
Abstract
Background:
Breastfeeding is especially beneficial to women with diabetes and their infants, yet diabetic mothers frequently experience less favorable breastfeeding outcomes.
Objectives:
To identify facilitators and barriers to breastfeeding for women with diabetes by comparing cognitive and social factors, health and hospital-related factors, and breastfeeding outcomes between women with and without diabetes.
Design/Methods:
Women with any type of diabetes (n = 28) and without diabetes (n = 29) were recruited during pregnancy. Data were collected from the electronic medical record and maternal surveys at 24–37 weeks' gestation, birth hospitalization, and 4 weeks' postbirth. We compared differences in mother's regard for breastfeeding, breastfeeding intention, and birth hospital experience by diabetes status, and estimated odds ratios for exclusive breastfeeding (EBF) and unmet intention to breastfeed.
Results:
Women with and without diabetes had similar breastfeeding intentions, attitudes, and self-efficacy. Women with diabetes were less likely to EBF, and more likely to have unmet intentions to EBF at hospital discharge, compared to women without diabetes. At 4 weeks' postpartum, there was no difference in breastfeeding by diabetes status, although EBF at hospital discharge was strongly associated with EBF at 4 weeks. Infant neonatal intensive care unit (NICU) admission and hypoglycemia were significantly associated with diabetes status, reduced EBF rates, and unmet breastfeeding intentions.
Conclusions:
Despite having a strong intent to breastfeed, women with diabetes experienced less favorable early breastfeeding outcomes and were less likely to meet their own breastfeeding goals. These differences may be driven by neonatal complications, such as infant hypoglycemia and NICU admissions, rather than maternal cognitive and social factors.
Introduction
Diabetes is one of the most common complications of pregnancy, impacting an estimated 16.8% of births worldwide, and between 2% and 11% of births in the United States, depending on race and ethnicity.1,2 The majority of women who have diabetes during pregnancy have gestational diabetes mellitus (GDM), which develops during pregnancy, whereas a smaller, but growing number are affected by pre-existing type 1 or type 2 diabetes mellitus.1,2 Breastfeeding has well-known health benefits for all mothers and infants, and there is growing evidence that it may be especially beneficial for women with diabetes. 3 In particular, studies have shown that breastfeeding may improve postpartum glucose tolerance and short- and long-term insulin sensitivity. 4 Breastfeeding may also reduce lifelong risk of obesity and type 2 diabetes for infants of mothers with GDM.5,6
Despite these benefits, women with diabetes tend to have less favorable breastfeeding outcomes.7,8 Most studies of the causes of lower rates of breastfeeding initiation, 9 reduced duration of any breastfeeding, 10 and shorter duration of exclusive breastfeeding (EBF)7,8 were performed in cross-sectional survey or vital statistics data. 10 No study has prospectively followed and compared women with and without diabetes through the continuum of pregnancy and the postpartum period to determine factors that may impede or protect breastfeeding.
Therefore, we aimed to identify facilitators and barriers to breastfeeding for women with diabetes by prospectively comparing infant feeding intentions and attitudes, breastfeeding self-efficacy, neonatal and postpartum complications, and breastfeeding outcomes between women with and without diabetes.
Methods
Participants and study design
In this prospective cohort study, after obtaining institutional regulatory approval, participants were recruited during pregnancy from either the obstetric clinics in the Yale Medicine network or from Yale EPIC MyChart. Maternal inclusion criteria included the following: (1) singleton pregnancy, (2) ≥18 years of age, (3) pregnancy 12–37 weeks' postmenstrual age (PMA), and (4) planning to deliver at Yale New Haven Hospital (YNHH).
If informed consent was obtained and when 24–37 weeks' PMA, participants were asked to complete a series of surveys and to allow abstraction of data from the maternal and infant medical records for prenatal care and the birth hospitalization (outlined below). Surveys were administered at 2 prenatal time points (24–32 weeks and 33–37 weeks) and two postnatal time points: birth hospitalization and 4–6 weeks posthospital discharge. Some participants enrolled in the study at 33–37 weeks' PMA and completed just one time point of prenatal surveys.
