
Abstract
Objective:
The objective of this study was to provide global breast milk intake estimates for infants and children from 0 to 3 years old.
Materials and Methods:
A systematic search of online databases (Embase, MEDLINE, and CENTRAL) was conducted and complemented with a manual search of additional databases (African Journals Online and LILACS), reference lists, and unpublished data. Studies with apparently healthy mothers and their children 0–3 years old worldwide were included. Random effects meta-analyses, subgroup analyses, and meta-regressions were conducted.
Results:
A total of 167 studies on breast milk intake were identified. The mean daily breast milk intake among all the studies included was 670 mL per day and 117 mL/kg per day. Breast milk intake was influenced by infant age, infant body weight, and breastfeeding practices. The deuterium dilution method tended to yield higher estimates than test-weighing methods. Breast milk intake over time was modeled with a nonlinear meta-regression: breast milk intake (mL/day) = 51–1.4 × days +180 × log(days). When restricting to studies involving healthy term infants exclusively breastfed up to 6 months, breast milk intake was 624 mL per day and 135 mL/kg per day at 1 month, 735 mL per day and 126 mL/kg per day at 3 months, 729 mL per day and 107 mL/kg per day at 6 months, and 593 mL per day and 61 mL/kg per day at 12 months.
Conclusions:
This review provides global breast milk intake estimates for infants and young children. It demonstrates differences in intakes according to region and measurement method, as well as longitudinal changes over the first year of life.
Introduction
Breast milk is the key component of the diet and an important source of nutrient intake in infants and young children. It is assumed that breast milk from healthy well-nourished women provides adequate amounts and concentrations of nutrients required for optimal growth of infants. Accordingly, the World Health Organization (WHO) recommends that infants should be exclusively breastfed for the first 6 months of life, and thereafter should receive nutritionally adequate and safe complementary foods, while continuing to breastfeed for up to 2 years or beyond.1,2
Data on breast milk intake can be used to assess infant feeding and to determine nutrient requirements for infants and young children. However, amounts of breast milk consumed can vary throughout the first years of life and across different populations. It is, therefore, important to have estimates of breast milk intake that are based on a wide variety of samples collected in a systematic manner.
In 1998, WHO published a report on complementary feeding in young children 3 with mean breast milk intakes in developing and industrialized countries. These values have been used widely to estimate breast milk intakes and to derive values, such as energy intake from breast milk, in clinical and research settings. Since then, several reviews on breast milk intake have been published, but have either been restricted to a limited number of studies, 4 or regions, 5 or focused on the comparison of different measurement methods. 6 A systematic review providing updated breast milk intake estimates for infants and young children representative of different regions across the world is needed.
This review was commissioned by the Food and Agriculture Organization of the United Nations (FAO) and WHO, to inform their work on updating nutrient requirements and safe upper levels of intake in infants and young children, originally established in 2004. 7 The objective of this systematic review was to provide estimates of breast milk intakes in infants and children from birth up to 3 years of age around the world.
Materials and Methods
Eligibility criteria
We included studies with apparently healthy, free from any clinical signs or symptoms of undernutrition or illness that might impact milk production, lactating women, and their offspring 0–35.9 months of age. Mothers and infants with severe or moderate acute malnutrition, and infants with enteral or intravenous feeding, diarrhea, Wilson's disease, or familial hypophosphatemia were excluded. However, women with chronic conditions, such as obesity, diabetes, or HIV, and infants with low birth weight or born prematurely were included.
We included studies that reported breast milk intake. Studies in which the breast milk intake measurement method was not reported, in which breast milk production or expression was measured without child intake, in which the breast milk intake was measured for <12 hours, or in which sample size and units were not reported, or where standard deviations (SD) could not be derived, were excluded. Intervention studies, cohort studies, cross-sectional studies and case–control studies were included. Conference abstracts, posters, commentaries, editorials, and studies for which full texts were unobtainable were excluded. Studies from all regions of the world, in all languages, and of any date of publication were included.
Search strategy
The online databases MEDLINE, MEDLINE In-Process and Other Non-Indexed Citations, EMBASE, and Cochrane Central Register of Controlled Trials (CENTRAL) were searched up to October 1, 2020 (Supplementary Files). Moreover, the African Journals Online (on December 11, 2020) and the LILACS database (on December 18, 2020) were searched to improve geographical coverage of the search. The reference lists of recent systematic reviews and included reports were screened manually. An update of the search was conducted in EMBASE on November 17, 2022, to identify new articles published.
Moreover, the International Atomic Energy Agency (IAEA) provided unpublished data from a selection of studies (IAEA, unpublished data, Country investigators: Africa: Amoussa Hounkpatin WBA, Kenguela Wabolou P, Lartey A, Bansa DK, Karuri EG, Nduati R, Owino V, El Kari K, Coutsoudis A; Asia: Urio EM, Thomas T, Fadjarwati T, Winarno EK, Karim N, Ahmed T, Yameen A, Hettiarachchi M, Winishagoon P, Poncharoen T, Nga TT; Latin America: Pallaro AN, Ramos Silva V, Weisstaub SG, Hernández Triana MT, Mieses Consepción KM, Aguilar Lema EM, Ramírez-Zea M, Della Santa Méndez AP. Breastmilk intake in infants by the dose to mother technique. 2021 Mar.).
