-term or premature babies, and women irrespective of hospitalization in the institutions mentioned above. After meeting the inclusion criteria, participants signed a free and informed consent form authorizing their participation in the research. Women with mastitis, breast abscesses, neoplastic processes, impaired tissue integrity in the breast body, or those who did not wait for reassessment were excluded from the study.
Figure 1 shows the high study dropout rate. The women were invited to participate in the research when entering in a public health service for other purposes (for a medical and/or exam appointment).
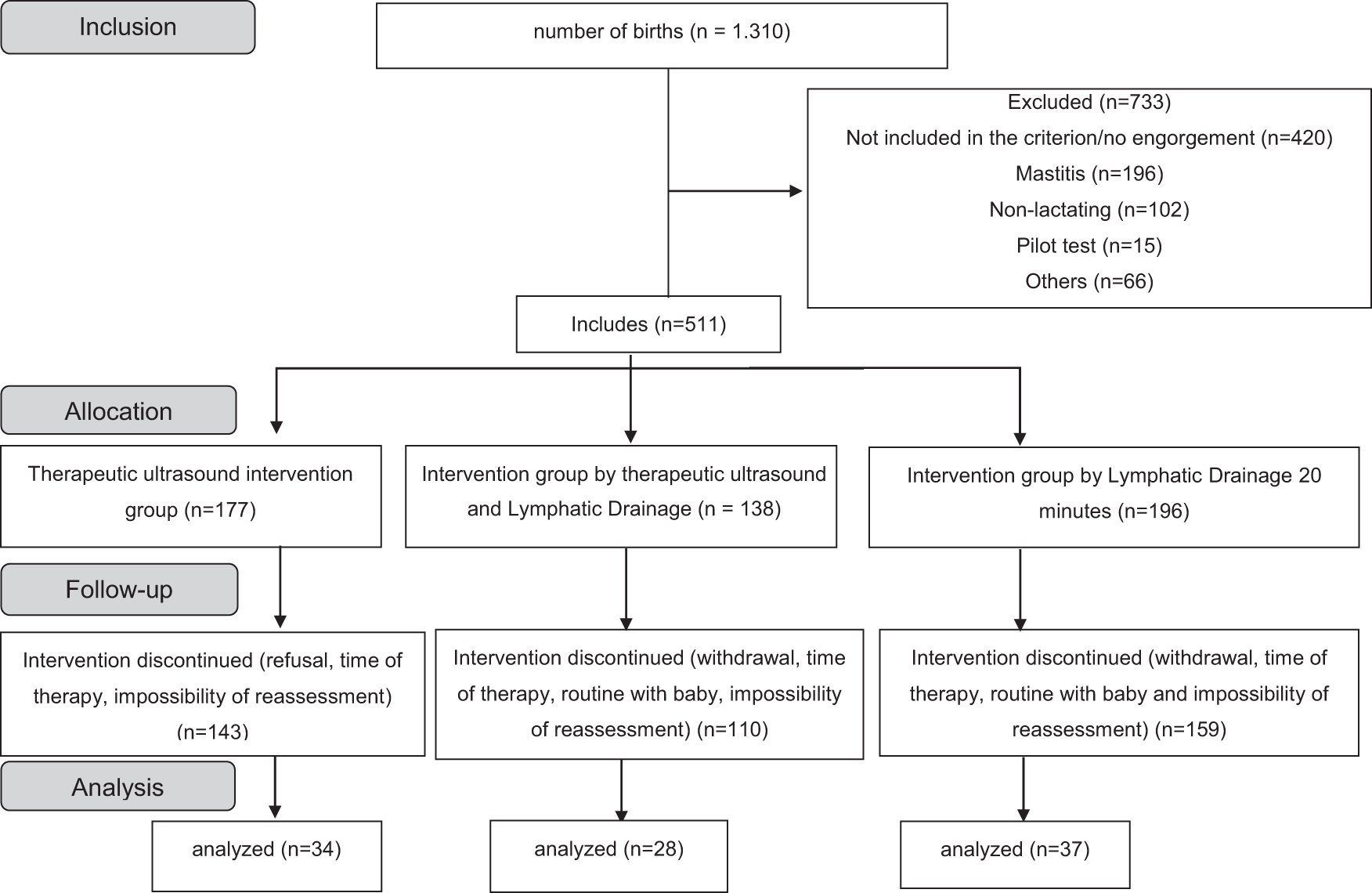
CONSORT flow diagram describing for patients of clinical trials.