Measurement tools
Demographics
Race/ethnicity, age, education, parity, and type of health insurance were obtained from each mother's electronic medical record.
Health and hospital factors
Diabetes status (type 1, type 2, gestational, or no diabetes), infant due date, and mode of delivery were obtained from each mother's electronic medical record. From the infant's chart, we obtained infant date of birth; weight; sex; neonatal intensive care unit (NICU) admission; and medical diagnoses, including hypoglycemia (defined as asymptomatic hypoglycemia requiring intervention; hospital protocol recommends treatment for infants with glucose <40 mg/dL from birth to 4 hours, <45 mg/dL from 4 to 24 hours, or <50 mg/dL from 24 to 48 hours).
Cognitive and social factors
Infant feeding intentions
Participants completed the Infant Feeding Intentions Scale (IFIS)11,12 at both prenatal visits (24–32 weeks and 33–37 weeks). The IFIS is scored 0–16, where the highest score represents very strong intention to provide breast milk as the sole source of milk for the first 6 months. We used each participant's most recently completed IFIS for this study.
Infant feeding attitudes
Participants completed the Iowa Infant Feeding Attitudes Scale (IIFAS) at 33–37 weeks PMA. The IIFAS measures attitudes toward breastfeeding and infant formula, including attitudes about the cost, convenience, health benefits, and social consequences of each feeding method. We also used two adapted versions of H & H Lactation Scale, which includes three subscales (maternal confidence/commitment breastfeeding, perceived infant breastfeeding satiety, and maternal infant breastfeeding satisfaction). 13 Scale items were worded in the present tense for mothers who indicated that they were still breastfeeding (e.g., “I feel a sense of pride from watching my baby grow from my breastmilk”) and in the past tense for mothers who tried breastfeeding, but were no longer breastfeeding at the time they completed the scale (e.g., “I felt a sense of pride…”).
Breastfeeding self-efficacy
We assessed breastfeeding self-efficacy during pregnancy and shortly after delivery in all participants who indicated an intention to breastfeed. At 33–37 weeks PMA, participants completed the prenatal breastfeeding self-efficacy scale (P-BSES). The P-BSES measures breastfeeding self-efficacy during the prenatal period, including the following domains: (1) skills and demands for breastfeeding or pumping, (2) gathering information about breastfeeding, (3) breastfeeding around other people, and (4) social pressure when breastfeeding. 14 During birth hospitalization, participants completed the Breastfeeding Self-Efficacy Short Form (BSES-SF). 15
Breastfeeding support
At 33–37 weeks PMA, we assessed participants' previous or planned use of 14 different sources of breastfeeding information and support. We used responses to this survey module to generate the total number of sources of support each participant used or planned to use.
Breastfeeding outcomes
Breastfeeding status at hospital discharge
We determined whether mothers were EBF at hospital discharge using infant feeding information in the electronic medical record from their hospital stay. We considered mothers to be exclusively breastfeeding at discharge if their infant received only breast milk in the last 24 hours before discharge.
Breastfeeding status at 4 weeks postpartum
We surveyed participants about their infant feeding practices at 4 weeks postpartum. Participants indicated whether or not they were still breastfeeding at all and reported the number of feedings in the previous 7 days of breast milk (from the breast or a bottle), formula, water, sugar water, other milk, juice, sweet drinks, baby cereal, or other foods. Participants were considered to be exclusively breastfeeding if they indicated giving only breast milk and no other food or drink in the past 7 days. These items were adapted from similar items used in the Infant Feeding Practices Study II (IFPS II). 16
Results
Data analysis
Means and standard deviations and frequencies and percentages were calculated to summarize scale and categorical variables, respectively. Maternal and infant characteristics were compared between women with and without diabetes using t-tests or Mann–Whitney U-tests for scale variables, and Chi-square or Fisher's Exact test for categorical variables, as appropriate. Simple logistic regression was used to estimate odds ratios (ORs) for EBF, unmet intention to exclusively breastfeed, and unmet intention to breastfeed in the last 24 hours of birth hospitalization. Data were analyzed using Stata 16.1. Statistical significance was established at alpha = 0.05.