Selection process
The identified records were imported into Covidence 8 and duplicates were merged. The records were screened for eligibility first by the title and abstract, and then by the full-text, in duplicate by two researchers. Any disagreement on the exclusion or inclusion of a report between the two reviewers was resolved by discussion between the two reviewers or by a third reviewer. For the update of the review, screening was done by one single reviewer.
Data extraction
Information on the study design, the participants, as well as the measurement methods was extracted. Values for breast milk intake per day and per body weight were extracted. If data were only available from figures, they were extracted with PlotDigitizer. 9 For trials, data were extracted solely from baseline or from the control group, except if the intervention was relevant to subgroup analyses or if there were no significant effect of the intervention. Data were extracted in Excel by one researcher and a subset was verified by another researcher. Whenever reported, predominantly breastfeeding was merged together with exclusive breastfeeding.
Data analysis
Data transformations and imputations were done according to the Cochrane Handbook for Systematic Reviews of Interventions
10
and following the recommendations of Borenstein et al.
11
If means and SD were not reported, they were imputed from 95% confidence interval
To calculate an overall mean breast milk intake per day and per body weight per day, random effects meta-analyses were conducted. Outlying and influencing studies were identified with Baujat plots. Subgroup analyses were conducted to investigate differences by lactation stage (colostrum 1–4 days postpartum [pp], transitional milk 5–15 days pp, and mature milk >15 days pp), health status (healthy versus condition), maternal age (adolescents versus adults), maternal body mass index (BMI), maternal anemia (yes versus no), gestation duration (term versus preterm), breastfeeding practice (exclusive/predominantly breastfeeding versus partial/mixed breastfeeding), country income category, continent, and measurement method.
A complementary analysis was limited to the studies that would provide the best quality estimates of breast milk intake, the “key studies,” studies with only healthy mothers and infants who were born at term, and, <6 months of age, exclusively breastfed.
The evolution of breast milk over time was plotted and fitted with a local polynomial regression. Then meta-regressions were conducted with several models (i.e., linear, quadratic, cubic, exponential, logarithmic, and restricted cubic splines) and the model with the best fit was selected based on Akaike information criterion. Statistical analyses were conducted with RAnalyticFlow (version 3.1.8) with the package meta.
Results
Study characteristics
From 5,064 records identified, a total of 167 studies including 20,857 participants were included. The flowchart of the study selection process is shown in Figure 1. The detailed characteristics of each included study are shown in the Supplementary Files. The study designs were cohorts (N = 81), cross-sectional studies (N = 46), trials (N = 35), and case–controls studies (N = 5). The studies were conducted in all continents of the world, with 50 studies in North America, 38 studies in Africa, 37 studies in Asia, 31 studies in Europe, 21 studies in Australasia/Oceania, and 20 studies in South America.