Sample allocation was performed to the treatment and control groups. Within the intervention group, the participants were divided into the following subgroups (Table 1):
Intervention Groups According to the Application of Biophysical Resources and Control Group
N, number of women; n, breast number.
LD, lymphatic drainage; TUS, therapeutic ultrasound.
G1: Sonopulse III therapeutic ultrasound equipment (IBRAMED; Amparo, SP, Brazil) with a nominal effective radiation area of 7 cm2 configured with continuous mode, a frequency of 1 MHz, and effective intensity of 2 W/cm2 for 20 minutes in each breast with a moving head using water-based gel for impedance matching.
G2: The same techniques were followed for 10 minutes each.
G3: Treatment was delivered for 20 minutes following these steps: (1) verify gentle touch/traction of skin, lift skin to allow flow of LD/vascular decongestion. (2) Ten small circles at junction of Internal Jugular and Subclavian vein. (3) Ten small circles in axilla. 4
To assess BE, the participants completed a questionnaire of their personal data, lifestyle habits, and gynecological, obstetric, and clinical history, as well as a pain analysis using the visual analogue scale (VAS) and an infrared thermography (Fig. 2). Before the thermographic evaluation, the volunteers underwent a 10-minute acclimatization period at room temperature (around 24°C) with the area to be treated uncovered. Vital signs such as blood pressure and body temperature were also assessed. Images were obtained using an infrared camera with MSX® and Wi-Fi model E6 (Flir Systems, Inc., Wilconville, OR, USA), with the camera lens positioned 40 cm from the breast's surface. Visual inspection and breast palpation were used to evaluate BE level by the six-point scale of Hill and Humenick 13 which is (1) Soft, no changes, (2) Slight change, (3) Firm, nontender, (4) Firm, beginning tenderness, (5) Firm, tender, (6) Very firm, very tender.
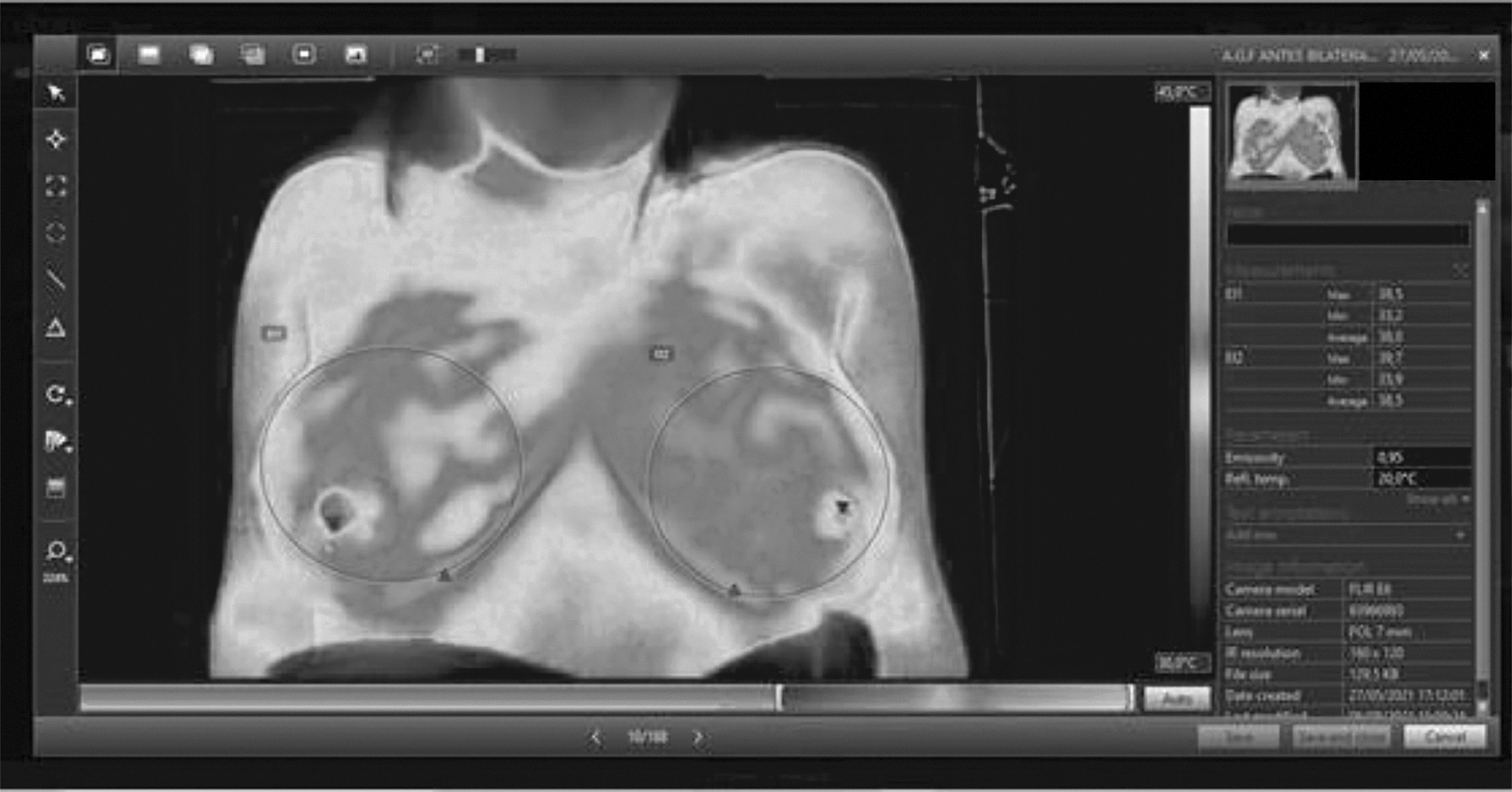
Representation of thermographic image analyzed in Flir tools program.
All data were previously treated using Python 3.0 tool and the respective libraries, pandas, numpy, scipy, and sklearn.impute (KNNImputer). The purpose of this pretreatment was to clean and prepare the data for statistical testing using the k-Nearest Neighbors (KNN) technique to impute missing values when necessary. KNN was chosen because it is a popular and efficient technique for imputing