
Abstract
Background:
Many female people with multiple sclerosis (pwMS) are in childbearing age; however, only few data exist about the situation of breastfeeding in pwMS.
Objective:
Our study analyzed breastfeeding rate and duration, reasons for weaning, and the impact of disease severity on successful breastfeeding in pwMS.
Methods:
The study included pwMS giving birth within 3 years before study participation. Data were collected by structured questionnaire.
Results:
Compared to published data, we found a significant difference (p = 0.0007) between the nursing rate in the general population (96.6%) and females with MS (85.9%). However, a higher rate of exclusive breastfeeding could be observed in our study population for 5–6 months in 40.6% of pwMS versus 9% for 6 months in the general population. In contrast, total breastfeeding duration in our study population was shorter (18.8% for 11–12 months) than in the general population (41.1% for 12 months). Reasons for weaning were predominantly (68.7%) related to breastfeeding barriers based on MS. No significant impact of prepartum or postpartum education on the breastfeeding rate could be observed. Prepartum relapse rate and prepartum disease-modifying drugs had no effect on breastfeeding success.
Conclusion:
Our survey provides an insight into the situation of breastfeeding in pwMS in Germany.
Introduction
Many female people with multiple sclerosis (pwMS) are in childbearing age, so family planning, delivery, and breastfeeding are important issues for them and for patient counseling. The positive effect of breastfeeding on the individual MS course has been shown in several studies.1–3 According to the World Health Organization recommendation, breastfeeding should be intensively promoted due to its various health benefits. 4
Despite published studies focusing on the effect of breastfeeding on disease activity in pwMS, so far, the effect of counseling on breastfeeding, nursing rates, barriers against breastfeeding, and reasons for weaning in pwMS has not been addressed in specifically designed studies. Data on nursing rates and exclusive breastfeeding may only be derived by studies with different focus, for example, by Langer-Gould et al. 1 The aim of this study was to investigate breastfeeding rate, duration of breastfeeding, reasons for weaning, and the impact of disease severity on successful breastfeeding in female pwMS.
Materials and Methods
Females with MS who gave birth within 3 years before study participation were included. For our study, a 29-item structured questionnaire was developed (Supplementary Table S1). The questionnaire was specifically designed to explore the individual breastfeeding history, MS history, and the socioeconomic status. The study was conducted at three university hospitals in Germany, the University of Augsburg, the University of Erlangen-Nuremberg, and the University of Bochum. Females with MS having visits during the recruitment period were offered to participate. Furthermore, the study was announced at the homepage of the German MS society, the European Institute for Breastfeeding and Lactation, and communicated to practicing neurologists specialized on MS. Data were collected between February 2020 and November 2021.
All participants gave written informed consent before participating in the study. The Ethics Committee of the University of Erlangen-Nuremberg provided approval (approval number 454_19 B). Descriptive analysis and Fisher's exact test were used for statistical computation (IBM® SPSS® Statistics software).
Results
In our study, 62 participants giving birth to 64 children were included. Most patients had relapsing remitting MS (98.2%) and were in the age range between 26 and 35 years (77%). The majority (75.9%) had no or one relapse within 2 years before birth.
Table 1 gives a summary of the participants' characteristics.
Summary of Participants' Characteristics
Participants in our study reported a significantly lower (p = 0.0007) nursing rate than described for the general population (85.9% versus 96.6%; Hockamp et al 5 ). In contrast, a substantially higher rate of exclusive breastfeeding could be observed in our study population with exclusive breastfeeding for 5–6 months in 40.6% of pwMS versus 9% for 6 months in the general population. 5 However, total breastfeeding duration was shorter in our study population (18.8% for 11–12 months) than in the general population (41.1% for 12 months 5 ). In our study population, the rate for exclusive breastfeeding was 78.1% for 0–2 months.