Sample characteristics
In our sample of 57 women with a mean age of 31.5 years, 42.1% identified as non-Hispanic White, 33.3% as non-Hispanic Black, 17.5% as Hispanic, and 7.0% as other. Twenty-eight (49.1%) had any type of diabetes, including 4 (7.0%) with type 1 diabetes, 4 (7.0%) with type 2 diabetes, and 20 (35.1%) with gestational diabetes. Comparisons between women with and without diabetes are presented in Table 1. Women with diabetes were significantly more likely to be non-Hispanic White. Age, parity, education, and type of health insurance did not differ by diabetes status.
Maternal Demographic Characteristics
Statistically significant findings are bolded.
Education, n = 53 (of 57).
Insurance, n = 52.
Fisher's exact test.
SD, standard deviation.
Cognitive and social factors by diabetes status
In the bivariate analysis of cognitive and social factors related to breastfeeding outcomes (Table 2), women with diabetes were not significantly different from women without diabetes in terms of breastfeeding self-efficacy or attitudes toward breastfeeding, as measured by IIFAS and H & H lactation scale. However, there were trends toward higher IIFAS score and higher IFI score, which suggest more favorable attitudes toward breastfeeding and stronger intention to breastfeed (p < 0.10). Examples of responses to IFI scale items, by diabetes status, are presented in Figure 1. There was also no difference in the number or types of sources of social support for breastfeeding, although women in both groups most commonly cited doctors or physician assistants (91.2%), nurses (63.2%), lactation consultants (63.2%), and family (59.6%).
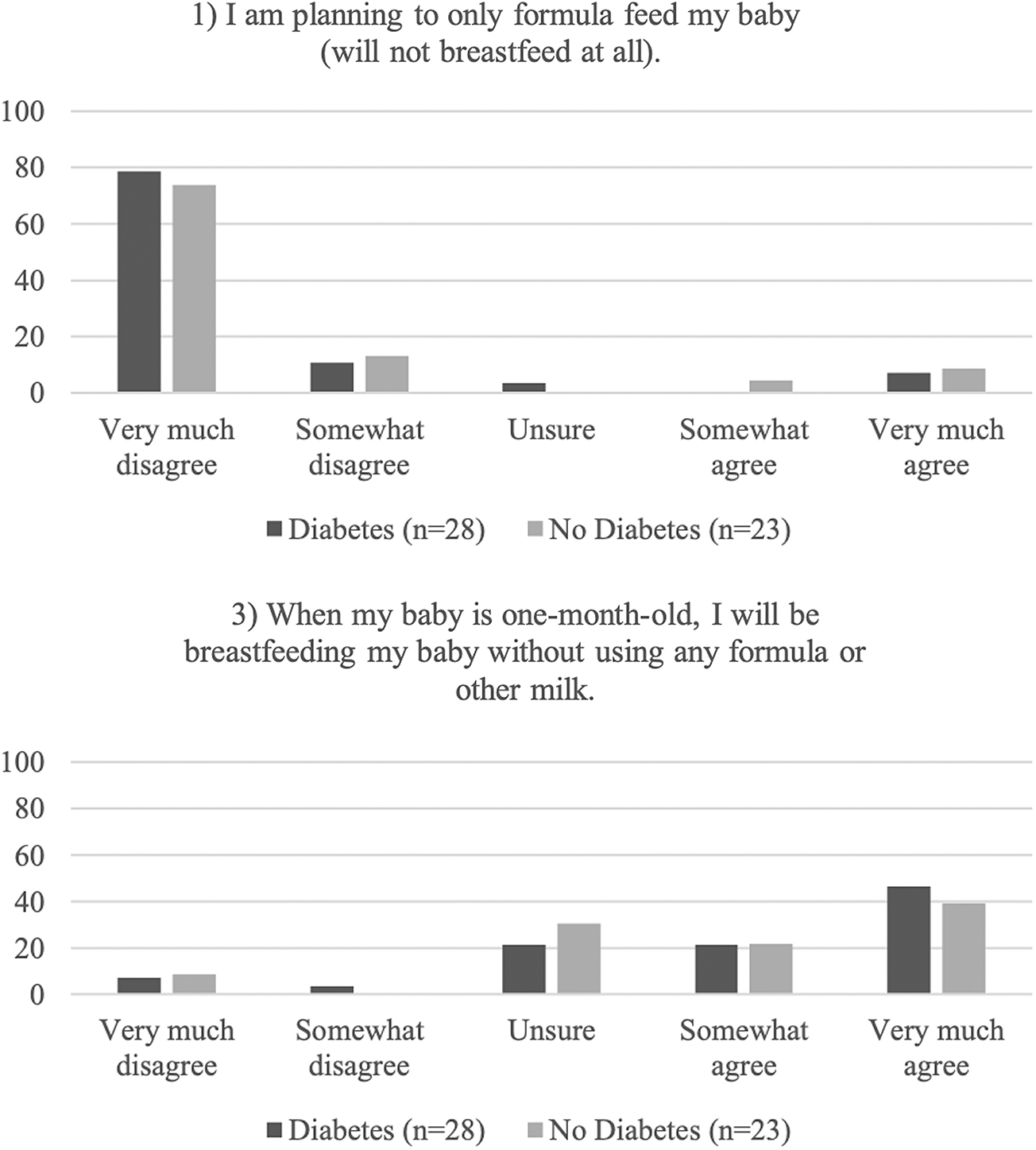
Percent of respondents selecting each answer choice for two items from the IFIS, by maternal diabetes status. IFIS, Infant Feeding Intentions Scale.
Maternal Cognitive and Social Factors
Breastfeeding intention (yes/no), n = 56 (of 57).
IIFAS, n = 43.
H & H scale and BSES, n = 48.
P-BSES, n = 49.
Fisher's exact test.
BSES, breastfeeding self-efficacy scale; IIFAS, Iowa Infant Feeding Attitudes Scale; P-BSES, prenatal BSES; SD, standard deviation.
Health and hospital factors by diabetes status
Maternal diabetes status was significantly associated with diagnosis of infant hypoglycemia and NICU admission (Table 3). There was no significant difference between groups in mode of delivery, infant sex, infant gestational age, or birth weight, although infant birth weight tended to be higher in the diabetes group (p = 0.08).