missing data, which are based on the distances of the “K” near neighbors, using the integral dataset as parameters for the calculations. Here “K” was set to 3.14,15 The maximum number of missing data per attribute was 14, corresponding to 14% of all collected data. Initially, for inferential treatment, the Shapiro–Wilk normality test was performed. One-way analysis of variance (ANOVA) with Tukey's post hoc test was used to examine parametric data. For nonparametric data, the Kruskal–Wallis test with Dunn's posterior test was used. All tests were performed with a significance of 5% using PrismStat 5.0.
Results
Sample description
The study included 99 women with a mean age of 26.4 ± 6.8 years. The mean pregnancy weight was 69.8 ± 13.4 kg, height was 1.58 ± 0.06 m, body mass index was 27.5 ± 5.1, and body temperature was 36.0°C ± 0.7°C.
The participants' levels of education were as follows: incomplete primary education, 14%; complete primary education, 5%; incomplete secondary education, 15%; complete secondary education, 43%; and higher education, 22%. No significant differences were found in these variables in relation to treatment (Table 2). The obstetric profiles of the evaluated patients showed that 56% had delivered vaginally versus 44% by cesarean section. The mean gestational age was 38.4 ± 1.8 weeks. Regarding parity, 60% were multiparous, and 40% were primiparous. The mean timing of the occurrence of BE in the population was 5.5 ± 2.8 days after delivery.
Obstetric and Physical Characterization of Lactating Women
ANOVA: different for p < 0.05.
ANOVA, analysis of variance; BMI, body mass index.
Temperature
The temperature measured by a thermographic camera was used to obtain the average found before, immediately after, and 30 minutes after each therapy was applied between the three groups. The temperature variable is normally distributed. It was observed that the average temperature of the breasts of group submitted only to TUS was 37.1°C ± 1.1°C before application, 35.9°C ± 1.7°C immediately after, and 37.6°C ± 0.8°C 30 minutes later. The mean of group referring to breast LD and TUS was 37.4°C ± 1.9°C before, 36.0°C ± 1.7°C immediately after, and 37.1°C ± 1.3°C 30 minutes later. The control group, with application only of the conventional technique of breast LD, presented the following values before, shortly after, and 30 minutes later: 36.7°C ± 1.3°C, 36.9°C ± 1.7°C, and 36.8°C ± 1.5°C, respectively (Table 3).