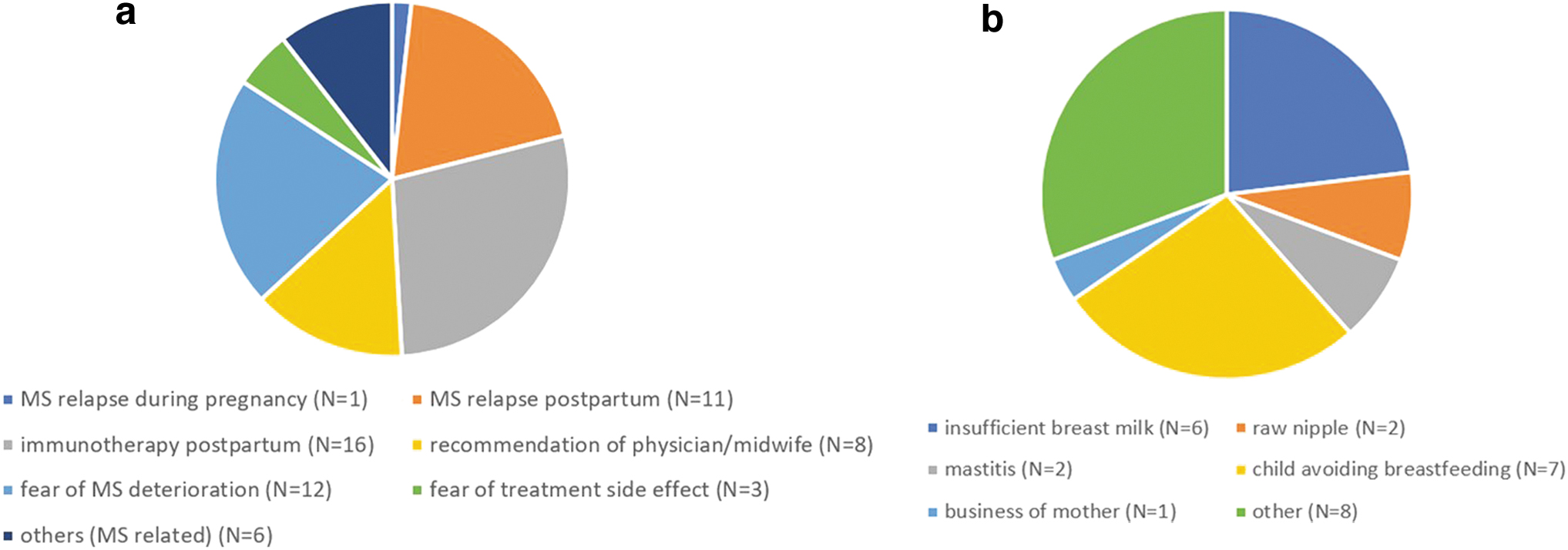
The main reasons for weaning were MS related (68.7%) (n = 45 participants answering this question) most frequently in descending order, starting postpartum immunotherapy, the patient's fear of MS deterioration, and/or a relapse postpartum.
MS- and non-MS-related reasons for weaning are displayed in Figure 1a and b.
Prepartum relapse rate and prepartum disease-modifying drugs (DMDs) had no effect on breastfeeding success, defined as mother's satisfaction with her breastfeeding outcome, total breastfeeding duration and exclusive breastfeeding duration (data not shown).
Furthermore, no significant association was demonstrated between prepartum or postpartum breastfeeding counseling and breastfeeding rate, duration of exclusive breastfeeding, or total breastfeeding time. Only 37.7% of breastfeeding mothers received any counseling about breastfeeding in MS. In contrast, 43.3% of all participants requested more information about it. Participants received prepartum counseling on breastfeeding mainly from neurologists (63.3%). Gynecologists (6.7%), midwives (6.7%), and lactation consultants (3.3%) provided advice in few cases only. Data regarding breastfeeding counseling are displayed in Table 2 and in Supplementary Table S2a and b.
Counseling About Breastfeeding in Multiple Sclerosis While Pregnant
Discussion
Although data on the effects of breastfeeding on the MS disease course have been published, to the best of our knowledge, the situation of breastfeeding in pwMS has not yet been addressed in specifically designed studies. Particularly, data on reasons for weaning in pwMS and the effect of counseling on breastfeeding rates in MS are lacking.
Our survey provides an insight into the situation of breastfeeding in pwMS in Germany, demonstrating a significant lower nursing rate (85.9%) compared to the general population in Germany (96.6%; Hockamp et al 5 ). Comparing our results with nursing rates in different countries is difficult because of varying national breastfeeding rates. 6 An almost equal breastfeeding rate of 87.3% among pwMS in the United States (466 pregnancies among 375 pwMS studied) has been reported, 1 of note, however, similar to the breastfeeding rate of 83.2% in the general population in the United States in 2019. 7
We found that 40.6% of children were exclusively breastfed over 5–6 months, and this is considerably higher compared to the general population (9% over 6 months 5 )—although a direct comparison is hampered due to the different study designs. Participants in our study had also longer exclusive breastfeeding periods, that is, 78.1% exclusive breastfeeding for 0–2 months, compared to other studies in pwMS with 59.7% exclusive breastfeeding for 2 months in a German cohort (201 pregnant women included), 2 and 34.4% exclusive breastfeeding for 2 months in an Italian cohort (423 pregnancies in 415 women). 8 We cannot exclude that our results are biased by the fact that pwMS having a positive attitude toward breastfeeding may have participated more frequently and may thus be overrepresented.