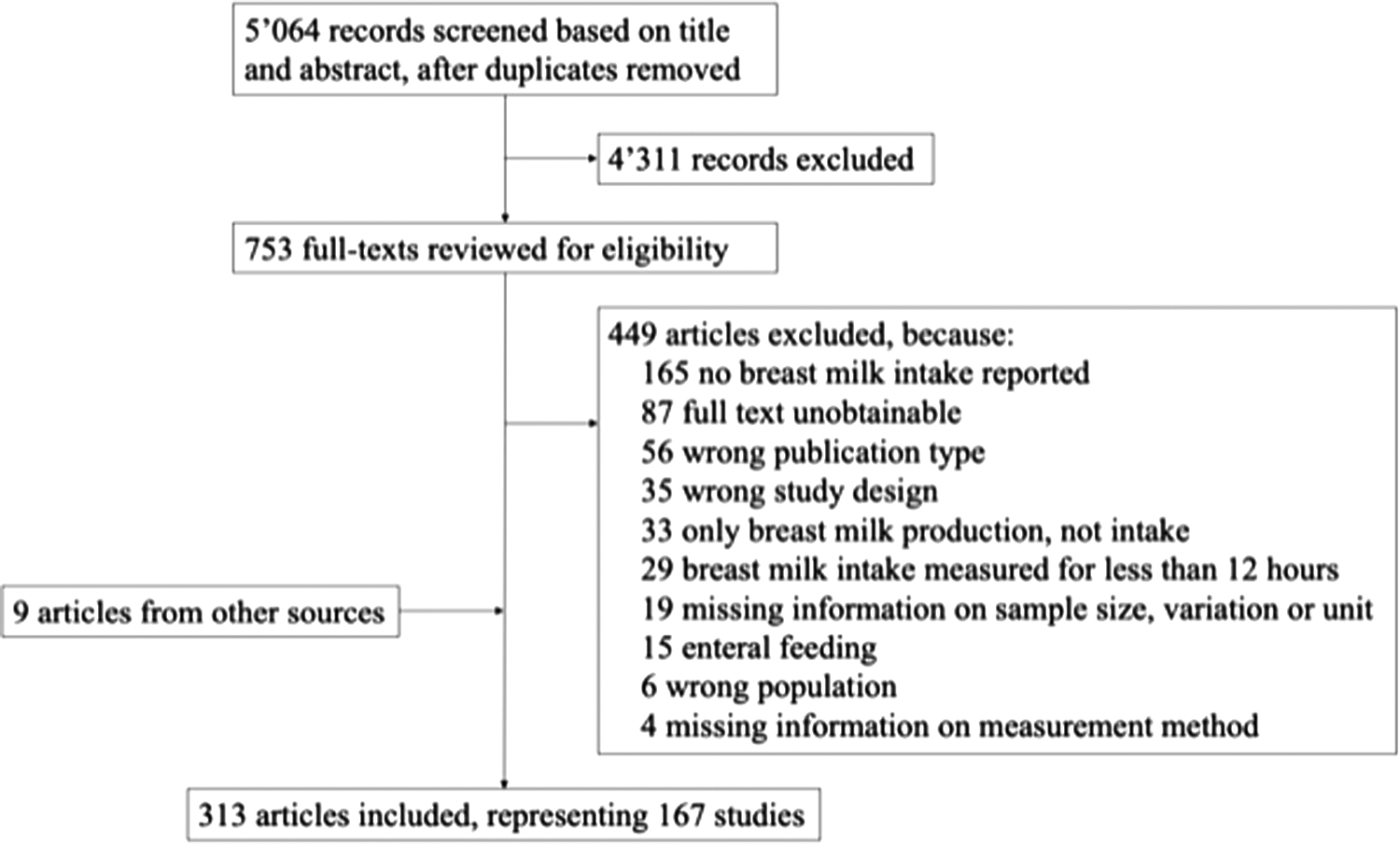
Study selection flowchart.
The countries with the most studies identified were the United States (N = 39) and Australia (N = 21). The majority of the studies included healthy populations (N = 99), many did not specify health status (N = 61), and a few included populations with conditions (N = 7). The conditions were diabetes type 1 (N = 1), diabetes type 1/gestational diabetes (N = 1), diabetes type 2/hyperthyroidism/hypothyroidism/ovulatory disturbance (N = 1), HIV (N = 1), mastitis (N = 1), persistent nipple pain (N = 1), and ankyloglossia (N = 1). The majority of the articles did not specify the nutritional status of their study population (N = 145), whereas some included population with a good nutritional status (N = 7), others with a suboptimal nutritional status (N = 15).
The methods used to determine breast milk intake were test-weighing (N = 113), deuterium dilution (N = 49), and both test-weighing and deuterium dilution (N = 5). The majority of the test-weighing was done by weighing the infant, except for two studies that used maternal test-weighing. Test-weighing was either self-managed by the mothers (N = 61) or conducted under observation or by a researcher (N = 34) or not reported (N = 23). The duration of test-weighing varied between 12 and 168 hours, with the majority being 24 hours (N = 58). Only 15 studies mentioned having corrected for insensible water losses. The scales used were electronic (N = 65), mechanical (N = 12), electronic and mechanical (N = 1), or unspecified (N = 39). The deuterium dilution technique was conducted by administering deuterium to the mothers (N = 47) and in some cases the infants (N = 7), with samples of saliva (N = 32), urine (N = 16), saliva or urine (N = 4), or unspecified (N = 2).
Meta-analysis
The mean intake of breast milk was 670 mL per day (95% CI: 630–710), ranging from 84 to 992 mL per day. Six outliers were identified and could be explained by the extreme ages of the infants included: Four were from studies with infants in the first days of life and two were with children of 2 years and above. The mean intake of breast milk per body weight was 117 mL/kg per day (95% CI: 112–122), ranging from 50 to 191 mL/kg per day. One outlier was identified, which was a study with infants between a large age range (1–12.5 months old).
The breast milk intakes among different subgroups are summarized in Table 1. Breast milk intake increased over the different lactation stages, from colostrum to transitional and mature milk. Breast milk intake was higher among healthy populations, exclusively breastfed infants, and when measured with deuterium dilution than with test-weighing and differed between continents (i.e., the lowest values were found in Asia), but did not differ between country income categories. Breast milk intake also did not differ between adolescent and adult mothers (noting there was only one study with adolescent mothers).
Summary of Subgroup Meta-Analyses for Breast Milk Intake Volume (mL/Day)
p-Value for difference between groups without “Unspecified/Mixed” group.
p-Value for difference between groups for all groups.