Results of Visual Analogue Scale, Six Points Scale, and Temperature Before and After Treatments
VAS, visual analogue scale.
The average temperatures collected immediately after the therapies applied in groups G1 and G2 showed a reduction owing to the use of the conductive gel during ultrasound application. Owing to this bias, this variable was not included in the graph in Figure 3. There was no significant difference (p > 0.05) between the temperatures before and 30 minutes after the treatment (Fig. 3A).

Breast engorgement
The degree of BE was assessed using a six-point scale before and 30 minutes after therapy. Group 1, received only TUS, showed a mean reduction of 1.3 ± 0.8 (dimensionless). Participants who received combined TUS and breast LD therapy had a mean reduction of 1.4 ± 1.0, while the group that received only breast LD had a mean reduction of 1.2 ± 0.9 (Table 3).
The Kolmogorov–Smirnov test showed that the sample did not follow a normal intergroup distribution. The difference between the medians of the six-point values before and 30 minutes after treatment was significant in all treatments (p < 0.05) according to the Wilcoxon statistical test (Table 3 and Fig. 3B). Thus, we can infer that TUS is as efficient as conventional breast LD to reduce engorgement levels and improve milk flow.
Pain intensity
Pain caused by BE was measured using the VAS before and 30 minutes after each therapy. TUS only (Group 1) reduced the pain level by a mean 3.6 ± 2.1 points. Group 2, which received TUS and breast LD, reported greater pain relief, with a mean decrease of 4.0 ± 3.1 points. Participants allocated to group 3, who received only breast LD, had a mean decrease of 4.0 ± 2.2.
The Kolmogorov–Smirnov test showed that the sample did not follow a normal intergroup distribution. The difference between the medians of the VAS values before and 30 minutes after treatment was significant for all treatments (p < 0.05) on the Wilcoxon test (Table 3). Thus, it is possible to see that the use of TUS and LD efficiently reduced breast pain, but their combined use has been shown to promote greater symptom relief and well-being. The VAS scores differed between the pre- and posttests for all groups (p < 0.0001) (Fig. 3C).
Discussion
Sample description
Corroborating with previous studies that state the occurrence of BE occurs between the third and fifth day after delivery, this study obtained an average timing for the occurrence of BE in the population among puerperal women of 5.5 ± 2.8 days after delivery. 16 It is important to highlight that the high dropout rate of women from treatment is due to the waiting time of 50 minutes for the application of the protocol, and most women could not wait that long.
Temperature
An increased temperature in the puerperal breast is a hallmark of BE. Thermographic analysis is a quantitative method used to evaluate BE.17,18 In this research, in groups 1 and 2 during the three consecutive periods, we perceived that the TUS did not cause overheating in the breast tissue. This information is significant considering that TUS was not historically part of the clinical practice of professionals treating BE due to a lack of evidence and under the justification that thermal effects could lead to the production of hot spots and tissue damage or generate neoplastic processes.
Maggi et al. evaluated the thermal effects of TUS on breast tissue before, immediately after, and 24 hours after treatment for engorgement and concluded that there was no significant increase in temperature. 19 In addition, according to the participants' perceptions reported during the ultrasound application, it did not produce discomfort and was well accepted by groups 1 and 2. However, knowledge about the anatomy of the region is necessary considering that the anastomotic circle, called Haller's vascular network, dilates in the pregnancy-puerperal phase, and may saturate the image. 17
Breast engorgement
A randomized controlled trial by Priyanka et al. 20 applied TUS at a frequency of 1 MHz in the continuous emission mode in a group composed of 40 women in the intervention group and 40 women in the control group. The researchers confirmed the hypothesis of a reduction in the six-point scale score after the application of TUS associated with the conventional therapy of hot compression and massage. 20 However, the authors performed follow-up and application of TUS for 4 consecutive days, while this research tested the application only in a single session. Even with a single session of ultrasound therapy, there was a significant reduction in the degree of engorgement. More pronounced improvement was observed when ultrasound was associated with breast LD.