Health and Hospital-Related Factors
Statistically significant findings are bolded.
Gestational age, n = 56 (of 57).
Insurance, n = 52.
Fisher's exact test.
NICU, neonatal intensive care unit; SD, standard deviation.
Diabetes and breastfeeding outcomes
During hospital stay
A similarly high proportion of women in both groups (89.7% of women without diabetes and 89.3% of women with diabetes, p > 0.05) initiated breastfeeding. However, women with diabetes were less likely to exclusively breastfeed in the last 24 hours before discharge compared to those without diabetes (OR 0.17, 95% confidence interval [CI] 0.04–0.69). In the subsample of women who expressed an intention to exclusively breastfeed, women with diabetes were significantly more likely not to meet their goal (OR 17.4, 95% CI 3.28–92.61), as were those who expressed an intention to breastfeed at all (OR 8.0, 95% CI 1.89–33.85). We originally intended to compare formula supplementation during the hospital stay by diabetes status, but found that any formula supplementation was perfectly correlated with non-EBF in the last 24 hours of hospital stay.
In other words, none of the women whose infants received formula while in the hospital was able to establish EBF before discharge. In addition to maternal diabetes, infant NICU admission and hypoglycemia were significantly associated with reduced EBF rates and unmet breastfeeding intentions (Table 4). In fact, none of the women whose infants were diagnosed with hypoglycemia or admitted to the NICU exclusively breastfed in the last 24 hours before discharge or achieved their goal of any or EBF. Of the 14 infants with hypoglycemia, hypoglycemia was treated with formula in 10 (71.4%), oral glucose gel in 11 (78.6%), at-the-breast feed in 4 (28.6%), and expressed breast milk in 1 (7.1%). Eight (57.1%) infants received more than one type of treatment. Of the 6 (42.9%) infants who received just one type of treatment, two received formula and four received oral glucose gel.
Breastfeeding Outcomes at Hospital Discharge
All outcomes are based on the last 24 hours of hospitalization.
Fisher's exact test.
EBF, exclusive breastfeeding; NICU, neonatal intensive care unit.