CI, confidence interval.
No studies were identified to permit the comparison of breast milk intake from anemic versus nonanemic women (i.e., only one study explicitly excluded women with severe anemia, 12 the other studies did not specify anemia status). The subgroup meta-analysis by maternal BMI was not possible because nearly all studies included several BMI categories, making comparisons not meaningful. However, a meta-regression with mean BMI was conducted. The association between maternal BMI and breast milk intake was nonsignificant (p = 0.867).
The daily breast milk intakes per body weight among different subgroups are summarized in Table 2. The differences between healthy and unhealthy populations and between regions became nonsignificant. The other significant and nonsignificant differences between subgroups, respectively, remained the same as for total breast milk intake.
Summary of Subgroup Meta-Analyses for Breast Milk Intake Volume per Body Weight (mL/kg per Day)
p-Value for difference between groups without “unspecified/mixed” group.
p-Value for difference between groups for all groups.
CI, confidence interval.
The differences between the measurement methods were further explored. Five studies compared deuterium dilution and test-weighing with measured breast milk intake in the same sample of infants.13–17 Four of the five studies found significantly higher values with deuterium dilution than with test-weighing (one was nonsignificant). When deuterium was administered to mothers, values tended to be closer to test-weighing results than when administered to infants. Differences between deuterium dilution and test-weighing tended to also be smaller when test-weighing values were corrected for insensible water losses.
When comparing all the studies that measured deuterium administered to mothers and all the studies that corrected for insensible water losses in test-weighing, the differences between methods became nonsignificant (deuterium dilution: N = 46, estimate: 744, 95% CI: 713–776, and test-weighing corrected for insensible water losses: N = 14, estimate: 735, 95% CI: 690–781, p-value: 0.749), indicating that the true breast milk intake probably lies between the two estimates from deuterium dilution and test-weighing.
Meta-regression
The evolution of breast milk intake per day and per body weight at different ages of the infant is shown in Figures 2 and 3, respectively. The intake of breast milk increases sharply over the first month and then reaches a plateau ∼3–4 months, and starts slowly