Similarly, Lavigne and Gleberzon tested the application of TUS over a period of 1–7 days. 21 They used parameters of 1 MHz in the continuous emission modality and an intensity of 2 W/cm2 in a group composed of 25 women with blocked ducts. For this population, the authors reported the average number of days that elapsed before the patient experienced improvement was 6.8, although 2 patients experienced resolution of their symptoms the same day and 9 experienced symptom resolution within 1 day. The authors indicate that it may be worthwhile to conduct a clinical trial to better ascertain the benefits.
As for the dose used in TUS in this study, Mitchell et al. also suggested the parameters of 1 MHz and 2 W/cm2 in the protocol they proposed as well as claiming that TUS is a noninvasive and satisfactory alternative that helps reduce edema and provide general relief of breast symptoms. 4 Thus, although all treatments using biophysical agents used in this research are beneficial in terms of engorgement, the patients' perception reported to the therapists during the ultrasound application proved more acceptable as it did not produce discomfort in the engorged region. Dos Santos et al. explained that acoustic energy is better absorbed by tissues with a high density and a large percentage of protein. 22 Therefore, considering that human milk contains high concentrations of protein, the use of ultrasound in the treatment of BE is justified.
Pain intensity
The thermal effects in the continuous modality are due to the vibration of cellular particles, promoting pain relief, increasing cellular permeability, and local blood flow. 23 Such results are corroborated by some studies, including the pioneering work of McLachlan et al. who, in their double-blind randomized study, applied TUS to engorged breasts with continuous emission mode and the intensity adjusted to provide comfortable heat (range, 2.4–2.6 W/cm2). 24 They observed that the group that received the resources reported feeling greater pain relief. According to the authors, this can be explained by the fact that ultrasonic waves produce heat in biological tissues and a consequent sensation of relaxation.
Anderson evaluated the relationship between various manual massage techniques and pain relief and concluded that all were equally effective at immediate pain reduction. 25 However, the authors raised limitations regarding the difficulty of systematizing a specific procedure and quantitatively analyzing the results, which reduce the ability to replicate them. This makes it necessary for future research to standardize objective assessment techniques and tools for breastfeeding disorders as well as gather a more homogeneous and robust sample.
Priyanka et al. also performed ultrasound application with breast massage using parameters similar to this research; however, the therapies were reproduced on 4 consecutive days. 20 According to the authors, pain intensity decreased. In contrast, Mangesi and Dowswell did not obtain significant results regarding pain degree and speed of resolution, but they affirmed that nonpharmacological strategies should continue to be researched considering their low cost and lack of side effects compared to drugs. 26
Therefore, the application of TUS did not generate injuries due to overheating in the breast region. In summary, our research demonstrated that all therapies effectively reduced the degree of engorgement according to the six-point scale. Combined therapy of TUS and LD was more effective in reducing pain. The use of these nonpharmacological methods can help in the treatment of engorgement. It is noteworthy that the patients' perception of therapies involving ultrasound was more pleasant and accepted than breast LD. However, considering the limitations of this study, further research is needed, including a randomized sample and more objective assessment techniques for pain and the degree of engorgement, such as algometry and ultrasound elastography.
Conclusions
Ultrasound equipment has already been approved for human treatment; nevertheless, in this research, temperature was monitored through thermography to exclude the possibility of ultrasound overheating. According to these data, the ultrasound therapeutic doses used did not promote tissue overheating. It is also important to note that ultrasound gel reduces the temperature of the tissue after application. TUS alone and in combination with LD in women with engorgement helped reduce local tissue stiffness, indicating a reduced degree of engorgement. A higher pain reduction effect was observed when TUS was combined with LD.
Footnotes
Authors' Contributions
S.O.M.: Conceptualization, data curation, formal analysis, investigation, and writing; L.C.d.C.B., T.M.d.A.C., A.P.S.d.S., R.M.d.A., G.L.C.F., and S.d.C.M.: Data curation and investigation. L.L.D.M.: Formal analysis and investigation. P.R.d.A.: Investigation and supervision. W.C.d.A.P.: Project administration. L.E.M.: Project administration, supervision, and visualization.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors acknowledge infrastructure support from the Bárbara Heliodora maternity and Luís Augusto Hidalgo de Lima Basic Health Unit. CNPq Grant No.: 311.650/2017-1 (National Council for Scientific and Technological Development, Brazil). Coordination of Superior Level Staff Improvement—CAPES, Grant 23038.015736/2019-70. This work was supported by Research Support Foundation of the State of Acre (Fapac) and Federal University of Acre UFAC.