Four weeks postpartum
Although there was no significant difference in breastfeeding outcomes or ability to meet EBF intentions at 4 weeks postpartum by diabetes status (Table 5), we found that EBF at hospital discharge was strongly associated with EBF at 4 weeks. Of those who were EBF at hospital discharge, 38.5% were still EBF at 4 weeks, compared to 3.6% of those who were not EBF at discharge (p = 0.008).
Breastfeeding Outcomes at 4 Weeks Posthospital Discharge
Fisher's exact test.
EBF, exclusive breastfeeding.
Discussion
In our study, women with diabetes had similar prenatal breastfeeding intentions, attitudes, and self-efficacy as those without diabetes, but were less likely to exclusively breastfeed and to meet their own breastfeeding goals by the end of their birth hospitalization. NICU admission and diagnosis of infant hypoglycemia, both of which were associated with diabetes status, may have contributed to the less favorable early breastfeeding outcomes in this population.
Breastfeeding outcomes and intentions
Our finding that mothers with diabetes were less likely to exclusively breastfeed during the last 24 hours of their hospital stay is consistent with previous research showing less favorable early breastfeeding outcomes in women with diabetes.7,8,17 Studies suggest that breastfeeding intention is an important predictor of outcomes in the general population 18 and diabetic populations,10,19 although few have compared breastfeeding intentions in women with and without diabetes. In one study, Loewenberg Weisband et al. 20 found that women with GDM had lower intentions to exclusively breastfeed in the first few weeks, whereas Finkelstein et al. 21 found no difference in breastfeeding intentions between pregnant women with and without diabetes. Our findings suggest not only similar but also a trend toward stronger breastfeeding intentions among women with diabetes during pregnancy.
Furthermore, there is very little literature on the extent to which women with diabetes meet their breastfeeding intentions. While the discourse around breastfeeding often centers around encouraging EBF, we believe it is important to examine whether mothers are able to achieve their own goals, and find ways to empower them to do so, as even strong intention may be overcome by external barriers. Our study is the first to our knowledge to report on the likelihood of meeting previously stated intentions to breastfeed and to find that mothers with diabetes are less likely to meet their intentions for any or EBF before hospital discharge. This finding prompts the exploration of prenatal and perinatal factors that influence breastfeeding outcomes.
At 4 weeks postdischarge, we did not find any difference in the odds of any or EBF, or in meeting intentions for EBF, by diabetes status. However, in our sample overall, those who exclusively breastfed in the last 24 hours of the hospital stay were more likely to exclusively breastfeed 4 weeks later, in agreement with evidence from other studies that in-hospital formula supplementation may impact longer-term breastfeeding success. A 2021 study by Whipps et al. 22 found that in-hospital formula supplementation reduced the likelihood of following a breastfeeding trajectory characterized by sustained EBF by 50%.
Chantry et al. 23 also found a reduced likelihood of EBF at 30–60 days among mothers who intended to EBF, but received formula supplementation in the hospital. In contrast, Loewenberg Weisband et al. 20 found no association between hospital formula supplementation and breastfeeding duration among women with GDM. Experimental evidence on the effects of formula supplementation on long-term breastfeeding outcomes has been mixed.24,25 When early limited formula supplementation was given as an intervention for infants who had initial larger than normal weight loss, it appeared to protect breastfeeding at 1 week and 3 months. 24 However, a larger trial found no difference in breastfeeding at 6 months. 25
Cognitive and social factors
Since earlier work shows key roles for cognitive and social factors in determining breastfeeding outcomes, we explored several of these factors in our sample. In particular, self-efficacy has been shown to significantly predict lactation success in the general population, 26 although very few studies have compared self-efficacy in diabetic and nondiabetic women. In a 2016 study of 67 Israeli women, Chertok and Sherby 27 found that maternal diabetes was associated with lower breastfeeding self-efficacy, but suggested that this difference was likely mediated by delayed secretory activation. In our study, we did not find any difference in either prenatal self-efficacy or postnatal self-efficacy, suggesting that maternal confidence does not explain the differences we observed in breastfeeding outcomes.