decreasing with the introduction of solid foods. The meta-regression model fitting the data the best was the logarithmic model. The meta-regression results are depicted in Figures 4 and 5. Table 3 provides breast milk intake estimates from key studies only at different ages from 1 to 24 months old estimated from the meta-regression model.
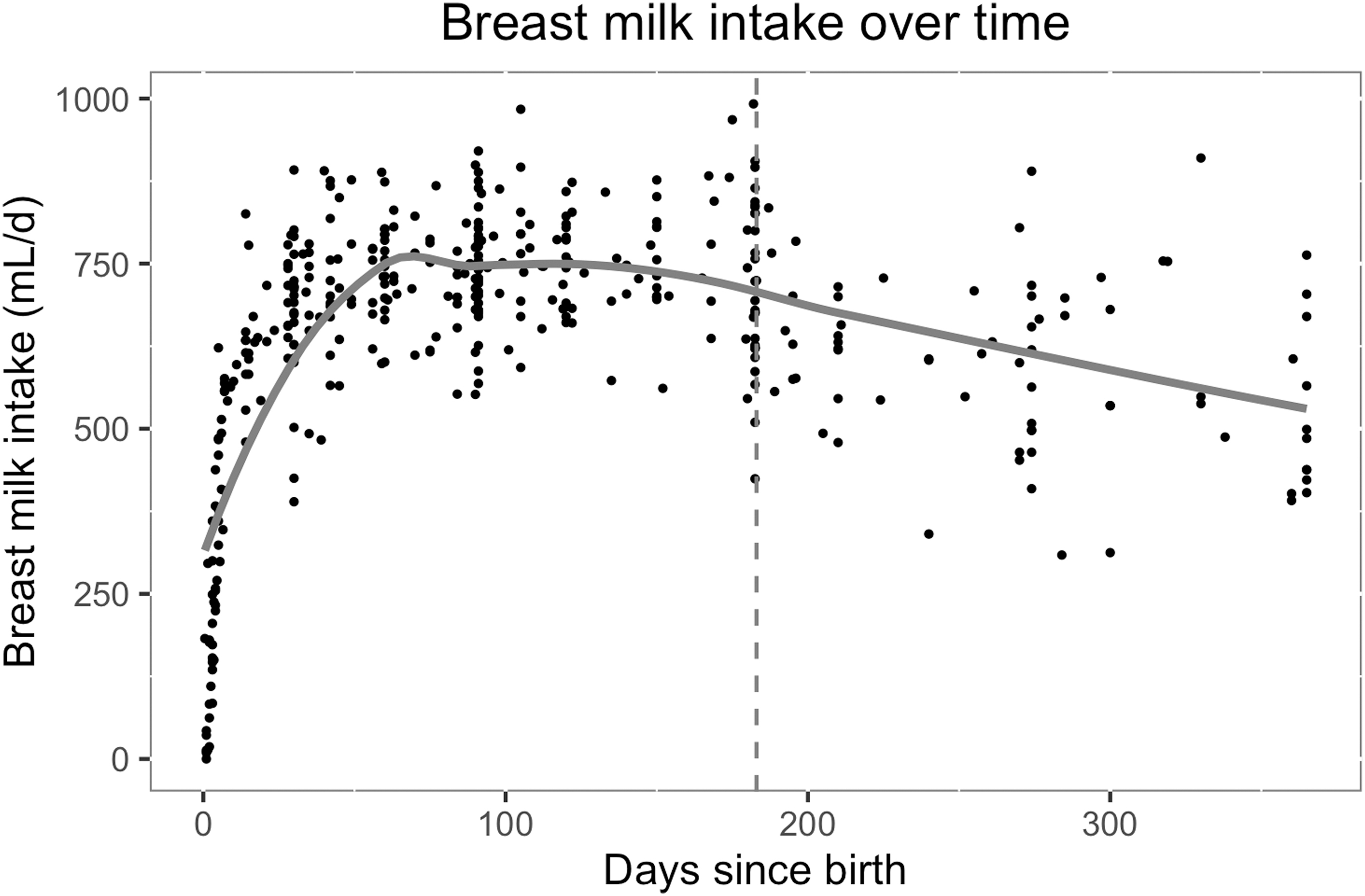
Breast milk intake (mL/day) over time (in days since birth), with local polynomial regression (
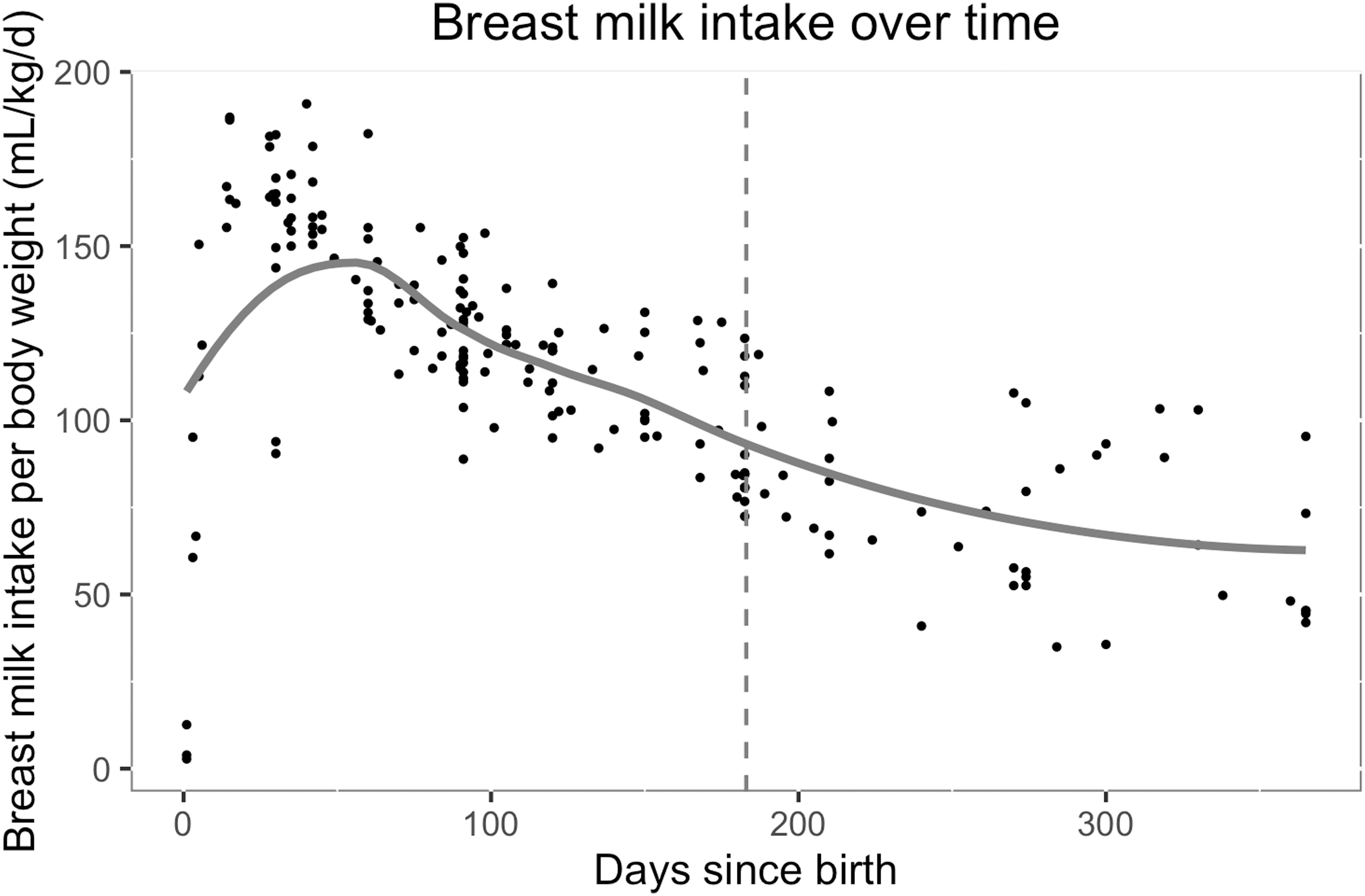
Breast milk intake per body weight (mL/kg per day) over time (in days since birth), with local polynomial regression (
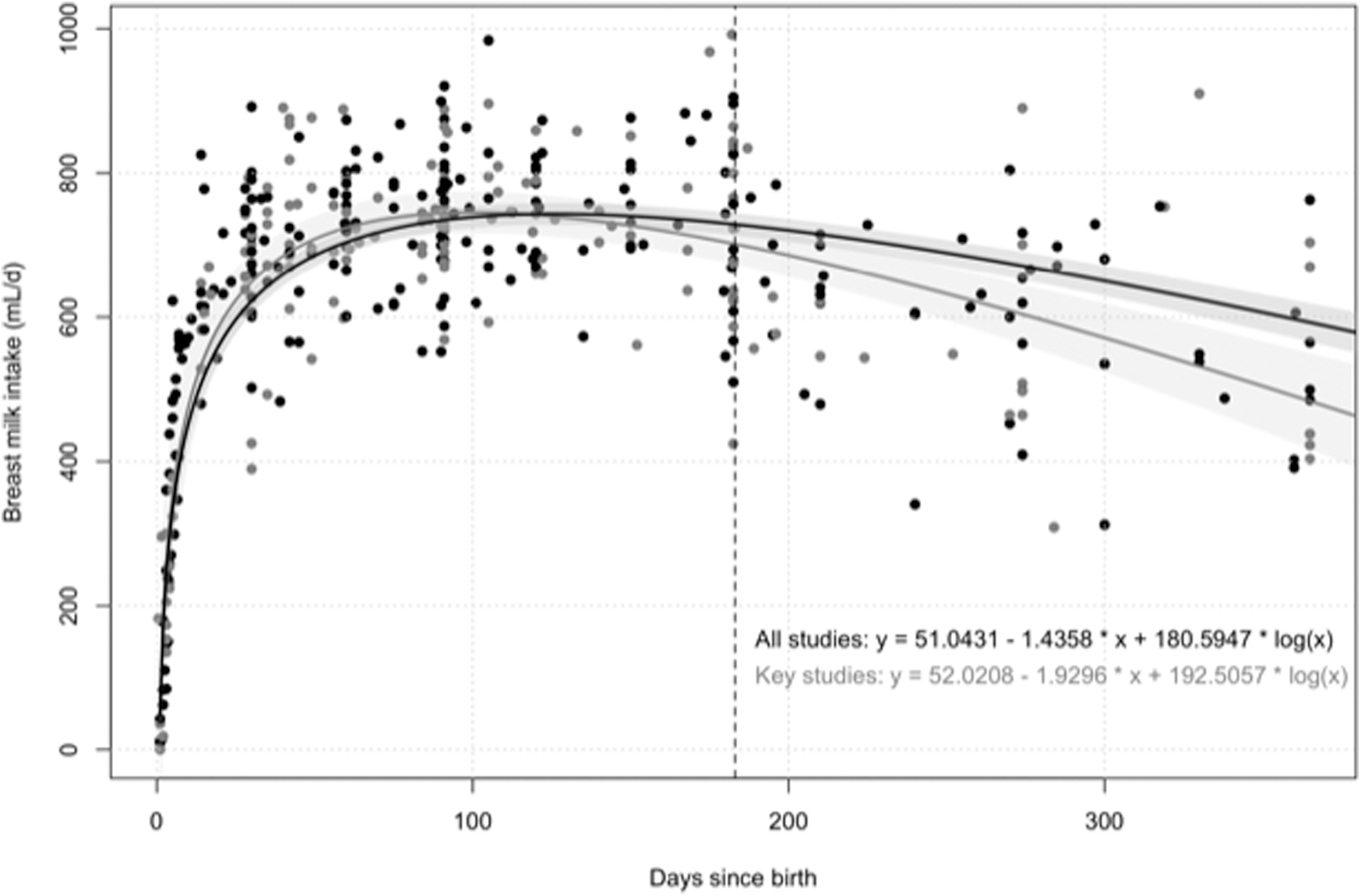
Breast milk intake (mL/day) over time (in days since birth) with log meta-regression with all (
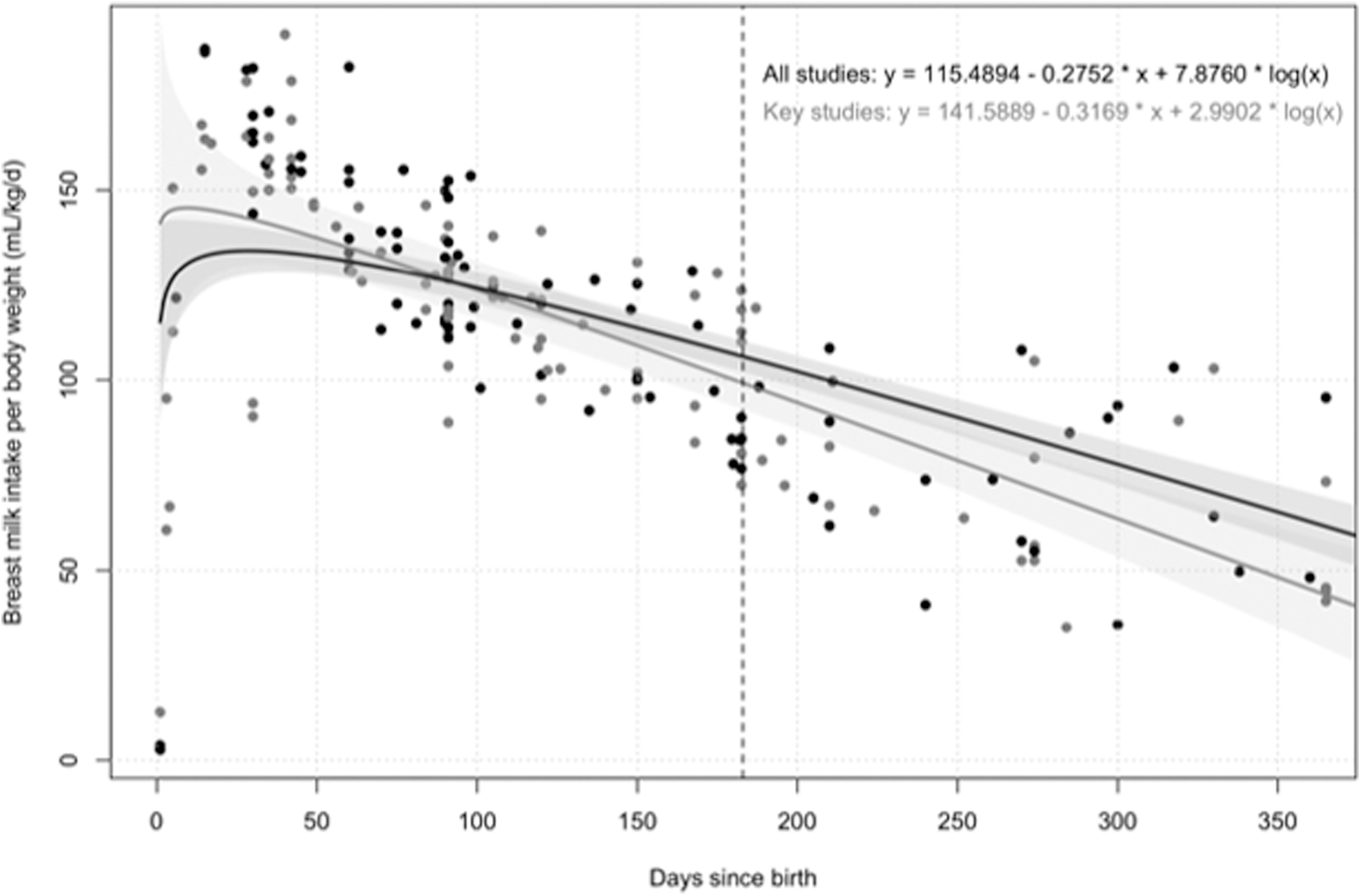
Breast milk intake per body weight (mL/kg per day) over time (in days since birth) with log meta-regression with all (
Mean Breast Milk Intake (95% Confidence Interval) from 1 to 24 Months of Age from Meta-Regression with Key Studies a
Healthy, term children exclusive breastfeeding up to 6 months.
There were insufficient studies >17 months of age to provide reliable estimates.
Discussion
Summary of results
This systematic review included a large number of studies, from all continents. The mean breast milk intake for children 0–35.9 months old was 670 mL per day and 117 mL/kg per day. Breast milk intake increased rapidly over the first month (from 45 up to 621 mL/day), reaching a plateau ∼3–4 months (just below 750 mL/day), and starting a progressive decrease ∼4–6 months with the introduction of solid foods. The evolution of breast milk intake over time was best modeled with a logarithmic model. Breast milk intake was influenced by infant age, infant body weight, breastfeeding practices, and measurement methods.
Interpretation
The intakes of breast milk found in this review are comparable with the values in the previous WHO review 3 (Tables 4 and 5). The 22 studies included in the 1998 WHO review were identified through a systematic search of Medline and references lists. All studies included in the WHO review used test-weighing, except for one study that used deuterium dilution. Our review included all the studies from the 1998 WHO review and included more and ulterior studies. For the interpretation of the values per infant age category, it is important to note that the age distribution within each age category was not evenly distributed, which could have skewed the estimates toward one end of the age category.