Usually, breastfeeding rates in the general population increase with higher socioeconomic status. Since participants in our study had a high socioeconomic status, this may have resulted in an overestimation of breastfeeding rates and exclusive breastfeeding in our study. In contrast, total breastfeeding duration in our study population was shorter (18.8% for 11–12 months) than in the general population (41.1% for 12 months 5 ). This may be ascribed to MS-related reasons for weaning, like timely starting immunotherapy, most frequently reported in our study. Other studies comparing total breastfeeding time in pwMS have not be published to the best of our knowledge.
A key finding of our survey, to our knowledge not investigated or reported in the literature before, was that reasons for weaning were predominantly MS related in around two thirds of participants. Most frequent reasons for weaning were in descending order, starting postpartum immunotherapy, the patient's fear of MS deterioration, a relapse postpartum, and the recommendation for weaning by a physician or midwife. Therefore, education of patients as well as professionals involved in prenatal and postnatal counseling regarding frequent and avoidable reasons for weaning may increase breastfeeding duration.
Although surprisingly general breastfeeding counseling had only a marginal effect on breastfeeding rate and duration in our study, targeted counseling regarding MS-related reasons, like fear from MS deterioration or the need to start postpartum immunotherapy, may increase the proportion of pwMS and their children who may benefit from longer nursing periods. This may be of increasing importance since more drugs have recently been approved for use during breastfeeding, for example, glatiramer acetate and ofatumumab. The need of intensifying education is reflected by the statement of >40% of our participants requesting more information on breastfeeding in MS. Interestingly, gynecologists, midwives, and lactation consultants were underrepresented in prepartum counseling on breastfeeding in MS. Since, especially, midwives and lactation consultants, and gynecologists frequently contact and come together with mothers in the context of prenatal care, the awareness of these professional groups should be raised regarding the particularities of breastfeeding in MS.
In our study, the relapse rate within 2 years before birth had no effect on breastfeeding rate, total breastfeeding time, or duration of exclusive breastfeeding. This is in line with other studies that could not identify an impact of the disease activity on the decision to breastfeed.2,3 However, these studies focused on a period of 2 years before pregnancy.
While in our survey we found no influence of DMD use within the 2 years before birth on breastfeeding success, other studies showed that pwMS receiving DMDs in the time before pregnancy were less likely to exclusively breastfeed their infants1,2,9 (n = 32 pwMS in Langer-Gould et al 9 ).
However, observation periods were different. A limitation of our study is that, despite numerous efforts to recruit participants, the number was lower than expected, resulting in potentially underpowered statistical testing. Furthermore, the study is not population based and might overestimate the real number and duration of breastfeeding.
Conclusion
In conclusion, our study gives an important insight into the breastfeeding situation in MS in Germany, providing data for improving counseling. Currently, an increasing number of DMDs may be used while breastfeeding according to their approval. This in conjunction with patient education, especially regarding frequent and avoidable reasons for weaning, may result in higher breastfeeding rates, making more children and mothers benefit from the health-related advantages of breastfeeding.
Footnotes
Authors' Contributions
S.A.: conceptualization (equal); writing—original draft (lead); formal analysis (lead); methodology (equal); investigation (equal); and data curation (equal). Ko.H.: conceptualization (supporting); writing—review and editing (equal); and investigation (supporting). L.C.: writing—review and editing (equal) and investigation (supporting). K.H.: writing—review and editing (equal) and investigation (supporting). F.T.N.: conceptualization (supporting); writing—review and editing (equal); and investigation (supporting). A.B.: Project administration (lead); conceptualization (equal); writing—review and editing (equal); investigation (equal); data curation (equal); and supervision (lead).
Disclosure Statement
S.A.: the author declares that there is no conflict of interest. Ko.H.: the author declares that there is no conflict of interest. L.C. received personal and as head of Neuropoint GmbH compensation, grants for congress travel and participation from Merck Serono, Roche, Novartis, Biogen, TEVA, Roche, Sanofi/Genzyme, Mylan, and Celgene/BMS, Janssen. K.H. received personal compensation and research grants from Merck Serono, Biogen, Novartis, TEVA, Roche, Sanofi/Genzyme, and Celgene/BMS, Janssen. F.T.N. received personal compensation from Biogen, Celgene/BMS, Janssen, Merck Serono, and Roche. He received grants for congress travel and participation from Biogen and Merck Serono. A.B. received personal compensation from Merck Serono, Biogen, Novartis, TEVA, Roche, Sanofi/Genzyme, and Celgene/BMS, Janssen. He received grants for congress travel and participation from Biogen, TEVA, Novartis, Sanofi/Genzyme, Merck Serono, Celgene, and Janssen.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.