Health and hospital-related factors
Women with diabetes and their infants are at risk for several adverse pregnancy outcomes and hospital experiences that may serve as barriers to lactation.28,29 We found that NICU admission was associated with reduced odds of EBF, and reduced likelihood of meeting intentions for any BF before discharge. Previous evidence on the impact of NICU admission on breastfeeding outcomes is mixed. In their large 2008 study in the general population (n = 138,359), Colaizy and Morriss 30 found a positive association between NICU admission and breastfeeding at 4 weeks, although this was the case only in preterm infants. In contrast, in a smaller GDM population, Morrison et al. found that admission to special care nursery was associated with breastfeeding cessation before 3 months. 29
Maternal diabetes is also a well-known risk factor for infant hypoglycemia,27,31 and our results support this finding. Proper management of hypoglycemia is imperative, as hypoglycemia may lead to neurological damage or death. However, treatment often involves formula supplementation, serving as a potential barrier to lactation. The 2011 American Academy of Pediatrics (AAP) guide and algorithm for the screening and subsequent management of neonatal hypoglycemia state “any approach to management [of hypoglycemia] …should not unnecessarily disrupt the mother-infant relationship and breastfeeding.” 32
At the hospital, where participants in our study received care, the protocol for treatment of asymptomatic hypoglycemia is based on the 2011 AAP guideline and recommends formula supplementation for those who intend breastfeeding only when mothers are “unavailable due to complications or general anesthesia.” 32 Potentially, this would lead to a disparity due to mode of delivery; however, we did not find delivery mode to be associated with diabetes status or breastfeeding outcome.
Instead, we found that in all cases of infant hypoglycemia, formula was given at some point during the hospital stay, none of the women whose infants had hypoglycemia was able to meet their intention to exclusively breastfeed, and this disparity persisted past the time of hypoglycemia risk. These results support the findings of a 2022 systematic review by Cummins et al., which identified neonatal hypoglycemia as a main reason for in-hospital formula supplementation among women with GDM. 12 With questions surrounding the long-term effects of asymptomatic hypoglycemia 33 and with known long-term benefits of breastfeeding, protection of breastfeeding should be a chief consideration in future evidence-based guidelines for asymptomatic hypoglycemia in newborns. Studies suggest that strategies involving the use of oral dextrose gel, 34 colostrum, 35 or donor milk 36 may reduce NICU admissions and support EBF.
Strengths and limitations
Our study is one of the first, to our knowledge, to compare a wide array of factors related to breastfeeding among women with and without diabetes from pregnancy through 4 weeks after hospital discharge. Furthermore, using data from patients' Electronic Medical Record to obtain breastfeeding outcomes in the hospital increases the validity of our results. This study also has some limitations, including our small sample size of 57 women, which limited our analytical abilities. We had initially intended to separate different types of diabetes, including GDM and pregestational diabetes (type I or type II), into distinct groups, but were unable to do so because of the limited number of participants in each group. In addition, our cohort was recruited from only one hospital center, limiting the generalizability of results.
Conclusion
In our study, women with diabetes had similar prenatal breastfeeding intentions, attitudes, and self-efficacy as those without diabetes, but were less likely to exclusively breastfeed and to meet their own breastfeeding goals by the end of their birth hospitalization. NICU admission and diagnosis of infant hypoglycemia, both of which were associated with diabetes status, may have contributed to the less favorable early breastfeeding outcomes in this population. Future research should focus on identifying strategies to support women with diabetes in achieving their breastfeeding goals, especially in the face of neonatal and postpartum complications.
Footnotes
Acknowledgments
The authors acknowledge Taryn Donavan, Tessa Kehoe, and Christine Henry for their contributions to participant enrollment and data collection.
Authors' Contributions
K.N.D. and S.N.T. conceived of and designed the study and collected data. K.N.D. analyzed the data. D.A. wrote the initial draft of the article. K.N.D., S.N.T., and D.A. reviewed and edited the article. A.A.M. provided essential assistance with participant recruitment and data collection.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a grant from the Allen Foundation (Grant # G-406). This publication was made possible by CTSA Grant Number UL1 TR001863 from the National Center for Advancing Translational Science (NCATS), a component of the National Institutes of Health (NIH) and NIH Grant T35DK104689.