Comparison of Breast Milk Intake with 1998 World Health Organization Review (mL/Day)
n = Number of participants.
Comparison of Breast Milk Intake with 1998 World Health Organization Review (mL/kg per Day)
n = Number of participants.
For example, in the 12–35.9 months age group, most of the studies were for children near 12 months old and few studies were available for children >24 months old. Therefore, the mean intake of breast milk in the 12–35.9 months would be more confidently applied to a 12-month-old infant, but less to a 35-month-old infant. To overcome this challenge, we conducted a meta-regression with age as a covariate.
Our review found that breast milk intake was influenced by infant body weight. Another review 18 found that breast milk volume was influenced by birth weight and gestational age, through differences in suckling strength, frequency, and duration. We were not able to assess differences in infants born term and preterm. Most of the studies comparing breast milk intake in term and preterm infants focused on milk expression only19–21 or used enteral feeding with the preterm infants,22–27 which were both criteria of exclusion in our review.
The latter review also found an influence of substance use, which we also could not assess, as most of the studies investigating the effect of the intake of different substances, such as contraceptive pills and growth hormones, focused on milk expression only,28–30 which was an exclusion criteria in our review. Other studies have found that maternal underweight does not influence breast milk production, 31 but maternal obesity does. 32 The absence of association between maternal BMI and breast milk intakes found in our review could have been due to the paucity of studies with women in the extreme BMI categories.
Concerning breast milk measurement methods, a systematic review 6 found that deuterium dilution and test-weighing methods were the best methods to measure breast milk intakes. Our review included only studies that used one of these two methods. However, both the deuterium dilution and test-weighing methods are still prone to errors resulting in possible over-estimation of intake with deuterium and underestimation with test-weighing.13–15 For example, deuterium dilution administered to mothers and measured in mothers and infants in saliva samples can provide more accurate estimates than when administered to infants or measured in urine samples.33–35
Test-weighing should be conducted by a researcher or by the mother under observation to avoid missing feeds, using an electronic scale to increase precision, and corrected for insensible water losses.6,36 In our review, the actual intakes of breast milk probably lie between the two estimates with the two different methods. When comparing deuterium dilution administered to mothers and test-weighing corrected for insensible water losses, the gap between the two estimates was narrower and became nonsignificant.
Strengths and limitations
A strength of this review is the considerate effort was made to cover as much as possible of the literature available on the topic, in terms of dates, language, and geography. In fact, a broad systematic search strategy was developed and complemented with additional searches, including searches of African and Latin American literature databases. Studies from all the continents were identified. Another strength of this study is the multiple subgroup analyses conducted to compare different groups of populations and study influencing factors. Moreover, a meta-regression was conducted to be able to model the effect of age on breast milk intake. The analyses restricted to the key studies give values of breast milk intakes of high quality and can be used as a reference.
A limitation of this review is the information available from the studies. Several studies did not provide sufficient information on influencing factors, especially on nutrition status. The results of the subgroup analyses should be interpreted with caution 10 as the studies were unevenly distributed between some of the subgroups (i.e., healthy versus unhealthy, adult versus adolescent mothers). Another limitation is that only study-level data were available. If individual-level data had been available, a more detailed and precise analysis could have been conducted. The Mothers, Infants and Lactation Quality study is an ongoing study whose goal is to establish reference values for breast milk by collecting individual-level data from well-nourished women and infants in four countries. 37 It will be useful to compare the results of the latter study, when available, with our review.
Conclusion
In conclusion, this study updates the 1998 WHO breast milk estimates 3 and is currently the most up-to-date and comprehensive systematic review on the topic to our knowledge. Results of this review can be used as an aid in assessing infant and young child nutrition, including the estimation of nutrient intakes and requirements.
Footnotes
Acknowledgments
We thank Dr Jason Montez for conducting the database searches and for providing inputs on the analyses and the report. We also thank the FAO/WHO expert group on nutrient requirements for children aged 0–36 months for their inputs, the IAEA for providing unpublished data from IAEA-supported projects and for their comments on the report, and the WHO translation team, Rain Yamamoto and Darius Rohani, for translating full texts.
Authors' Contributions
M.R.L. designed the research protocol. M.R.L. and Q.Y. screened the studies for the original review and M.R.L. screened the studies for the update. M.R.L. extracted the data for all studies, except for the studies in Chinese, which were extracted by Q.Y. Q.Y. verified a subset of the extracted data. M.R.L. conducted the analyses. M.R.L. wrote the report and Q.Y. provided inputs.
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this study was provided to M.R.L. and Q.Y. by the Food and Agriculture Organization of the United Nations (FAO) and World Health Organization (WHO).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.